
Abstract
Abstract
Background:
The inferior mesenteric artery (IMA) is usually divided during the resection of sigmoid colon and rectal cancers. However, this sometimes results in a vein (SRA\V) insufficient blood supply to the anastomosis, leading to anastomotic leakage. We summarized the experience of laparoscopy surgery approach to perform the D3 lymph node dissection with preserving the superior rectal artery and vein.
Methods:
Our method involves peeling off the vascular sheath from the inferior mesenteric vessel to the superior rectal vessel and dissection of the lymph node around the IMA together with the sheath. The feasibility outcomes of the technique were evaluated in 36 cases of laparoscopic resection of sigmoid and rectal cancer.
Results:
Our method involves peeling off the vascular sheath from the inferior mesenteric vessel to the superior rectal vessel and dissection of the lymph node around the IMA together with the sheath. The feasibility of the technique was evaluated in 36 consecutive cases of laparoscopic resection of sigmoid and rectal cancer. Patients with sigmoid or rectal cancer underwent operation via the present laparoscopic approach. No serious complications related to the approach were encountered. The number of cleared lymph nodes was 17 (range 10–35). The operation time was 200 (range 160–300) minutes. The blood loss was 50 (range 20–100) mL. Anastomotic leakage never occurred in these patients without preoperative chemoradiation therapy, the patients had quick convalescence, as evaluated by the recovery of flatus passage (2.8 ± 1.5 days), postoperative hospitalization (10.8 ± 4.6 days), degree of postoperative pain for 48 hours (2.5 ± 0.5, visual analog scale), duration of postoperative ambulation (1.5 ± 0.5 days), and drainage tube removal time (1.0 ± 0.4 days).
Conclusion:
Our method allows equivalent laparoscopic lymph node dissection to the preservation of the SRA\V technique without excessive operative time, complications, or bleeding. It seems to be a promising and feasible technique for these patients with sigmoid and rectal cancer.
Introduction
I
However, the optimal level of vascular ligation of the IMA in left-sided colon and rectal cancer surgery remains controversial with regard to anatomical, technical, and oncologic perspectives. Several experts prefer a technique of lymph node dissection up to the root of the IMA and low ligation, with preservation of the IMA and left colic artery (LCA). The other surgeons intend to dissect the same to the root of the IMA instead of the low ligation, without preservation of the left colic and supper rectal artery, because they believe that communicating branched vessels are formed between inferior rectal artery, middle sacral artery, and superior mesenteric artery in the left colon intestinal wall. Unfortunately, the most considerable complication in sphincter-saving operation for cancer of the rectum is anastomotic leakage, which has been reported with an incidence of 3.3%–8.3% approximately,3,4 especially in old patients with cerebrovascular disease and atherosclerotic vessels. In addition, once it does happen that may result in intra-abdominal sepsis. It is universally acknowledged that the original reasons for the anastomotic leakage are the intestinal blood supply and the anastomotic tension.
Although there is still controversy on which location is beneficial to divide the artery during distal colorectal cancer resection, preservation of the LCA may result in an improved blood supply to the proximal cut end of the sigmoid colon. 5 Ischemia at the distal cut end may also occur, because blood is supplied to the long distal limb only from the anal side when the IMA or the superior rectal artery (SRA) is divided. Therefore, when the IMA\V-LCA\V-SRA\V axis is preserved, the blood supply to the distal limb can be maintained better, which may in turn decrease the incidence of anastomotic leakage. Although Kobayashi et al. 6 had attempted to preserve the SRA to maintain the blood supply to distal sigmoid colon, the approach to preservation of upper rectal artery has not been reported. Thus, we probably present a feasible and secure method to dissect the lymph nodes around the IMA with preservation of the IMA\V, LCA\V, and SRA\V axis in laparoscopic sigmoid and rectal cancer resection.
Materials and Methods
Patients and methods
Patient information
From January 2014 to January 2015, we prospectively collected the results of 36 consecutive, curatively operated cases of sigmoid colon and upper rectal cancer (Table 1). All cases were staged preoperatively by colonoscopy, enhanced computed tomography (CT), or nuclear magnetic resonance imaging (MRI) for the patients who cannot use the enhanced CT scan. The method of lymph node dissection was decided preoperatively according to the stage of the individual case. Lymph nodes around the IMA were dissected but the IMA, LCA, and SRA were preserved. The operative time, estimated blood loss, intra- and postoperative morbidity, and number of dissected lymph nodes in these patients were estimated. Written informed consent was signed by every patient, who had been told possible procedure-related benefits and risks (including possible complications and corresponding managements). The Institutional Review Board of Xinjiang Tumor Hospital approved this protocol.
ASA, American Society of Anesthesiologists; BMI, body mass index.
Surgical technique
Patients were laid in head-down position during the laparoscopic procedure. The lymph nodes were dissected after mobilizing the sigmoid colon with a medial to lateral approach. First, the root of the IMA was exposed by the gauze strip to isolate the small intestine to the level of the duodenum and the vascular sheath of the IMA was dissected to expose the tunica adventitia of the IMA. A loose fascial space exists between the vascular sheath and the tunica adventitia, so once the surgeon accesses to the layer, it is easy to peel off the vascular sheath with the ultrasonic harmonic scalpel, and the lymph nodes are then detached from the IMA together with the vascular sheath. The vascular sheath is peeled off down to the bifurcation of the LCA and continuously the dissection is extended toward the SRA. The ligation is advanced along the level from where the LCA crosses the IMV up to the sigmoid branch artery. Furthermore, the method for vein disposal is from the anal side of the SRA. Finally, the sigmoid mesentery is transected from the root of the IMA to the IMV, and en bloc dissection of the lymph nodes around the IMA is completed. During these procedures, care should be taken to preserve the left hypogastric nerve. There are some key points related to nerve injury during laparoscopic radical resection for rectal cancer. Meticulous hemostasis and adequate tension are critical to maintaining good visualization of the operative field in laparoscopic surgery. Hypogastric nerve has close relationship with the upper part of the rectum. Incorrect operation in the pelvic parietal peritoneum during dissection of upper rectum will lead to nerve injury. When the IMA was lifted, the angle was gradually revealed between the IMA and abdominal aorta. When performing dissection of IMA, bilateral nerve tracts should be pushed to the posterior abdominal wall and anterior fascia of the abdominal aorta should be well protected to avoid nerve injury. Conventional blunt dissection is not recommended in the procedure. Intestinal anastomosis is used by double stapling (Figs. 1 and 2).
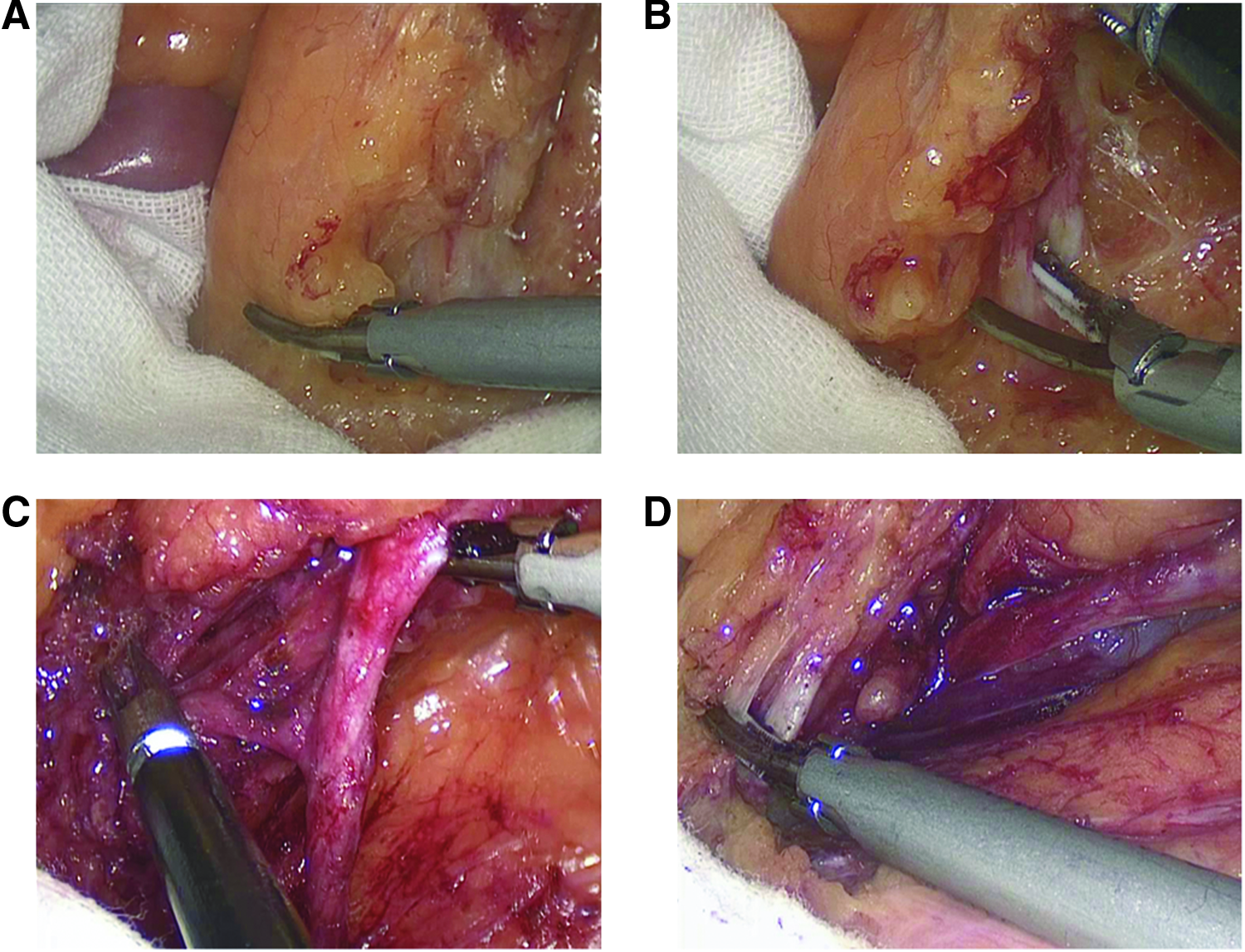
Operative technique (part 1).

Operative technique (part 2).
Perioperative managements
Patients who underwent general anesthesia resumed water and soft diet gradually 12 hours after surgery. Patients were observed for any signs of fever, abdominal pain, abdominal distension, and peritonitis. Prophylactic antibiotics were applied, and stool was softened for patients. Epidural analgesia and nonsteroidal anti-inflammatory drugs were not being used during the perioperative period. Using nasogastric tubes and anal canal as anti-ileus strategies can be circumvented if the patients' ambulation took place, both of which were routine procedures in this study.
Complications
It is worth highlighting the fact there is no highly sensitive radiological modality for detecting anastomotic leak. We usually did physical examination for the patients during the operation, such as the insufflation leak test. After the operation, the complaints of the patients and their symptoms and signs could give us clues about complications. In turn, poor postoperative recovery, patient looking unwell with tachycardia, fever, and leukocytosis should raise the alarm. When complications were suspected, we did X-ray, B ultrasound, or CT for patients to make a confirmed diagnosis.
Data collection and analysis
All the clinic pathological data of the cases were collected and analyzed using a statistical description approach.
Results
All patients who successfully completed the surgery underwent lymph node dissection as scheduled. The characteristics of the patients are shown in Table 1. The results were median operation time 200 (range 160–300) minutes, intraoperative blood loss 50 mL (range 20–100), anastomotic leakage never occurred in these patients without preoperative chemoradiation therapy, the patients had quick convalescence, as evaluated by the recovery of flatus passage (2.8 ± 1.5 days), postoperative bed activity time (1.5 ± 0.5 days), postoperative hospitalization (10.8 ± 4.6 days), degree of postoperative pain for 48 hours (2.5 ± 0.5, visual analog scale), drainage tube removal time (1.0 ± 0.4 days). Postoperative pathologic staging was T2N0M0 in 4 cases, T3N0M0 in 12 cases, T3N1M0 in 12 cases, and T4aN1M0 in 8 cases. The median number of lymph nodes was 17, the specimens' cut edge and circumferential resection margin (CRM) were negative. All the patients received follow-up for 2 weeks; two cases of diarrhea and two cases of pneumonia occurred during postoperative. No serious complications related to the approach were encountered, such as incision infection, abscess, bleeding, anastomotic fistula, thrombosis, and deaths (Table 2).
Discussion
Lymph node involvement is a major prognostic factor for survival after colorectal cancer surgery, which advocated the importance of pathologic examination of 12 or more nodes, 7 especially in stage II colorectal cancer. 8 Moreover, it has been explicitly proved that D3 lymph nodes should be performed in advanced colorectal cancer, including the central lymph nodes with a metastasis rate of 0.3%–8.6%. 9
Two potential risks exist in performing SRA\V-preserving colon resection: leaving residual lymph nodes and disseminating metastatic lymph nodes that affect the number of harvested lymph nodes and postoperative survival. Several groups have discussed the significance of thorough lymph node dissection up to the root of the IMA. They indicated that the 5-year survival rate of patients who had lymph node metastasis around the IMA but underwent lymph node dissection up to the root of the IMA was as good as 40%. In laparoscopic surgery, we use the technique of lymph node dissection around the IMA with preservation of the vessel of the IMA\V-LCA\V-SRA\V axis. The dissected median numbers of the lymph nodes were up to the above principle. Furthermore, Wakahara et al. 10 reveal that sigmoidectomy with SRA preservation can be performed without compromising the quality of lymph node dissection and relapse-free survival.
In addition, controversies exist on the level of arterial ligation in rectal cancer surgery. From oncologic considerations, many surgeons apply high tie arterial ligation (level of the IMA). Other strategies include ligation at the level of the LCA (low tie). In contrast, the drawbacks of the high ligation have been proven to decrease perfusion and innervation of the proximal limb, which would affect the distal colon blood supply. Furthermore, Lange et al. 9 indicated that low tie is preferred over high tie at the level of arterial ligation in rectal cancer surgery through systematic review. Recently, Guo et al. 11 state that low ligation with apical lymph node dissection in rectal cancer treatment provides better anastomotic blood supply but is not associated with differences in node retrieval rate or operation time through a clinical trial. It seems to be that preservation of the LCA has been a favorable procedure for lower colorectal cancer surgery, whenever possible, to maintain the blood flow to the proximal cut end of the sigmoid colon.
Moreover, it is difficult to ascertain the exact cause of bowel necrosis that may not have been directly caused by high ligation. On the basis of a study by Tsujinaka et al. 12 , it can be concluded that proximal bowel necrosis after high ligation is potentially fatal, and the predictive factors of this complication include advanced age, cerebrovascular disease, atherosclerotic vessels, and hypertension. The ideal method to intraoperatively assess viability of the bowel has not yet been developed. In addition, it is well known to surgeons that the bowel distal to the anastomosis is at risk for ischemia when the SRA is divided below Sudeck's critical point. 13 Herein, we determine to provide a safe method with preserving intact the LCA\V-IMA\V-SRA\V axis to guarantee well-perfused anastomotic limbs and prevent anastomotic ischemia according to individual patient's risks.
Blood supply to the anastomotic site is important for preventing anastomotic leakage. Preservation of the IMA\V-LCA\V-SRA\V axis may be important in achieving this, as it could integrally maintain blood flow to the distal sigmoid colon and upper rectum, especially after surgery for proximal sigmoid colon cancer in which the long distal limb is retained. In cases of lower sigmoid colon cancer or upper rectum, preservation of the axis is extremely complicated because it bifurcates, forming small arteries in the mesorectum and broken easily due to the thin wall of the vein. Tocchi et al. 14 conducted a randomized controlled trial and reported a significantly lower rate of anastomotic leakage after left colectomy for diverticular diseases in the SRA-preserving group than in the non-SRA-preserving group.
Our experience showed that preservation of the SRA\V-LCA\V-IMA\V axis for the sigmoid and rectal cancer is not only feasible but also of benefit to patients. Significant symptom improvement with no serious postoperative complications was observed. Preservation of the SRA\V-LCA\V-IMA\V axis has several advantages over laparoscopic colectomy. (1) It can be applied by an entirely laparoscopic approach. The whole procedure can be completed in a laparoscopic manner. (2) The maintenance of vessel integrity and the free tension of the colonic segment proximal to the anastomotic result in adequate anastomotic blood flow to rapid healing, with relatively low anastomosis leakage. In particular, old patients with risk factors, such as cerebrovascular disease and atherosclerotic vessels. Although a complete preservation axis was intentionally performed in 36 patients in the current study, no patient developed infectious complications. (3) It is apt to determine intraoperatively at which point the bowel should be optimally transected. Surgeons attempt to transect the bowel where it is oncologically safe as well as being viable. Therefore, it is inevitable to delay the operative time without affecting the incidence of anastomotic leak, on account of unnecessary surgical procedures for a majority of patients, who were subjected to routine extended bowel resection, including mobilization of the splenic flexure for prevention of proximal bowel ischemia. However, there are several limitations in this technique in terms of tension free. It may be challenged that the preservation of the SRA\V-LCA\V-IMA\V axis may inevitably limit the pull down of the proximal bowel segment to the low pelvic level to facilitate a tension-free colorectal anastomosis and thus paradoxically increase the risk of anastomotic leakage. So far, we found that such a technique should be applied to the upper rectal and sigmoid cancer instead of low location cancer.
To our knowledge, how preservation of blood flow could contribute to improvement of the leakage rate without compromising oncological results remains unclear. This is the first report about the preservation of IMA\V-LCA\V-SRA\V axis in sigmoidectomy or rectectomy. Laparoscopic lymph node dissection around the IMA preserving the root of the IMA and LCA was feasible by our method, without compromising operation time, blood loss, operative safety, or the number of harvested lymph nodes. However, the advantage of the IMA\V-LCA\V-SRA\V axis-preserving procedure should be further assessed in intraoperative techniques for assessing anastomotic blood supply; laparoscopic perfusion assessment with Pinpoint™ system (Novadaq) could provide surrogate information on the blood supply of an anastomosis.
Actually, although it is more difficult to dissect out veins than arteries, there are some tips for attention. Since the distal of IMV is adjacent to that of IMA closely, or even overlapping, procedures were performed with maintaining the tension through traction, with attention for distribution and location of the venous. In our opinion, we should adopt the particular sequence that the vein can be easily dissected out from the distal end to the proximal end.
Conclusions
In conclusion, sigmoidectomy and rectectomy with preservation of the IMA\V-LCA\V-SRA\V axis can be performed for sigmoid and rectal cancer without sacrificing the quality of lymph node dissection. It is noteworthy that there was no anastomotic leakage among the 36 patients undergoing SRA\V-preserving surgery. The advantage of the IMA\V-LCA\V-SRA\V-preserving procedure should be further assessed by intraoperative imaging, which will be subsequently transanal, to assess mucosal perfusion of the completed anastomosis and affirmed by a randomized control study.
Footnotes
Acknowledgment
We thank other members of the Department of Gastroenterological Surgery, Affiliated Tumor Hospital, Xinjiang Medical University, who did not contribute directly to this review but gave valuable advice throughout the study.
Disclosure Statement
No competing financial interests exist. L.G. and H.J.W. conceived and designed the study. H.J.W., Z.L.Z., and Q.S.W. performed the experiment and contributed to the acquisition of data. C.L. revised the statistical analyses. L.G. wrote the manuscript. All authors read and approved the final manuscript.