
Abstract
Abstract
Introduction:
Although laparoscopic cholecystectomy is currently the standard treatment for benign gallbladder pathologies, some cases still require conversion to open cholecystectomy. Since open cholecystectomy has a significantly higher morbidity rate and a lengthier stay in the hospital compared with laparoscopic surgery, predicting this conversion would grant a great advantage in the management of cholecystitis. Therefore, in this study, we aimed to develop a predictive statistical model.
Materials and Methods:
Between August 2006 and January 2011, 1335 laparoscopic cholecystectomies were initiated at the General Surgery Department of Hacettepe University. One hundred four of these cases were started as laparoscopic surgeries, but converted to open cholecystectomies. In our study, we randomly chose 104 laparoscopically completed cases and compared them with the 104 converted cases. We used 31 parameters, including demographics, ultrasonographic findings, and laboratory values, to compare groups. These parameters were later included in a logistic regression analysis to create a statistical model that predicts conversion to open cholecystectomy.
Results:
Among the 1335 laparoscopically started cases, 104 (7.7%) were converted to open surgery. In our study, we found age, gender, ultrasonographic findings of acute cholecystitis, history of choledocolithiasis, history of abdominal surgery, and alkaline phosphatase (ALP) levels to be significant risk factors. By using a receiver operating characteristic curve, we found that the risk significantly increases after 55 years of age and an ALP over 80 IU/L.
Discussion:
Using four parameters—age, gender, history of abdominal surgery, and ALP—in our statistical model, we were able to predict the conversion from laparoscopic to open cholecystectomy with 70% sensitivity and 79% specificity.
Introduction
L
Surgeries that cannot be completed laparoscopically pose the main challenge. Although laparoscopic cholecystectomy is a relatively safe procedure, it may cause complications such as bile duct injuries, which can have catastrophic consequences. Therefore, it is crucial to stop the laparoscopic procedure before injuries occur, and knowing which cases will be problematic provides an advantage. Most injuries happen because surgeons decide to continue with the laparoscopy instead of converting to open surgery. Although some reports show the conversion rate to be as high as 35%, the generally accepted rate is between 2% and 15%.2–4 With the introduction of laparoscopic subtotal cholecystectomy (LSTC), there seems to be a decrease in the number of conversions. 5 Regardless, LSTC is a relatively new technique, and many surgeons still decide to convert to open surgery.
Several preoperative factors have been associated with a higher conversion rate to open cholecystectomy, including older age, male gender, acute cholecystitis, obesity, and a higher leukocyte count. 2 The successful prediction of conversion would allow better planning of surgery time and postoperative accommodations and also help prevent complications due to pneumoperitoneum. Numerous studies have been conducted to predict this conversion rate, including statistical models. To better evaluate conversion factors, we also conducted a retrospective study, which is also performed in this study.
Patients and Methods
Patients
Between August 2006 and January 2011, 1444 cholecystectomies were performed in Hacettepe University General Surgery department. One hundred nine cases were planned as open cholecystectomy and therefore removed from our study. One hundred four cases were converted to open surgery, and we compared these to 104 randomly chosen, laparoscopically completed cases. We performed a retrospective analysis of 31 parameters, including patient demographics, clinical findings, previous treatments, ultrasonography results, laboratory analysis, and intraoperative findings. Demographics and previous treatments included gender, age, body mass index, concomitant systemic diseases, pancreatitis, and choledocholithiasis treatments. Operations on patients receiving choledocholithiasis or pancreatitis treatment were performed 6 weeks after treatment. Clinical findings included fever (body temperature greater than 38°C during admission), upper-right quadrant tenderness on initial physical examination, number of abdominal pain attacks, history of abdominal surgery, and general clinic of acute cholecystitis. The combination of upper-right quadrant pain and fever is retrospectively defined as acute cholecystitis. Ultrasonographic evaluation included gallbladder wall thickness (> 4 mm is considered to be pathologic), pericholecystic fluid, and acute cholecystitis, which is considered to be the combination of both. Laboratory analysis included leukocyte count, aspartate transaminase (AST), alanine transaminase (ALT), alkaline phosphatase (ALP, normal value is < 390 IU/L), gamma-glutamyl transpeptidase (GGT), and total and direct serum bilirubin. Intraoperative findings included anatomic variations, indication for conversion, and time of surgery (daytime or nighttime). Surgeries were performed either by residents or by senior surgeons. The standard four-port technique was applied in all cases. None of the surgeries involved intraoperative cholangiography or choledocal exploration.
Statistics
Among the 1231 laparoscopic cholecystectomies that were completed successfully, we chose 104 as the control group through the Statistical Package for Social Sciences (SPSS) “select case” option. We compared the 104 converted patients with the control group.
We used SPSS version 17 (IBM SPSS Statistics) for data analysis, Pearson chi-square and Fisher's exact test for categorical variables, and the t-test for continuous variables. Multivariate logistic regression analysis was performed to determine the combination of variables that would distinguish each group. Intervals were calculated through logistic regression odds ratios and their correspondent 95% confidence interval (95% CI). The receiver operating characteristic (ROC) curve was used with ALP and age to determine a cutoff value after which risk was significantly increased.
The logistic model calculates a probability for each subject. A cutoff value of 0.5 was used to calculate the sensitivity and specificity of the model. If the probability for a specific subject was higher than 0.5, conversion to open cholecystectomy was predicted for the subject. Finally, the predicted probabilities and the actual groups were cross-classified to calculate sensitivity and specificity.
Results
One thousand three hundred thirty five cases were evaluated in the study. One thousand two hundred thirty one cases (85.2% of the 1444 cases) were laparoscopically completed successfully. One hundred four cases (7.7%) were converted to open surgery. The most common cause of conversion was the inability to distinguish anatomic landmarks due to inflammation and fibrosis around the Calot's triangle, which was present in 72.3% of the converted cases. Univariate comparison of analyzed variables is shown in Table 1. The following factors were found to be statistically insignificant: variables of body mass index, fever, upper-right quadrant tenderness, history of pancreatitis, ultrasonographic findings of gallbladder wall thickness over 4 mm and pericholecystic fluid, leukocyte count, AST, ALT, GGT, total and direct serum bilirubin, anatomic variations, time of surgery, and the seniority of the surgeon leading the surgery. The number of attacks was close to the border of significance.
ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate transaminase; BMI, body mass index; GGT, gamma-glutamyl transpeptidase; RUQ, Right Upper Quadrant.
Male gender, age, ALP, history of abdominal surgery, history of choledocolithiasis, and ultrasonographic findings of acute cholecystitis were found to be statistically significant. Being male increased the risk of conversion by 2.912 times (95% CI: 1.410–6.018). Similarly, age greater than 55 years increased the risk by 4.660 times (95% CI: 2.3–9.441), ALP greater than 80 IU/L increased the risk by 2.355 times (95% CI: 1.158–4.789), and a history of abdominal surgery increased the risk by 2.548 times (1.189–5.46).
We drew an ROC curve and determined that 55 years of age and an ALP value of 80 IU/L were the best cutoff values. A multivariate logistic regression analysis showed that age greater than 55 years, male gender, ALP greater than 80 IU/L, and history of abdominal surgery were independent risk factors. Choledocholithiasis and ultrasonographic findings of acute cholecystitis were also risk factors, but because they were observed in a low number of cases, they could not be included in our multivariate analysis. Even though ultrasonographic findings of acute cholecystitis were a risk factor, clinical findings of acute cholecystitis were not.
Table 2 shows the results of logistic regression. We used these risk factors to develop a model that predicts open cholecystectomy with 70% sensitivity and 79% specificity. The area under the ROC curve for the overall model is 0.77. The 95% CI is between 0.71 and 0.84 and a P value lower than .001.
ALP, alkaline phosphatase; B, beta coefficient; Exp (B), exponentiation of beta coefficient.
Figure 1 shows the formula for this statistical model. All four values are required to be present for a positive diagnostic test. For example, for a 68-year-old male patient with normal ALP values and no prior abdominal surgery, the risk of conversion would be 53.8%.
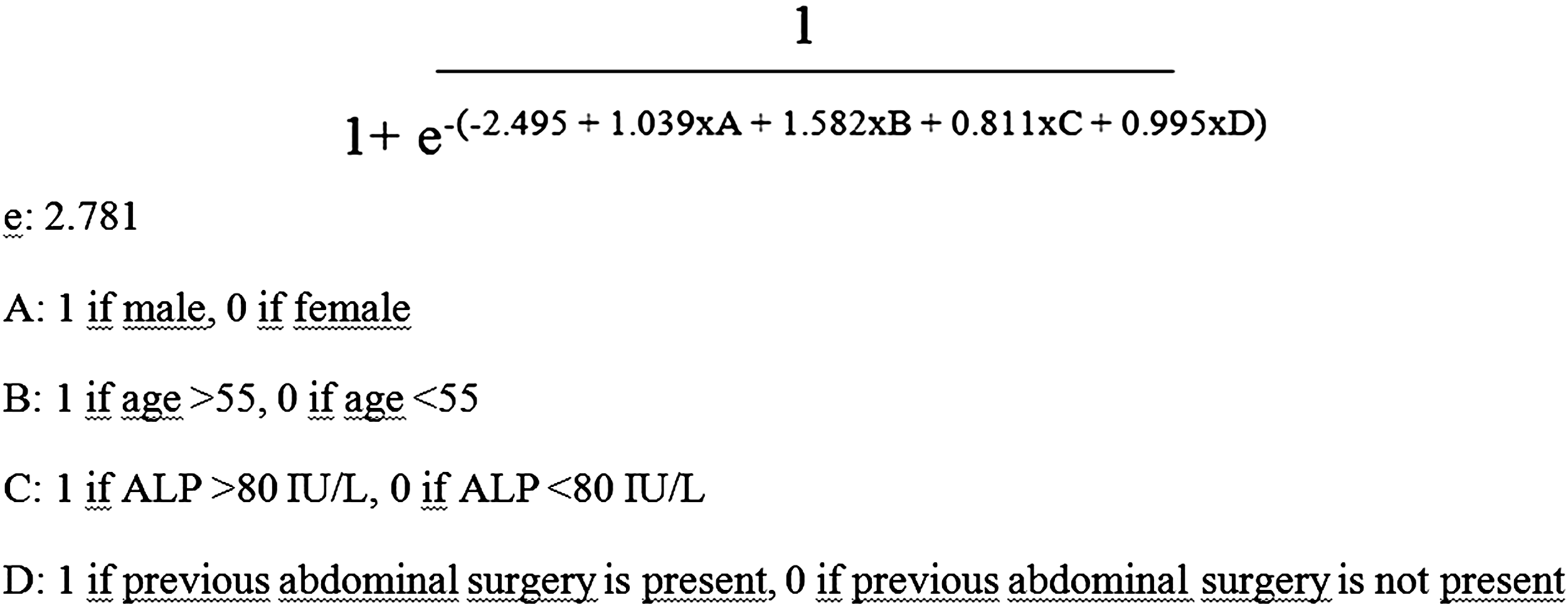
Formula for statistical model.
Discussion
The preoperative identification of predictive factors for conversion of laparoscopic cholecystectomy to open surgery is a longstanding question. The rate of conversion is 7.7% for our clinic, whereas reported rates in literature range between 3% and 24%. The most common reason for conversion seems to be inflammation and fibrosis around the Calot's triangle, which is consistent with literature.3,6,7 Most authors regarded male sex as a risk factor for conversion, and our experience was similar.2,3,8–11 Genc et al. found that only male sex is a risk factor. 8 Hutchinson et al. 9 did not find age to be a risk factor, whereas we found it a significant risk and noticed that the risk significantly increased after 55 years of age. Other authors report age as a risk factor; however, they give cutoff values ranging from 50 to 65 years.2,4,6,10,11 Another study showed a cutoff value of 50 years. 6 Age is probably important because an individual is likely to experience higher number of cholecystitis attacks while aging. Our data show that an ALP value that is higher than 80 IU/L, although this is regarded as within normal range, is a relevant risk factor. There is no other report in literature regarding ALP values as a risk factor. ALP is known to increase as a result of cholestasis and cholecystitis. These patients probably have a history of previous cholecystitis attacks which may cause an increase in ALP. We also found that a history of abdominal surgery is another risk factor, as previously reported by other authors.2,6 We did not find obesity as a risk factor, although it was reported as such by some authors.4,9,12,13 In this study, acute cholecystitis and choledocolithiasis preoperatively treated by endoscopic sphincterectomy were also found to be risk factors. Choledocholithiasis develops at the setting of longstanding gallstones and subsequent inflammation around gallbladder may interfere with laparoscopic intervention. However, because of the low number of these cases, we did not include them in the multivariate analysis. Even though ultrasonographic findings of acute cholecystitis were a risk factor, clinical findings of acute cholecystitis were not. This result indicates that ultrasonographic findings are more valuable when determining conversion rates. In contradiction to our findings, Sakpal et al. found that surgeon experience was a risk factor. 6
There were numerous attempts in the past to identify predictive factors for conversion to open cholecystectomy. Similar to our study, Kama et al. found male gender, age (> 60 years), abdominal tenderness, history of abdominal surgery, gallbladder wall thickness, and acute cholecystitis as risk factors, and developed a scoring system with 78% sensitivity and 72% specificity. 11 In this scoring system, the presence of acute cholecystitis and ultrasonographic gallbladder wall thickness had the highest coefficient, whereas age had the lowest. 11 Gupta et al. 14 found that history of hospitalization, palpable gallbladder, impacted stone, and gall bladder wall thickness were predictive risk factors. Their scoring system has a sensitivity of 95.74% and a specificity of 73.68%.
In conclusion, we managed to create a statistical model for predicting conversion from laparoscopic to open cholecystectomy. Our model included age, gender, ALP value, and history of abdominal surgery. There is still room for potential in this model with multicentered analysis. An accurate prediction of high-risk patients will allow surgeons to schedule the time of surgery and assemble a team accordingly. This prediction will also enable surgeons to inform high-risk patients before surgery.
Footnotes
Acknowledgments
This article was selected as a poster presentation for the 10th European-African Hepato Pancreato Biliary Association Congress, Belgrade, 2013. Authors would like to thank Mrs. Handan Selamoglu for extensive language editing.
Disclosure Statement
No competing financial interests exist.