
Abstract
Abstract
Introduction:
Use of a Fogarty catheter for emergent occlusion of tracheoesophageal fistulas (TEFs) has been described for use in unstable neonates. Our purpose was to describe a case series of elective Fogarty catheter occlusion of the TEF.
Materials and Methods:
A formal operative laryngoscopy and rigid bronchoscopy were performed with Fogarty catheter placement into the fistula before surgical intervention. The balloon was inflated and gentle traction provided occlusion of the tract. An endotracheal tube was then placed in a midtracheal location irrespective of fistulous tract location. The Fogarty catheter was removed at the time of fistula ligation.
Results:
Six patients underwent Fogarty catheter occlusion of the TEF at the time of repair. The average gestational age was 38 ± 2 weeks and birth weight was 2499 ± 399 g. Associated anomalies or comorbidities were present in 2 of 6 patients (33%). Five patients (83%) had an esophageal atresia with distal TEF, all of whom underwent surgical intervention before day of life (DOL) 2. Of these patients, 3 were performed thoracoscopically, 1 was converted from thoracoscopic to open, and 1 was initiated as an open procedure. One patient had an H-type fistula, which was repaired through a cervical approach on DOL 48. Average time required for both bronchoscopy and Fogarty placement was 10 ± 2 minutes. There were no complications associated with Fogarty catheter placement and catheter dislodgement did not occur during any of the procedures.
Conclusion:
Elective Fogarty catheter occlusion of TEF can be performed safely and expeditiously, alleviating many perioperative challenges of TEF.
Introduction
T
Some authors have described the use of Fogarty balloon occlusion in unstable patients or in cases in whom the fistula may be difficult to identify, as in H-type fistulas and reoperative procedures.6–8 There have only been 2 case reports in 1995 and 2007 describing the elective use of Fogarty catheters in the repair of TEFs. Both of these articles describe the benefits of this technique, including reduction of aspiration and improved ventilation. Our purpose was to describe a case series in which routine elective occlusion of the TEF with Fogarty catheter was performed before operative repair and to evaluate the import of this method in TEF repair.
Materials and Methods
Data collection
After obtaining IRB approval (IRB14-00732), a retrospective review of patients who underwent TEF repair with coinciding laryngoscopy, rigid bronchoscopy, and Fogarty catheter placement was performed. Between the dates of January 1, 2014 and September 30, 2014, 6 patients were identified. Data collection included demographics, comorbidities, age at operation, operative times for bronchoscopy and Fogarty placement, and complications.
Surgical management
To fully evaluate the airway, patients underwent awake fiberoptic laryngoscopy in the Neonatal Intensive Care Unit to evaluate the dynamic airway and document vocal cord motion. At the time of surgery, all procedures were initiated with formal laryngoscopy and rigid bronchoscopy. This portion of the procedure was performed under general anesthesia with preservation of spontaneous ventilation, allowing for a complete evaluation of the airway and identification of the fistula location, evaluation of degree of tracheomalacia, palpation of larynx to evaluate for laryngeal cleft, and identify any concomitant anatomical airway abnormalities. A Fogarty catheter (3F–5F) was then deployed under direct vision into the fistulous tract and inflated with 1 mL of air (Fig. 1). Gentle traction was applied to the catheter until the balloon was visible as a bulge in the posterior tracheal wall to ensure occlusion. The catheter was secured to the patient's cheek on the same side as surgical approach, allowing for expeditious removal at the time of fistula ligation. The trachea was then intubated with the tip positioned in the midtrachea, regardless of the location of the fistula. After securing the airway opposite to the side where the Fogarty catheter was secured, line placement and patient positioning were performed with conversion to high-frequency oscillatory ventilation if a thoracoscopic approach was chosen. Standard surgical repair was then undertaken using a thoracoscopic, open, or cervical approach. After observation and isolation of the fistula by the surgical team, the balloon was let down and the Fogarty catheter removed by the anesthesia team at the time of fistula ligation after confirmation by the surgical team.
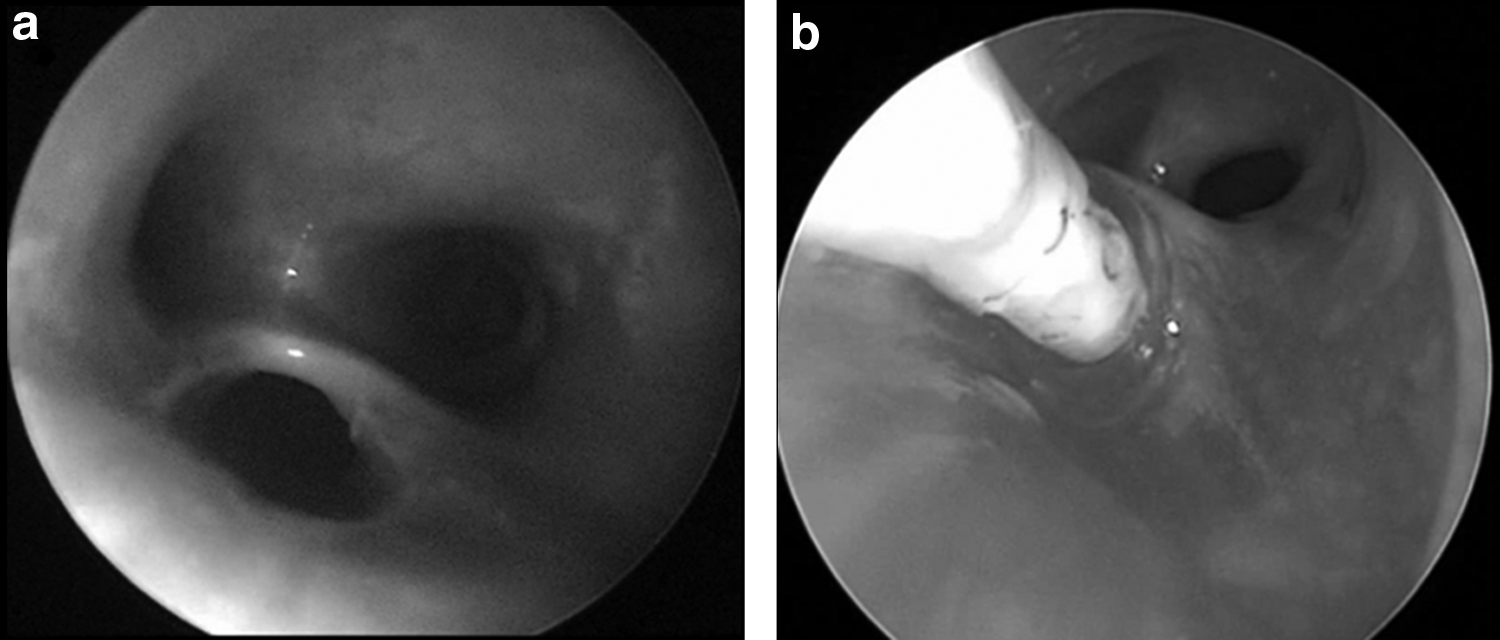
Fogarty catheter insertion.
Results
Patient characteristics
Six patients underwent Fogarty catheter placement at time of operative repair. The average gestational age was 38 ± 2 weeks and average birth weight was 2499 ± 399 g (range 1750–2856 g). There was a male predominance (67%). Of these patients, one had dextroposition of the heart and the remainder had less significant cardiac anomalies (2 with small ventricular septal defects, 3 with small patent foramen ovales). One patient had significant congenital anomalies, including anal stenosis, patent urachus, renal dysplasia with renal failure, and malrotation.
Five patients had esophageal atresia with distal TEF (gross classification type C) and 1 patient had an H-type fistula (gross classification type E). The 5 patients with distal fistulas were identified on day of life (DOL) 0, whereas the patient with H-type fistula who had multiple congenital anomalies was diagnosed at DOL 33 and repaired on DOL 48.
Operative data
All 5 patients with type C TEF underwent surgery before DOL 2, whereas the patient with H-type fistula was repaired on DOL 48. Three of the 5 patients underwent successful thoracoscopic repair. One patient required conversion to open for hemostasis and observation. One patient underwent a planned open approach and the remaining patients underwent repair through a cervical approach (H-type fistula). The average time for bronchoscopy was 10 ± 2 minutes and the average Fogarty catheter size was 4F ± 1F. In 2 patients, moderate tracheomalacia was identified, 1 of whom required aortopexy at a later date because of recurrent hypoxic events. No further anomalies, including laryngotracheal cleft or vocal cord paralysis, were identified. There were no complications from bronchoscopy or Fogarty balloon placement, including dislodgement, injury to the airway or fistula, or bleeding.
Discussion
Fogarty catheter placement to facilitate TEF repair has been described in majority of publications as a rescue technique during the preoperative period to prevent further damage to the lungs from aspiration, prevent gastric dilation, or to improve ventilation in unstable patients with large fistulas.6–10 In cases in whom identification of the fistula may be difficult, such as reoperative procedures or H-type fistulas, the use of both Fogarty catheters and a guide wire has been reported. 11 The elective use of this technique is less well documented, but two case reports have discussed its potential to minimize risks of aspiration events and hypoventilation during surgical repair.12,13
The most significant advantage of this approach is the ability to control the fistula early. This occlusion prevents shunting of the ventilation that may result in hypercapnia and gastric distention. These effects may be beneficial in both minimally invasive and open approaches, as previous data suggest that ineffective ventilation occurs in up to 16% of open cases. 10 Routine bronchoscopy is already used by many surgeons to identify the location of the distal fistula, evaluate for a proximal fistula, and document other anatomic abnormalities such as tracheal clefts and tracheomalacia. For those surgeons who routinely perform bronchoscopy, addition of Fogarty placement would add minimal time to the operative procedure. Our data suggest that the addition of both bronchoscopy and Fogarty placement would add as little as 10 minutes to the operative time, which may arguably be regained in some patients with increased security that occlusion of the fistula provides. Although traditional teaching attempts to minimize these risks through placement of the endotracheal tube distal to the fistula, at least 11% of fistulas occur at or below the level of the carina, and an additional 23% will be within 1 cm of the carina, rendering this approach unachievable. 14 Fogarty catheterization avoids this concern by early occlusion of the fistula, which allows more ideal anesthetic management and optimal placement of the endotracheal tube for ventilation.
An underappreciated advantage of this routine approach is an opportunity to perform a thorough evaluation of the airway before surgical intervention. Kosloske et al. have previously reported that this routine evaluation can reveal crucial findings that influence operative planning and management in up to 57% of cases. 15 In addition, there is an incidence of nearly 30% of severe associated laryngotracheal abnormalities, requiring surgical intervention that may be identified with this bronchoscopic evaluation. 14 Similarly, 2 of the 6 patients in our study had bronchoscopic findings of tracheomalacia, and 1 patient later required aortopexy because of recurrent hypoxic events. In routinely evaluating the respiratory tract preoperatively, surgeons may gain additional insight into the clinical events that may impact the postoperative period, while also identifying anomalies that may require intervention. In our series, we subjectively noted that identification of the fistula was aided through use of both the bronchoscopy and the Fogarty catheter in identification of the fistula.
One limitation of this study is that it is a single-center, retrospective study. For this reason, it may be difficult to ascertain its applicability to other centers or surgeons. Other centers would require a surgeon adept at interventional rigid bronchoscopy to fully benefit from the approach. In addition, our center uses an oscillating ventilator during many of these cases, which may also decrease the shunting experienced. However, we have noted that this ventilation technique does not mitigate this complication entirely, especially in large fistulas or those located at the carina. In addition, the power of this study is limited by the relative rarity of the condition. With increased number of patients, complications not seen within our study may be encountered.
The operative management of TEF presents many challenges for both the surgical and anesthetic teams. We believe that routine placement of the Fogarty catheter addresses these obstacles by limiting inadvertent ventilation through the fistula, preventing gastric distention and allowing for optimal positioning of the endotracheal tube with minimization of ineffective ventilation for both the thoracoscopic and open approaches. Our study suggests that this technique can be performed safely with minimal addition to the operative time.
Conclusion
Elective Fogarty catheter occlusion of TEF can be performed safely and expeditiously, alleviating many perioperative challenges of TEF and aiding completion of repair through a minimally invasive approach.
Footnotes
Disclosure Statement
No competing financial interests exist.