
Abstract
Abstract
Objectives:
The aim of this study was to investigate the clinical usefulness for prediction of outcome of laparoscopic partial nephrectomy (LPN) using the R.E.N.A.L nephrometry scoring system (RNS) and centrality index score (C-index).
Materials and Methods:
We retrospectively reviewed 64 patients who underwent LPN from 2010 to 2014 in our institution. The RNS and C-index scores were assigned according to the described protocols for their systems. The relationships between the patients' scores before surgery and the outcomes of LPN, warm ischemia time (WIT), operative time (ORT), estimated blood loss (EBL), and percent change in estimated glomerular filtration rate (eGFR) were analyzed retrospectively.
Results:
Mean tumor size was 3.1 cm, mean WIT was 27.6 minutes, mean ORT was 189.0 minutes, and mean EBL was 187 mL. Although the RNS had statistically significant correlations with WIT, ORT, and percent change in eGFR, these correlations were not score-dependent. For WIT, a statistically significant difference was observed between the low-risk group and the middle-risk group. For percent change in eGFR, a statistically significant difference was observed between the low-risk group and the high-risk group only. For the C-index, statistically significant correlations between complexity categories and WIT, ORT, EBL, and percent change in eGFR were observed. Regarding the raw C-index scores, linear correlations were observed between the scores and each outcome of LPN.
Conclusions:
The RNS and C-index are useful for predicting the complexity of LPN. The C-index may be more suitable than the RNS for predicting postoperative renal function.
Introduction
I
From the technical standpoint, PN is more difficult to perform than RN, especially when it is performed under laparoscopy. Laparoscopic partial nephrectomy (LPN) has higher complication rates.10–12 Preoperative evaluation of the complexity of a planned LPN is important for selecting the appropriate surgical procedures. Several evaluation methods have been presented for standardization of the anatomical features of renal tumors.13–15 The R.E.N.A.L nephrometry scoring (RNS) system was proposed in 2009 as a standardized system for quantitating renal tumors. 13 The RNS is based on five features that characterize the anatomy of a solid renal tumor on preoperative cross-sectional imaging. The centrality index score (C-index) is described as a set of clinically useful measures of tumor centrality. 14 The C-index is obtained by dividing the distance from the tumor center to the kidney center by the tumor radius. It remains unclear whether the RNS or the C-index can reflect surgical outcome more correctly. To clarify this question, this study evaluated the association of both systems' scores with tumor complexity and postoperative outcome.
Materials and Methods
We reviewed the records of 64 consecutive patients who underwent LPN for a solid renal tumor performed by two surgeons between April 2010 and August 2014 at our institution. All patients underwent preoperative imaging with contrast-enhanced computed tomography or magnetic resonance imaging. Demographic and operative data were obtained from the medical records. RNS and C-index scores were determined according to the described protocols for those systems.13,14
For RNS, the patients were divided into the low-risk group (nephrometry sum 4–6), middle-risk group (sum 7–9), and high-risk group (sum 10–12). For the C-index system, the patients were divided into two categories of 2.5 points or more as the low-complexity group and <2.5 points as the high-complexity group.
Preoperative characteristics were assessed, including sex, tumor size and location, age, body mass index, and estimated glomerular filtration rate (eGFR). Intraoperative characteristics were assessed, including warm ischemia time (WIT), operative time (ORT), and estimated blood loss (EBL). For the postoperative renal function indicator, percent change in eGFR at 3 months after the surgery was used. We investigated the relationship between intraoperative and postoperative characteristics and the systems categories of the RNS and the C-index. In this patient series, the RNS and C-index were not used to determine the surgical procedure.
Statistical analysis was performed using JMP version 9 (SAS, Cary, NC). Values of P < .05 were considered statistically significant.
Results
Sixty-four patients were included in this study. The patients' characteristics are shown in Table 1. The distribution of the RNS and C-index values is shown in Table 2. Of the 64 study patients, 49 (77%) were male and 15 (23%) were female. For RNS criteria, 19 (30%) patients were categorized in the low-risk group, 35 (55%) patients were categorized in the middle-risk group, and 10 (15%) patients were categorized in the high-risk group. For C-index criteria, 37 (58%) patients were categorized in the low-complexity group, and 27 (42%) patients were categorized in the high-complexity group. The mean tumor size was 3.1 cm. Sixty-one (95%) laparoscopic partial nephrectomies were performed with renal artery clamping; all of these procedures involved warm ischemia.
C-index, centrality index score.
C-index, centrality index score; RNS, R.E.N.A.L. nephrometry scoring system.
The mean WIT was 27.6 minutes, and the mean ORT was 189.0 minutes. The mean EBL was 187 mL.
The operative and postoperative characteristics in each system are shown in Table 3.
C-index, centrality index score; eGFR, estimated glomerular filtration rate.
In analyzing the RNS categories, the middle-risk patients had significantly longer WIT than the low-risk patients. The mean WIT values were 21.2 minutes for the low-risk group, 30.8 minutes for the middle-risk group, and 27.6 minutes for the high-risk group (P = .0175 for low versus middle).
As for the C-index criteria, the WIT was significantly longer in the high-complexity group than in the low-complexity group (31.9 minutes versus 21.7 minutes, P = .0039).
Regarding ORT, the middle-risk group had significantly longer ORT than the low-risk group in the RNS (157 minutes for low-risk group, 202 minutes for middle-risk group, and 206 minutes for high-risk group; P = .0162; low versus middle and P = .0536; low versus high). In the C-index, the ORT in the high-complexity group was significantly longer than in the low-complexity group (214 minutes versus 155 minutes; P = .0002).
With the RNS, we could not find any significant associations between the risk groups and EBL (97 mL for low-risk group, 241 mL for middle-risk group, and 170 mL for high-risk group). In the C-index, EBL was significantly higher in the high-complexity group than in the low-complexity group (257 mL for high-complexity group and 91.3 mL for low-complexity group; P = .0347).
For renal function change after LPN, RNS risk criteria were significantly associated with percent change in eGFR (−8.40% for low-risk group, −13.2% for middle-risk group, and −18.4% for high-risk group; P = .0227; low-risk group versus high-risk group). In the C-index, percent change in eGFR was significantly higher in the high-complexity patients than in the low-complexity patients (−17.0% mL for high-complexity group and −6.5% for low-complexity group; P = .0001). Moreover, a linear correlation was observed between raw C-index values and intra- and postoperative factors, such as WIT, ORT, EBL, and percent change rate in eGFR after LPN (R2 = 0.164, P = .0012 for WIT; R2 = 0.326, P < .0001 for ORT; R2 = 0.066, P = .0397 for EBL; R2 = 0.210, P = .0002 for percent change in eGFR). Among them, strong correlation was observed between the C-index score and ORT, especially percent change in eGFR (Fig. 1).
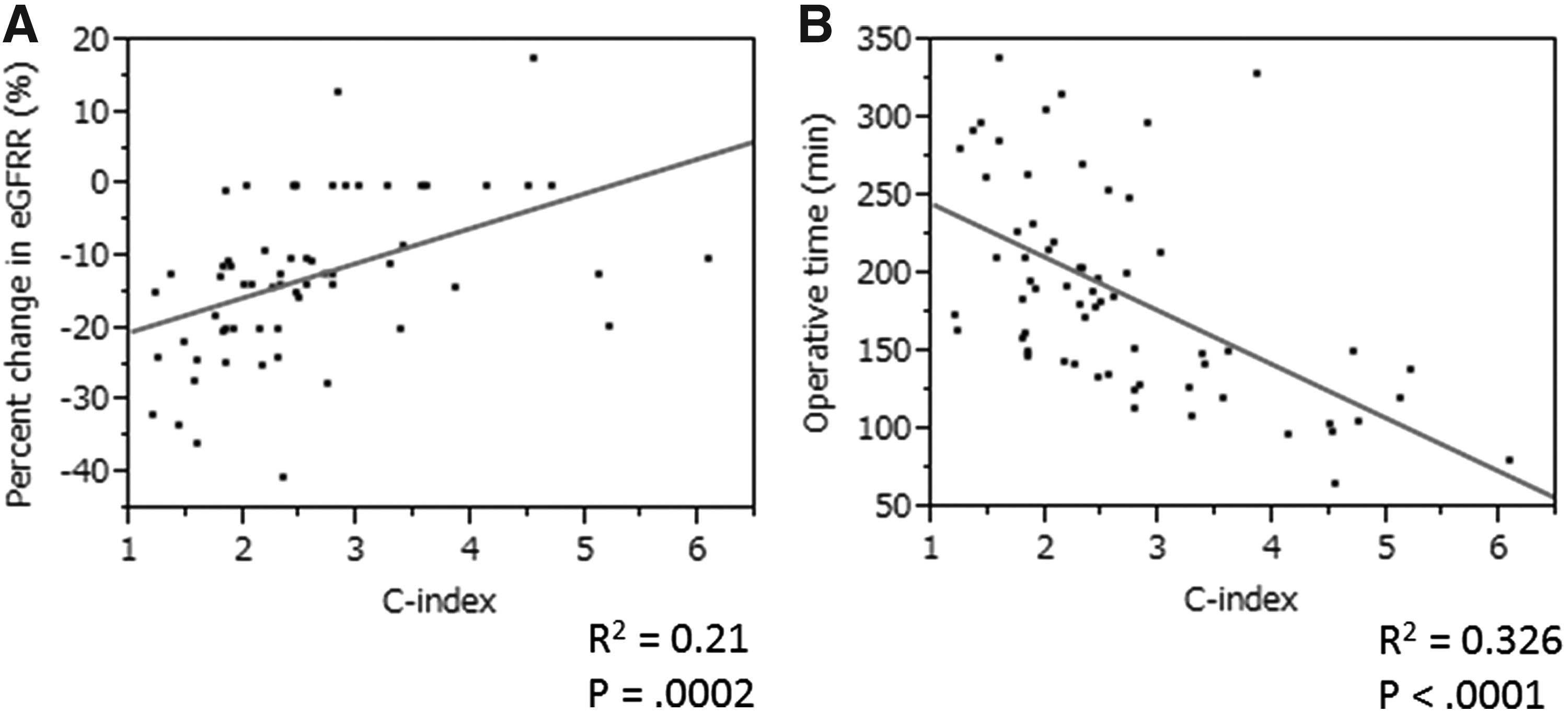
Correlations between raw C-index values and outcomes
Discussion
The mainstay for the treatment of localized renal mass is excision. Retrospective studies have clarified that oncologic outcome of PN is equivalent to RN for patients with early stage kidney cancer.4–7 In recent years, the indications for PN have been expanding. Laparoscopic and/or robot-assisted PN is widely performed in many medical centers. Multiple scoring systems have been proposed to standardize the description of the anatomical features of renal tumors.
Several studies have reported attempts to verify the usefulness of each scoring system for estimating PN outcomes. The RNS and the C-index appear to be the most well discussed of the scoring systems.
Regarding the RNS, its usefulness for estimating the complexity of LPN has been well addressed. Although previous articles have consistently stated that RNS was useful for estimating intraoperative outcomes, such as EBL, WIT, and hospital length of stay, study results have been inconclusive on whether the RNS can estimate renal functional outcome correctly after surgery.16,17 On the other hand, one study reported an association between the C-index and renal functional outcomes after LPN. 18 Interestingly, these investigators did not find any association between the C-index and intraoperative outcomes, such as EBL or ORT. 18 However, since the number of studies examining the relationship between the C-index and LPN has been limited, it is difficult to reach any definitive conclusions.
To date, only a few articles have been published evaluating several preoperative scoring systems for predicting LPN outcome using the same patient population. In these articles, the similarity of the RNS to the C-index is relatively well described; however, the differences between the scoring systems were not fully discussed.19,20 This study is the first to directly compare the usefulness of the RNS and the C-index using the same patient population and to clearly discuss the differences between the RNS and the C-index.
Our analysis showed that the RNS and C-index are useful systems for predicting the complexity of LPN. For predicting renal function outcome after LPN, the C-index may be more useful than the RNS considering the strong statistical correlations.
The RNS is a superior system for predicting surgical complexity. Several previous studies have reported that the RNS score was associated with the intraoperative parameters of ischemia time, EBL, and total ORT.16,17 Although this study also demonstrated that the RNS categories of low-risk, middle-risk, and high-risk were partially correlated with WIT, ORT, and percent change in eGFR, we could not find a consistent relationship between RNS criteria and intra- and postoperative outcomes. For example, WIT was significantly different between only the low-risk and middle-risk groups; on the other hand, percent change in eGFR was significantly different between only the low-risk and high-risk groups. The RNS score is obtained by the sum of the numbers that represent five tumor factors. So, the same RNS score does not mean same tumor condition; the tumor condition can vary between the same score. As for the high-risk criteria, patients with sums of 11 or 12 were not included in this study; only patients with the sum of 10 were included. Patients with sums of 11 or 12 have very complicated tumors and are not suitable candidates for LPN. This may explain why the RNS could not predict the outcome of LPN consistently. On the other hand, the descriptions by the RNS are superior for making decisions regarding the surgical procedure; the score is useful for selecting the appropriate procedure for each patient depending on the tumor description.
The C-index directly describes tumor complexity; it is obtained by dividing the distance from the tumor center to the kidney center by the tumor radius. It is very important that raw C-index scores are well correlated with WIT, ORT, EBL, and percent change rate in eGFR after LPN. In future, by accumulating a large number of cases, a nomogram can be created for correctly predicting postsurgical results (i.e., eGFR change) by using the C-index score before surgery. By predicting surgical outcome more accurately, more precise decisions can be made concerning the appropriate procedure for each patient (e.g., LPN or open PN or laparoscopic RN, etc.).
Although the RNS and C-index are useful systems for patient evaluation before LPN, there are differences between them. The RNS is applicable for describing tumor complexity, and the C-index is helpful for predicting the outcome of LPN. The characteristics of each system need to be recognized so that each can be used appropriately, depending on the purpose.
This study had some limitations. It was a single-institution retrospective study with a small number of study patients, and the follow-up period was short. A large, prospective, multi-institutional study is required to demonstrate the ideal validated use of the C-index for predicting LPN outcome.
Conclusions
The RNS and C-index score systems can provide useful descriptions of surgical complexity. The C-index has the potential for precisely predicting postoperative renal function. At the present time, for daily clinical application, the characteristics of each scoring system should be recognized so that appropriate use can be made of them.
Footnotes
Disclosure Statement
No competing financial interests exist.