
Abstract
Abstract
Purpose:
The usage of barbed sutures is increasingly being reported in the field of laparoscopic surgery. However, there have been reports of suture-related complications such as small bowel obstruction or anastomosis stricture. We present our experience of hepaticojejunostomy (HJ) using V-loc, during laparoscopic cyst excision for choledochal cyst.
Methods:
At our center, from August 2014 to January 2015, 4 patients were treated for choledochal cyst. Laparoscopic cyst excision with Roux-en-Y HJ was performed, and HJ was performed with intracorporeal suturing using unidirectional barbed sutures. After surgery, the patients were followed up in the outpatient clinic every 3 months to monitor for long-term complications such as biliary stricture.
Results:
There were no short-term complications. Among the 4 patients, 3 patients did not experience any long-term complications. As of this writing, the follow-up period for the 4 patients is 16 months for the first 2 patients and 11 months for the later 2 patients. Biliary stricture was diagnosed in 1 patient at 7 month follow-up. HJ revision was performed with an open right subcostal incision. The anastomosis showed dense fibrosis and stricture. The patient recovered uneventfully after the surgery.
Conclusions:
HJ using barbed sutures was relatively easy to perform, but barbed sutures may have a tendency to cause stricture when used in biliary enteric anastomosis. Caution must be taken to prevent overtightening of the suture.
Introduction
B
For this reason, barbed sutures are being used in many fields of laparoscopic surgery. Many studies have reported on the safety and feasibility of barbed sutures, compared with conventional sutures.1,2 In contrast, there have been recent reports of suture-related complications, such as small bowel obstruction 3 or anastomosis stricture. 4 Despite the fact that barbed sutures are not a newly introduced technology, it seems that the safety of these sutures has not been fully established.
Choledochal cysts are a rare disease, characterized by biliary tree dilation. The incidence of choledochal cyst is relatively low in the Western population, estimated to be ∼1 in every 100,000–150,000. The incidence is much higher in Asia, at about 1 in every 1000. 5 The treatment of choice is complete excision of the cyst with appropriate surgical reconstruction. As in many other fields in surgery, laparoscopic surgery has been reported to be feasible in the treatment of choledochal cyst.6,7 But because of the narrow caliber of the bile duct, meticulous intracorporeal suturing and knotting are necessary. And because of this, many centers still perform open surgery for the treatment of choledochal cyst. Barbed sutures can be useful in this setting.
We present our initial experience of laparoscopic cyst excision with hepaticojejunostomy (HJ) using V-loc (Covidien, Mansfield, MA) unidirectional barbed sutures for the treatment of choledochal cysts.
Materials and Methods
Study design
This was a retrospective case series, performed by analyzing medical records. This study was approved by the Institutional Review Board of our center. At our center, from August 2014 to January 2015, 4 consecutive patients were treated for choledochal cyst. Laparoscopic cyst excision with Roux-en-Y HJ was performed, and HJ was performed using intracorporeal sutures of V-loc unidirectional barbed sutures. After surgery, the patients were followed up in the outpatient clinic every 3 months to monitor for long-term complications such as biliary stricture.
Outcome measurement
Patient demographics and perioperative outcome were analyzed. The collected demographic data were age, sex, body mass index (BMI), comorbidities, and pathologic findings. The collected perioperative data were operation time, estimated blood loss, return to diet, length of hospital stay, short-term complications, and long-term complications. Short-term and long-term complications were defined as events that required treatment within and after 30 days after surgery, respectively.
Surgical technique
The patient was placed in a supine position. After general anesthesia, a 10 mm trocar was placed through the umbilicus and a videoscope was inserted. Under direct vision, a 12 mm trocar was placed in the left subcostal area, about 10 cm below the xiphoid process, about 5 cm to the left of the midline. Two 5 mm trocars were placed in the right subcostal area, similar to the right subcostal trocars placed in four-port cholecystectomy, but in a more caudal position. When five trocars are used, an additional trocar is placed in the left subcostal area, lateral to the 12 mm trocar.
The gallbladder was retracted with an instrument inserted through the right lateral trocar. The peritoneum over the first part of the duodenum was incised, and the peritoneum overlying the choledochal cyst anterior wall was dissected. The lateral wall of the cyst was mobilized from the hepatic artery, and the posterior wall of the cyst was mobilized from the portal vein. The proximal end of the cyst was dissected and divided. The cystic duct was dissected and divided, but the gallbladder was not dissected from the liver bed because of retraction purposes. The distal end of the cyst was dissected down to the intrapancreatic portion. The distal stump was ligated with two hem-o-lok clips and divided.
The jejunum 50 cm distal from the Treitz ligament was divided intracorporeally with a linear stapler (endo-GIA®; Ethicon Endosurgery, Inc., Cincinnati, OH) inserted through the 12 mm trocar. The distal jejunal limb was brought up to the liver and HJ was performed with 3-0 absorbable unidirectional sutures (V-Loc 180®; Covidien). A continuous running suture was performed on both the posterior and anterior wall of the anastomosis (Fig. 1). After anastomosis was completed, the remnant suture was cut with ∼1 cm remaining. At a location about 45 cm distal from the HJ, hand-sewn jejunojejunostomy was performed by delivering the jejunum through the left subcostal 12 mm incision, which was extended to about 2 cm. The specimen was removed and a drain was placed in the Morrison's pouch.
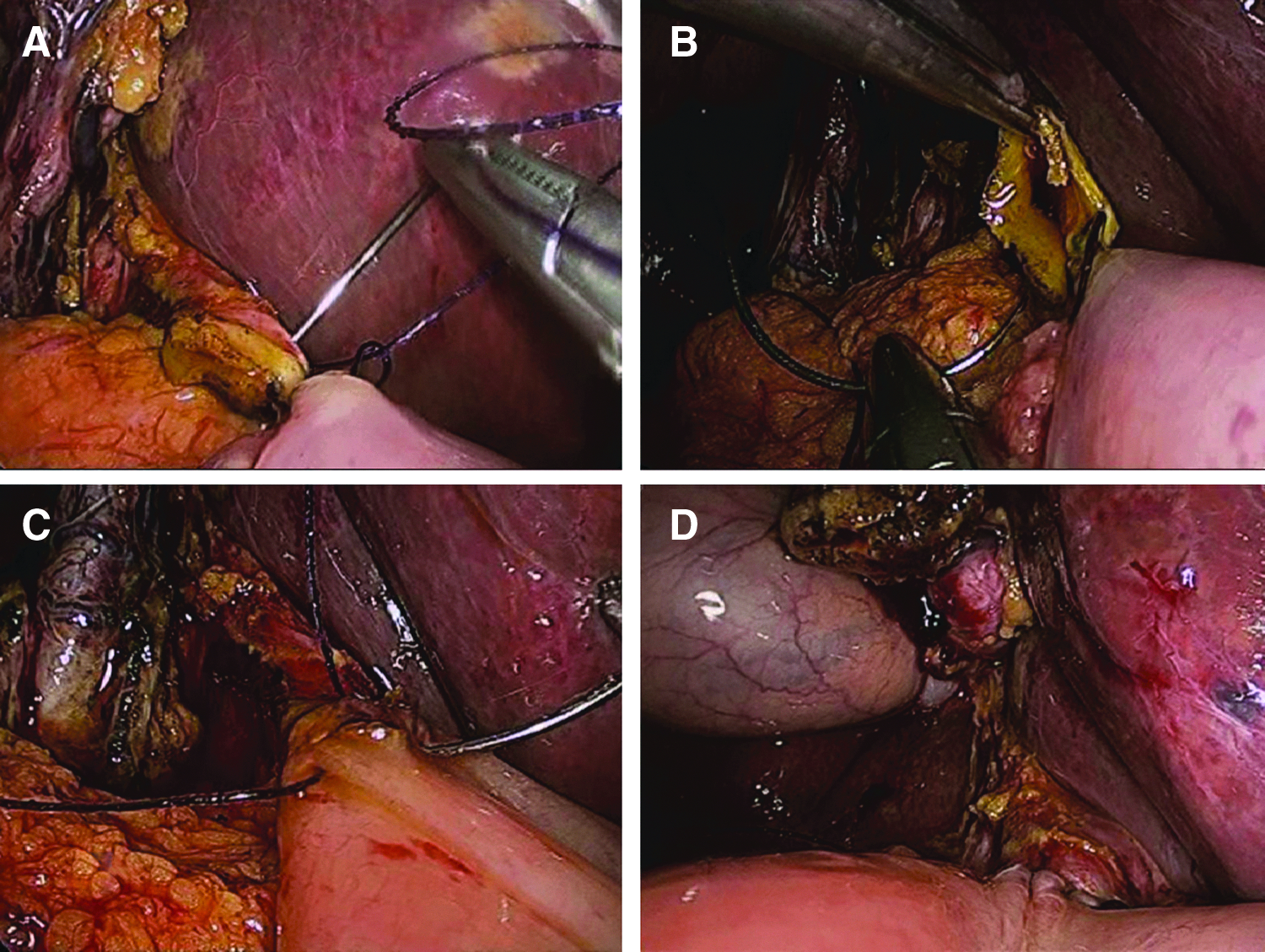
Operative view of hepaticojejunostomy using unidirectional barbed sutures after laparoscopic cyst excision.
Results
During the study period, 4 patients received treatment for choledochal cyst. Table 1 shows the demographic data and perioperative data of the 4 patients. Three patients were female and 1 patient was male. The average age was 41.2 ± 11.9 (range 22–54) and the average BMI was 22.9 ± 4.9 kg/m2 (range 18.7–31.1 kg/m2). In all 4 patients, the initial presenting symptom was abdominal pain and the Todani classification was type 1. The average size of the cyst was 3.5 ± 0.8 cm (2.5–4.5 cm).
The mean operation time was 160.0 ± 15.4 minutes (range 145–185 minutes), and the average estimated blood loss was 182.5 ± 97.1 mL (30–300 mL). In the first 2 patients, five trocars were used, and in the third and fourth patients, four trocars were used.
There were no short-term complications. Among the 4 patients, 3 patients did not experience any long-term complications. As of this writing, the follow-up period for the patients are 16 months for the first 2 patients and 11 months for the third and fourth patients. One patient, at 6-month follow-up, showed jaundice with a total bilirubin level of 3.6 mg/dL and an alkaline phosphatase level of 567 U/L. Magnetic resonance cholangiopancreatography (MRCP) was performed and biliary stricture was diagnosed. HJ revision was performed under general anesthesia and the anastomosis showed dense fibrosis and stricture. The patient recovered uneventfully after the surgery.
Discussion
Choledochal cyst (CDC) is a disease that manifests as a congenital dilation of the intrahepatic and/or extrahepatic bile ducts. It affects more females than males, and is often detected in the first decade of life. It is categorized into five subtypes, according to a classification established in 1959 by Alonso-Lej et al. 8 Type I, which is the dilation of the common bile duct, is the most common type, comprising ∼50%–80% of all cases. All the cases in this study were also type I. Treatment of CDC is complete excision of the cyst, followed by appropriate surgical reconstruction. With the advent of laparoscopic surgery, laparoscopic treatment has been established as a feasible option.
The most difficult part of laparoscopic suturing is maintaining suture tension during suturing and making the knot. Since their introduction in 2009, barbed sutures have made laparoscopic suturing easier by eliminating the need of maintaining tension or knot making. Many products have been developed, such as V-loc (Covidien) unidirectional sutures or Stratafix (Ethicon Endosurgery, Inc.) bidirectional sutures. These sutures are applied over a wide range of specialties. The use of barbed sutures has been reported in urologic surgery, orthopedic surgery, and plastic surgery.9–11 But its most active use has been in the field of advanced laparoscopic general surgery. Many types of anastomoses have been performed laparoscopically using barbed sutures. There have been reports of gastrojejunostomy and pancreaticojejunostomy.12,13
In this study, the usage of barbed sutures in HJ was analyzed. HJ is the key component of laparoscopic treatment of choledochal cyst. Unlike other types of anastomoses, this cannot be performed using a linear stapler. This is because the caliber of the bile duct is small and because the location of the anastomosis is adjacent to the liver hilum, with very little space to maneuver in. When considering these characteristics of HJ, it seems that HJ can benefit from the use of barbed sutures. With the difficult process of maintaining suture tension and knot making eliminated, laparoscopic HJ can be performed much easily. In fact, the average operation time of our study was about 160 minutes, which was shorter than the operation times reported previously, which was about 210∼250 minutes.7,14
But among the 4 patients included in our study, 1 patient developed anastomosis stricture. At routine follow-up, this patient showed an elevated total bilirubin level of 3.6 mg/dL and MRCP showed stricture at the HJ. HJ revision was performed and the operative findings showed dense fibrosis at the anastomosis site, resulting in anastomotic stricture. Several factors may have influenced the development of anastomosis stricture. When HJ is performed, there is the inherent risk of stricture, compared with other anastomoses with larger caliber such as enteroenteric anastomosis. This is especially true in the treatment of CDC. After complete excision of the dilated bile duct cyst, the remaining bile duct to be anastomosed is often of normal caliber. Furthermore, when compared with pediatric CDC patients, adult CDC patients have suffered the disease for a longer duration of time. This results in more inflammation and fibrosis, which can result in a higher overall complication rate. 7 Indeed, a 2011 study by Cho et al. that analyzed adult CDC patients reported a stricture rate of 6.3%, which is higher than stricture rates reported in the pediatric population. 15
Another factor that obviously needs to be considered is surgical expertise. Of course the level of surgical expertise is difficult to objectify, but we are a high-volume hepatobiliary center, performing about 120 cases of major liver resection, 50 cases of major pancreatic surgery, and 15 cases of liver transplantation annually. Also, we have previously reported the use of barbed sutures in laparoscopic choledocholithotomy, 16 and are not inexperienced in the usage of these sutures. These things considered, it is possible that overtightening of the suture may have caused the stricture. In contrast to conventional sutures, in which the suture can be tightened or loosened after completion of suturing, barbed sutures have limited capacity of be loosened after suturing. When using barbed sutures, overtightening should be avoided, especially in anastomoses of small caliber such as HJ.
The characteristics of the barbed suture may have caused the stricture. Specifically, the barbs built into the sutures have shown to cause adverse side effects such as small bowel obstruction or anastomosis stricture. Donnellan and Mansuria reported a case of small bowel obstruction caused by the remaining end of bidirectional sutures. 17 These sutures were used for closure of the vaginal cuff after laparoscopic total hysterectomy. The authors describe in their article that after experiencing this case, they modified their technique of suturing by using surgical clips at the end of each remaining suture, and cutting the suture flush with the clip. A similar case was reported by Thubert et al. 18 Laparoscopic sacral colpopexy was performed, and peritoneal closure was performed with barbed sutures to prevent bowel entrapment. The lateral wall of ileum was snared by the remaining suture, resulting in small bowel volvulus and obstruction.
In these two case reports, the surgeons had left a length of remnant barbed suture after anastomosis, which caused the small bowel obstruction. But in the case reported by Kohler et al., peritoneal closure was performed using barbed sutures after transabdominal preperitoneal hernioplasty. 3 During the initial procedure, the operator sutured the peritoneum with the barbed suture, and after completion of closure cut the suture flush with the peritoneum to ensure that there was no remnant suture. However, the suture cut through the peritoneum and caused a small bowel obstruction, which required reoperation. It seems that small bowel obstruction can be used even after “adequate” usage of the suture.
In their 2013 article, Liatsikos et al. reported their results of using barbed sutures in laparoscopic pyeloplasty. 4 In 6 patients, a knotless continuous anastomosis was performed between the ureter and the renal pelvis using barbed sutures. Five patients (83%) developed anastomosis stricture. The authors allow that surgical technique and the inherent characteristics of ureteropelvic junction anastomosis may have influenced the results.
Before the introduction of barbed sutures, knots were made laparoscopically after intracorporeal suturing. After completion of suturing, the sutures were cut with several centimeters of suture left to avoid loosening of the knot. But in the case of barbed sutures, because of its structural characteristics, too much remnant sutures may result in complications. The instruction manual made by one of the manufacturers explains that after completion of suturing, two or three sutures should be made backward and the remnant suture “cut flush with the tissue,” this may prevent any suture-related complications. But the literature shows that complications may arise even when the suture is cut short.
An issue to be considered is cost of the sutures. Barbed sutures are more expensive than conventional monofilament sutures used in HJ. According to the expense reports of our hospital, using the current exchange rate of this article writing in February 2016 that is 0.81 US dollars (USD) per 1000 Korean Won, the cost of V-loc is 20.4 USD and the cost of PDS II sutures (PDS®II polydioxanone; Ethicon, Somerville, NJ) is 6.1 USD. Although using barbed sutures can be easier, the increased cost can be a burden to the patient and the medical system. It seems that the advantages of reduced operative time and the disadvantages of suture-related complications and expensive cost need to be weighed carefully.
As of this article writing, this is the first report of HJ using barbed sutures. As the reduction in operation time in our study shows, HJ using barbed suture was relatively easy to perform. But it seems that with regard to the usage of barbed sutures, additional safety measures need to be applied. At our center, we plan to continue using barbed sutures in the laparoscopic treatment of choledochal cyst, being careful to prevent overtightening of the suture. If we encounter a second case of anastomosis stricture, it is our plan to reconsider our choice of laparoscopic sutures.
Conclusions
HJ using V-loc unidirectional sutures was relatively easy to perform, but barbed sutures may have a tendency to cause stricture when used in biliary enteric anastomosis. Caution must be taken to prevent overtightening of the suture. Further studies are required to confirm these findings.
Footnotes
Disclosure Statement
No competing financial interests exist.