
Abstract
Abstract
Intro:
Although the use of laparoscopy has significantly increased in colorectal procedures, robotic surgery may enable additional cases to be performed using a minimally invasive approach. We separately evaluated the value of laparoscopic and robotic colorectal procedures compared to the open approach.
Methods:
Patients undergoing nonemergent colorectal operations from 2010 to 2013 with National Surgical Quality Improvement Project data were identified. Robotic and laparoscopic procedures were separately matched (1:1) to open cases. Outcomes included 30-day composite morbidity, length of stay, operative time, and inpatient costs. Frequently used intraoperative disposable items were categorized, and significant cost contributors were identified by surgical approach. Statistical differences were determined with Chi-square and Wilcoxon signed-rank tests.
Results:
Both laparoscopic (n = 67) and robotic (n = 45) approaches were associated with decreased composite morbidity compared to matched open cases (lap vs. open: 22.4% vs. 49.2%, P < .01; robotic vs. open: 6.7% vs. 33.3%, P < .01). Median length of stay was significantly shorter for both laparoscopic and robotic compared to open surgery (lap vs. open: 5 vs. 7 days, P < .01; robotic vs. open: 5 vs. 7 days, P < .01). Median hospital costs were similar between laparoscopic and open surgery ($13,319 vs. $14,039; P = .80) and robotic and open surgery ($13,778 vs. $13,629; P = .48).
Conclusion:
These findings illustrate the value for both laparoscopic and robotic approaches to colorectal surgery compared to the open approach in terms of short-term outcomes and inpatient costs. Advanced intraoperative disposable items such as cutting staplers and energy devices are important targets for additional cost containment.
Introduction
T
Multiple studies have compared outcomes and costs between robotic and laparoscopic colorectal operations and have consistently shown similar outcomes, but increased overall costs in patients undergoing robotic surgery.3,6–8 Thus, when an operation can be completed laparoscopically, the robotic approach is unlikely to add value. Yet, the universal adoption of laparoscopy for colorectal surgery has been slow, and laparoscopic colorectal resections have been associated with higher conversion rates to open surgery than robotic-assisted operations.9–11 Robotic technology may enable certain procedures to be performed with a minimally invasive approach that could not otherwise be performed using the laparoscopic approach either due to disease, patient, or surgeon factors. To determine the value of the robotic approach in these cases, it would be most appropriate to compare outcomes and costs of robotic cases to open colorectal procedures using the laparoscopic approach as a benchmark.
In this study, we set out to evaluate the value of minimally invasive surgery, both robotic and laparoscopic, compared to open procedures. We hypothesized that both laparoscopic and robotic surgery would have benefits in terms of short-term morbidity compared to open surgery. To determine whether this benefit translates to improved value, we performed cost identification so that surgeons and policy makers have a better awareness of the contributors to costs, and therefore, the value of minimally invasive surgery.
Methods
Study design
We performed a retrospective single institution cohort study of patients who underwent nonemergent colorectal resections from January 2010 to June 2013. Patients, as well as preoperative factors and postoperative outcomes, were identified using American College of Surgeons National Surgical Quality Improvement Program (NSQIP) data. NSQIP data were merged with information on financial outcomes from the hospital decision support system. The validity of NSQIP data has been previously described. 12 The study protocol was reviewed and approved by the local university institutional review board with waiver of informed consent.
Colorectal procedures included hemicolectomy, total abdominal colectomy, proctectomy, and total proctocolectomy and were defined using administrative CPT codes. To make more adequate comparison groups between minimally invasive and open procedures, we identified open procedures that could be considered candidates for minimally invasive surgery using preoperative criteria that were developed for the purposes of this study. Patients were not considered a candidate for minimally invasive procedures if they had ever undergone previous open abdominal surgery, undergone >3 laparoscopic abdominal procedures, or if their disease process precluded minimally invasive approach such as in obstruction from cancer or bowel perforation with diffuse contamination. Medical Chart review was performed to verify surgical approach. Patients with incomplete financial information were excluded from the study. Laparoscopic and robotic cases were separately matched (1:1) to open cases determined to be candidates for MIS based on procedure type, indication (neoplasm, diverticulitis, inflammatory bowel disease, and other nonemergent lower gastrointestinal tract complications or disorders), and body mass index (BMI) within 4 U.
Clinical outcomes
NSQIP complications were grouped to define 30-day postoperative outcomes. 13 Our primary outcome of interest was an overall composite morbidity that included any complication. Surgical site infection included superficial surgical site infection, deep surgical site infection, organ space surgical site infection, and wound disruption. Sepsis included postoperative sepsis and septic shock. Urinary tract complications included acute renal insufficiency, acute renal failure, and urinary tract infection. Respiratory outcomes included pneumonia, unplanned intubation, and ventilation greater than 48 hours. Venous thromboembolism included postoperative deep venous thrombosis or pulmonary thromboembolism. Cardiac complications included myocardial infarction or cardiac arrest. Central nervous system complications included cerebrovascular accident, coma, and peripheral nerve injury. Other complications included bleeding/transfusions, unplanned return to the operating room, 30-day hospital readmission, and 30-day mortality.
Cost analysis
To evaluate the costs of each surgical approach, we first examined total costs, including both variable and fixed costs. Because hospitals vary in the methods and amounts by which fixed costs are distributed across charge items, we also separately examined variable costs that represent the expenditures related to each additional use of a charge item. Costs for the overall hospitalization included those occurring on the day of the operation until the day of discharge. We then identified cost associated with operative expenses (including anesthesia, operative time, and surgical supply). In addition, we identified disposable surgical items that were frequent high-cost contributors. We categorized disposable surgical items and only item categories used in greater than 50% of each surgical approach were included in the item cost subanalysis.
Statistical analysis
Chi-square, fisher exact, and Wilcoxon signed-rank tests were used to determine significant differences in financial and clinical outcomes. All univariate and bivariate statistics were calculated using SAS version 9.4 (SAS Institute). Matching was completed using R statistical package matching software (Match). Graphing was performed using R package ggplot2. 14 Statistical significance was set at alpha 0.05 for all tests.
Results
Of 291 patients undergoing open colorectal surgery, 153 (52.6%) met study criteria as potential candidates for minimally invasive surgery. We successfully matched 112 (73%); 67 to patients undergoing laparoscopic surgery and 45 to patients undergoing robotic surgery (Table 1). After matching, patients undergoing laparoscopic and open procedures had largely similar demographic and risk factors. Patients undergoing robotic procedures were similar to matched open cases except for significantly lower number of males and higher rates of previous abdominal surgery. The majority of matched robotic procedures were for rectal resections, whereas the majority of matched laparoscopic cases were performed for colon resections.
COPD, chronic obstructive pulmonary disease; SIRS, systemic inflammatory response syndrome; APR, abdominal perineal resection; LAR, low anterior resection; LHC, left hemicolectomy, RHC, right hemicolectomy; TAC, total abdominal colectomy, TPC, total proctocolectomy.
In both matched groups, the minimally invasive approach was associated with decreased overall composite morbidity (Lap vs. Open: 22.4% vs. 49.5%, P < .01; Robotic vs. Open: 6.7% vs. 33.3%, P < .01) (Table 2). For laparoscopic cases compared to matched open cases, there were significantly fewer surgical site infections and bleeding/transfusion events. Median operative time was significantly longer in robotic compared to open (4.2 vs. 3.4 hours; P = .01) matched groups, but was similar between laparoscopic and open groups (2.8 vs. 2.8 hours; P = .44) (Fig. 1). Median length of stay was significantly lower in the laparoscopic compared to matched open cases (5 vs. 7 days; P < .01) and for robotic compared to matched open cases (5 vs. 7 days; P < .01) (Fig. 2).
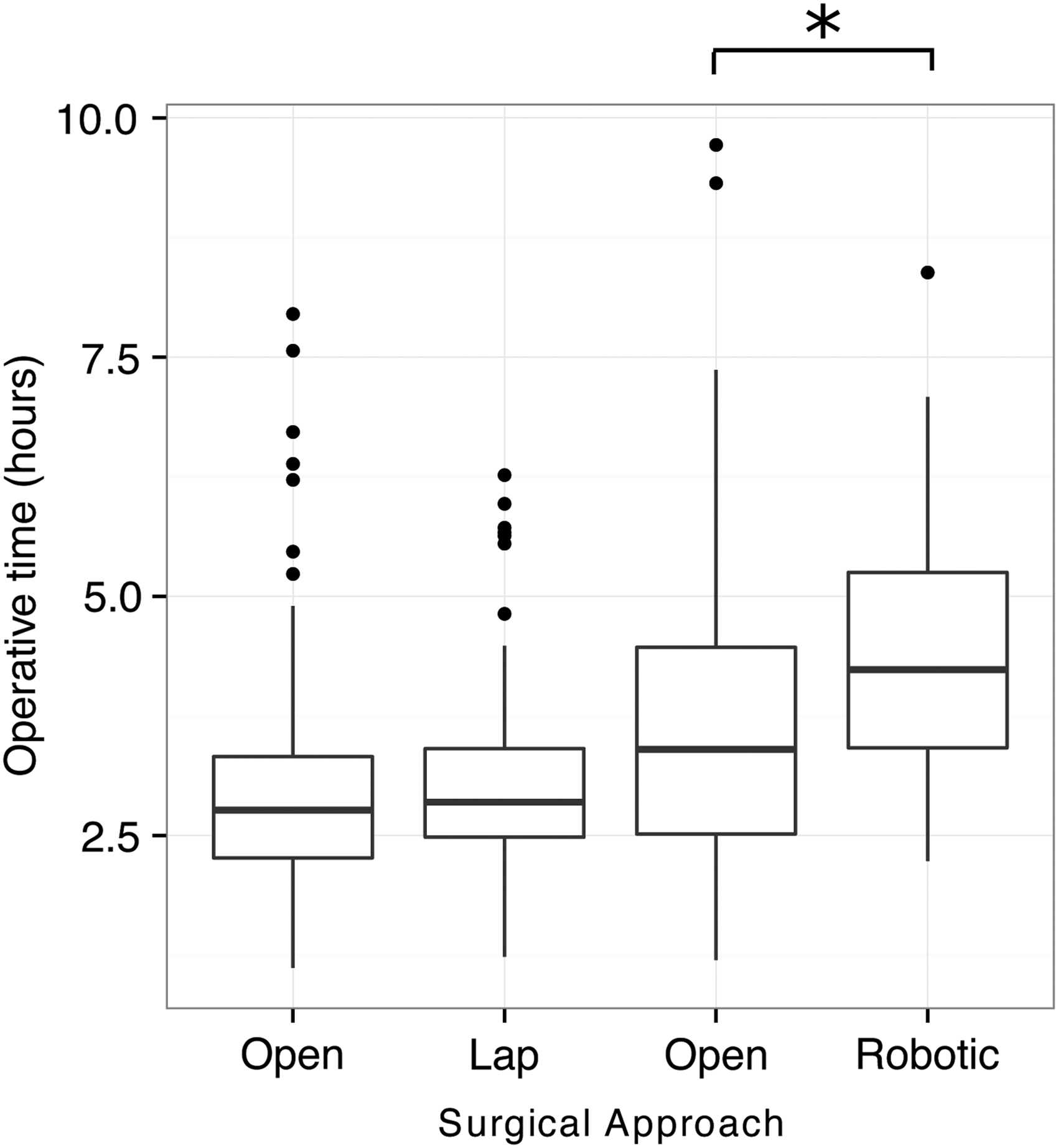
Operative time by surgical approach in matched groups; *P < .01.
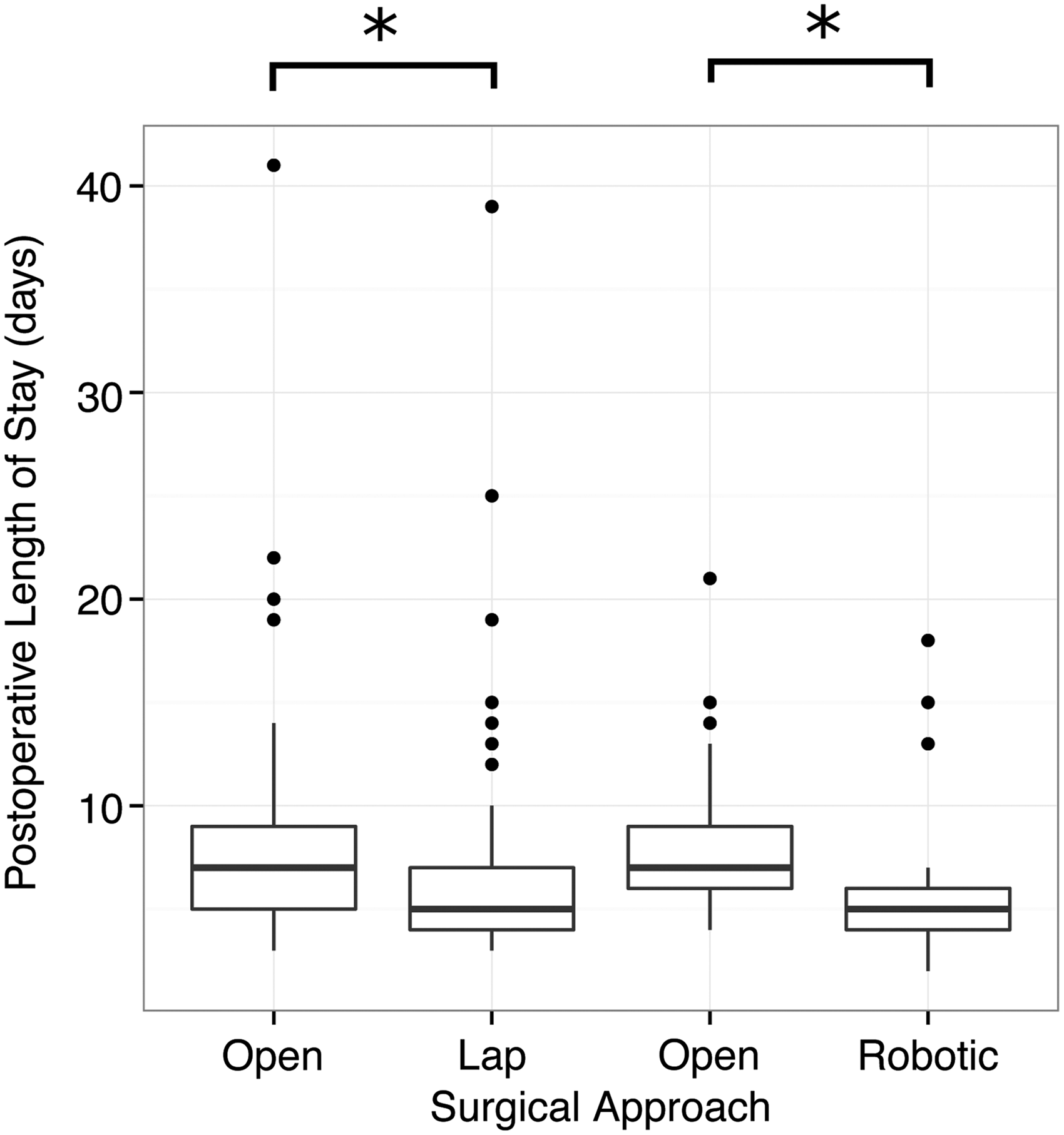
Postoperative length of stay by surgical approach in matched groups; *P < .01.
VTE, venous thromboembolism.
Median overall hospitalization costs were similar between both laparoscopic and matched open patients ($13,319 vs. $14,039; P = .80) and between robotic and open matched groups ($13,629 vs. $13,778; P = .80) (Table 3). To identify the different drivers of costs, we separated costs attributable to operating expenses and further to disposable surgical supply costs. For robotic but not laparoscopic matched cases, there were significantly higher total costs associated with both operative expenses ($9,572 vs. $7,297; P < .01) and surgical supply ($4,861 vs. $2,660; P < .01).
Overall, hospitalization includes all costs from day of operation to discharge, including operative expenses.
Operative expenses include anesthesia, operative time, and surgical supply costs.
Given significant differences in cost of surgical supply, we sought to identify the disposable items that significantly contributed to the intraoperative cost in each surgical approach. Table 4 lists median variable costs for surgical disposable item categories that were used in greater than 50% of cases of each surgical approach. Items related to advanced technologies accounted for the highest surgical supply costs: cutting staplers, Seprafilm, and energy devices. Comparison of costs between operative approaches was limited due to different frequency of use, but did reveal significantly higher costs of staplers in robotic cases. A composite of surgical packs and dressing supplies had increased costs in both laparoscopic and robotic cases compared to open cases. The median cost of energy devices was higher in laparoscopic cases compared to matched open controls. Laparoscopic and robotic approaches had lower costs of sutures and clips compared to open cases; however, this was a very small contributor to costs compared to other items.
Discussion
In this study, we separately evaluated the value of laparoscopic and robotic approaches compared to open colorectal surgery. Overall, 30-day composite morbidity and length of stay were significantly lower in both minimally invasive approaches compared to matched cases undergoing open surgery. Overall, inpatient cost was similar in laparoscopic cases compared to matched open procedures, as well as for robotic and matched open procedures. Intraoperative costs were significantly higher in the robotic compared to open surgeries with advanced disposable items, including cutting staplers and energy devices, as well as surgical packs contributing to the cost difference. Together, these findings provide targets for cost containment and illustrate that both laparoscopic and robotic approaches have value by virtue of improved short-term outcomes with equivalent inpatient costs compared to open colorectal surgery.
Several randomized trials have supported short-term outcome advantages with laparoscopic compared to open colorectal surgery;15,16 however, only a few retrospective studies have compared short-term outcomes between robotic and open approaches. For colorectal resections, the robotic approach has been consistently associated with decreased time to bowel function and length of stay, but with longer operating time compared to open surgery.4,17–21
In addition, the robotic approach has been associated with decreased blood loss, improved postoperative physical functioning, decreased surgical site infections, and decreased postoperative pain. 18 In our study, the majority of laparoscopic and matched open cases were performed for colectomy, whereas the majority of robotic resection was performed for rectal resections. For these procedures, our findings support the enhanced quality of both the laparoscopic and robotic approaches compared to open surgery in terms of short-term morbidity and length of stay.
Although we found similar inpatient costs between laparoscopic and open surgical approaches, recent studies have supported that patients undergoing laparoscopic colorectal surgery have decreased total hospital cost compared to patients undergoing open surgery.3,22 These savings in laparoscopic surgery have been attributed to decreased length of stay, but can be significantly affected by postoperative morbidity. 23 We did note a trend for lower median overall costs in laparoscopic cases, and our study had a smaller sample size compared to these prior studies comparing laparoscopic and open approaches. For robotic colorectal surgery, two studies, one Italian unmatched study and one smaller Canadian unmatched study, have reported higher total costs compared to open surgery.21,24 While the additional fixed and indirect costs related to the purchasing, maintenance, and depreciation of robotic platforms are significant cost contributors, the amount that these additional costs add to each operation will vary by center volume. This study illustrates similar total costs between robotic and open operations at our institution and is the first to highlight frequent, high–cost, intraoperative disposable items that surgeons can additionally target for improving costs. 25
The focus of our article was to understand the value of robotic surgery to enable more cases to be performed using a minimally invasive approach, not as a replacement for a laparoscopic approach. As such, we purposefully did not compare robotic and laparoscopic costs in a matched case approach, and the structure of our matching does not allow for direct comparison between these two approaches. The robotic group differed from the laparoscopic group in that the robotic operations were more complex, as the majority was rectal resections and included total proctocolectomies. Prior studies have consistently shown similar outcomes, but higher costs with the robot compared to laparoscopic surgery.3,6–8 Indeed, a large multicenter randomized trial is underway to compare short-term and long-term outcomes for the laparoscopic versus robotic approach for rectal surgery. 26 However, despite a significant rise in minimally invasive surgery for colorectal disease, only 50% of colectomies were performed using the laparoscopic approach in 2010.3,27 Our results suggest that in colorectal cases where a robotic approach can increase the likelihood of a patient receiving a minimally invasive approach beyond what is currently achieved with standard laparoscopy, robotic surgery can add significant value. Rectal operations requiring dissection within the deep pelvis, as were the majority of robotic operations included in this study, are likely where the robot offers the greatest advantages to surgeons.
This study has several limitations, including its retrospective design and small sample size. Patients were matched on operative indication, procedure type, and BMI, yet there were small, but significant differences in gender and frequency of prior abdominal surgery in robotic and open cases. Although open cases were determined to be candidates for minimally invasive surgery based on specified criteria for this study, this does not readily translate that they could have actually been performed using a minimally invasive approach. We were unable to specify the exact contribution of purchasing, maintenance, and depreciation of operative equipment, including laparoscopic and robotic platforms, although these costs are indirectly accounted for in our total costs for each case. The cost of disposable items, operative time, and hospital stay among other items is unique to each hospital and our estimates may not be generalizable to all centers. Furthermore, several robotic laparoscopic instruments are reusable for only a limited number of cases, and we may underestimate the variable supply item cost of these endoscopic tools. However, the costs of these reusable instruments are indirectly accounted for in our analysis of total intraoperative costs that includes fixed costs. Finally, this study did not assess oncologic or long-term outcomes. Although the appropriateness of laparoscopy in treatment of colon cancer is well supported, recent trials in rectal cancer have questioned the role of laparoscopy for achieving adequate oncologic margins compared to open resections.28–30 However, the robotic approach may offer distinct advantages for rectal cancer resections and whether these pathologic results lead to long-term outcome differences has not yet been determined.
Conclusions
Patients undergoing laparoscopic and robotic colorectal surgery had decreased 30-day composite morbidity and length of stay compared to matched cases undergoing open colorectal surgery. Inpatient costs were similar in laparoscopic and robotic cases compared to open surgeries. Advanced disposable items, including cutting staplers, energy devices, as well as surgical packs, are frequent high-cost contributors to intraoperative costs. These findings support that laparoscopic and robotic approaches have value compared to the open approach in colorectal surgery, and additional targets for intraoperative cost containment are provided.
Footnotes
Acknowledgments
R.H. Hollis is supported by grant T32 CA091078-13 from the National Institutes of Health. The authors thank Fred Horton for assistance in obtaining financial data for this study.
Disclosure Statement
No competing financial interests exist.