
Abstract
Abstract
Background:
In the recent years, laparoscopic splenectomy and esophagogastric devascularization (LSD) for liver cirrhosis and portal hypertension rapidly gained the interest of hepatobiliary surgeons due to its minimal invasion. This study aimed to gather and analyze available data from the observational studies that have compared LSD and open splenectomy and esophagogastric devascularization (OSD) for liver cirrhosis and portal hypertension.
Materials and Methods:
All the studies comparing LSD and OSD for liver cirrhosis and portal hypertension were searched on the available databases, including the Cochrane Central Register of Controlled Trials, Medline, Science Citation Index, EMBASE, China National Knowledge Infrastructure, Wanfang Database, and China Biomedical Database. Data were analyzed using Review Manager software version 5.0.
Results:
After the literature search, a total of 17 studies were included in the meta-analysis, which involved 1093 patients: 552 in the laparoscopic group and 541 in the open group. The laparoscopic group was shown to have a lower overall postoperative complication rate (0.43; 95% confidence interval [CI; 0.29–0.64]) than the open group (P < .0001), which was not associated with heterogeneity between the studies. The laparoscopic group was shown to have a lower intraoperative blood loss (−320.62; 95% CI [−552.35 to −88.9]), shorter time of oral intake (−29.08 hours; 95% CI [−35.28 to −22.88]), and shorter hospital stay (95% CI [−6.19 to −2.19]) than those of the open group (P < .00001). The operative time of the laparoscopic group was 42.16 minutes longer (95% CI [32.20–52.11]) compared with the open group (P < .00001). There was no significant difference of hospitalization costs between the studies.
Conclusion:
This meta-analysis demonstrated that laparoscopic left lateral resection is a safe and feasible option associated with a reduced overall complication rate. The current evidence suggested that it could be performed routinely in liver centers.
Introduction
L
Recently, owing to the cumulative experiences of laparoscopic surgeries and recent advances in operating devices, especially vessel sealing systems, laparoscopic approaches have been increasingly indicated in various fields, including for patients with liver cirrhosis and portal hypertension, where significant advances in laparoscopy equipment and training have enabled laparoscopic splenectomy and esophagogastric devascularization (LSD) to be carried out in a lesser invasive way.5,6
Observational studies have shown the increased efficiency and safety of LSD. Some studies have directly compared LSD and open splenectomy and esophagogastric devascularization (OSD). However, no multicenter randomized controlled trial (RCT) or meta-analysis has compared these two types of operations. This study aimed to gather and analyze available data from the observational studies that have compared LSD and OSD for patients with liver cirrhosis and portal hypertension, aiming at clarifying controversy about their utilization in such conditions.
Materials and Methods
Literature search
The reviewer searched the following online electronic databases—the Cochrane Central Register of Controlled Trials, Medline, Science Citation Index, EMBASE, China National Knowledge Infrastructure, Wanfang Database, and China Biomedical Database—using the search terms: laparoscopic splenectomy, portal hypertension, azygoportal disconnection, devascularization, and esophagogastric devascularization. Searches were updated until July 2014. After identifying relevant titles, the abstracts of these studies were screened to identify whether the study was eligible. The full article was retrieved when the information in the title and/or abstract appeared to meet the objective of this review. A manual search of reference lists of studies thus obtained was conducted for any relevant articles not found in the computerized search.
Study selection
Clinical studies eligible for inclusion were, which described LSD, performed in the setting of liver cirrhosis and portal hypertension. Given the paucity of the available evidence addressing the study question, all study designs were accepted in the overall review, including RCTs, controlled clinical trials, comparative studies, and case series. Studies were required to use LSD in at least five patients per treatment group and report efficacy and/or safety outcomes. Studies containing duplicate material were excluded and the larger of the studies, containing the best-documented data, was included for the analysis. Studies involving pediatric patients and animals were excluded.
Data extraction
Two reviewers (authors H.Y. and H.Z.) independently extracted all relevant information in a data collection form, including study characteristics (author, country, sample size, and methodological characteristics) and operative outcomes (operative time, intraoperative blood loss, the time of oral intake, hospitalization costs, postoperative hospital stay, and complications).
Statistical analysis
The statistical software Review Manager, version 5.0 (The Cochrane Collaboration, Software Update, Oxford, United Kingdom) was used to perform the analysis. The weighted mean difference was used to analyze differences among continuous variables, taking into account the effect of sample size. The odds ratio, which examines the odds of an adverse effect occurring in each group and compares it, was used to analyze differences in dichotomous variables. The 95% confidence interval (CI) was reported for each analyzed value.
To standardize the data on continuous variables, it was important to include the standard deviation for each variable reported directly by each study. For the studies that provided the range values for each variable, these values were converted to standard deviations and analyzed. Continuous variables without standard deviations were not included in the analysis. Studies that had no events with a particular outcome for laparoscopic and open groups were not included. To assess publication bias, graphic exploration with funnel plots was used.
Results
Characteristics of included studies
The search identified a total of 233 potential articles. After initial screening and deduplication, 30 articles were selected from their titles and abstracts and a full examination of their texts was made. Ultimately, there were 17 articles that were deemed to meet the inclusion criteria (Fig. 1). All were observational studies with methodological limitations (Table 1) as follows: seven nonrandomized comparative studies and nine case series. The included studies can be divided into two subgroups according to surgical procedures: LSD group and OSD group.
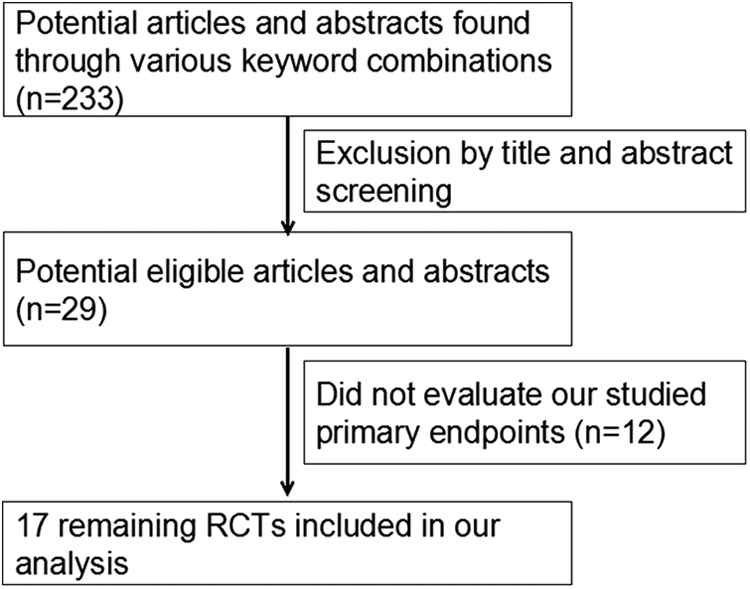
Analysis of the search results. RCT, randomized controlled trial.
LSD, laparoscopic splenectomy and esophagogastric devascularization; OSD, open splenectomy and esophagogastric devascularization.
Meta-analysis of operative time
Seventeen RCTs (Wang Z, 2009; Jiang S, 2010; Wu L, 2011; Huang XW, 2007, unpublished data)7–19 have evaluated the operative time. Heterogeneity analysis of the operative time was significant difference (P = .0001; I2 = 65%), and a random effect model was used. The results showed that the operative time in the LSD group was longer than OSD group (Mean Difference [MD] = 42.16, 95% CI [32.20–52.11]; P < .00001) (Fig. 2).
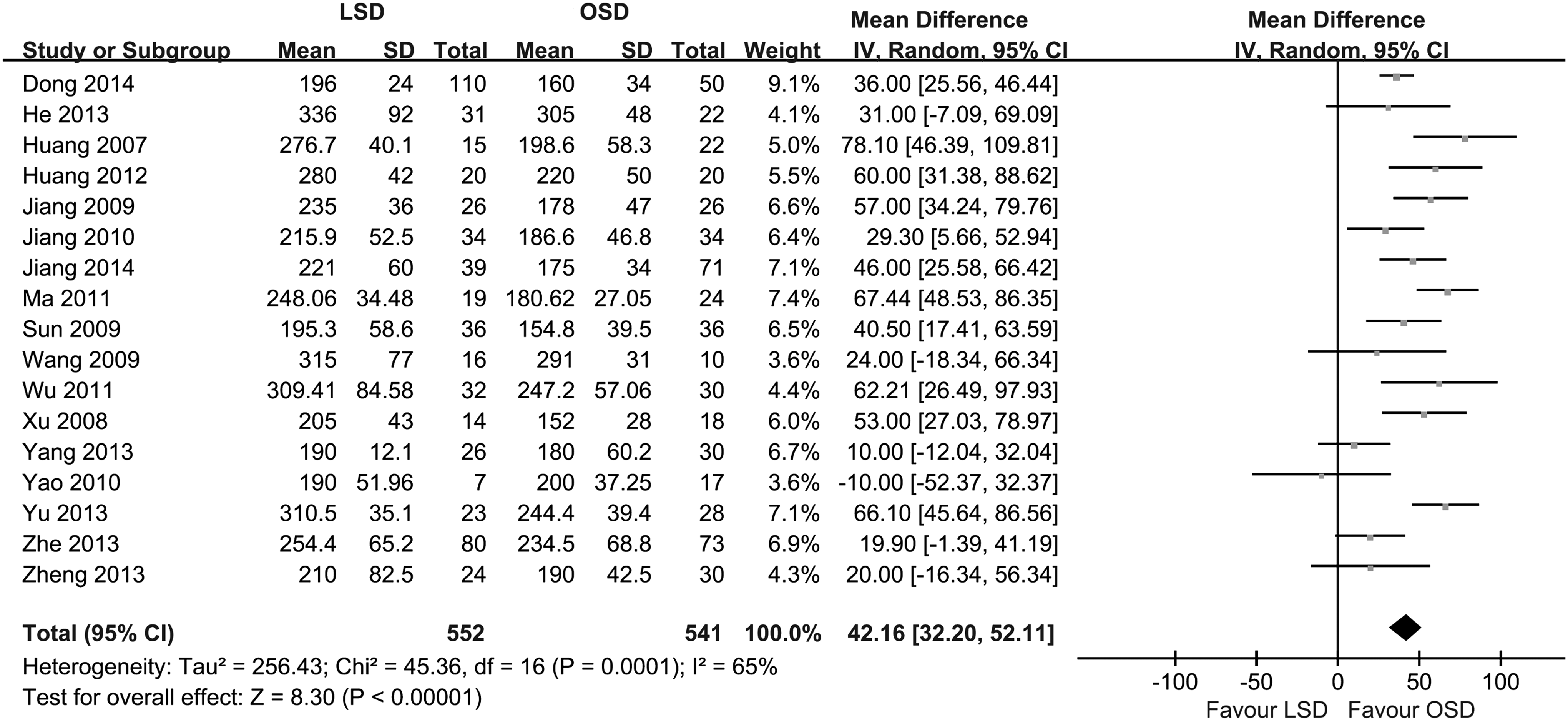
Meta-analysis of assessing the operative time. Test for heterogeneity: chi-squared test with its df and P value; inconsistency among results: I2 test for overall effect; Z statistic with P value. CI, confidence interval; df, degrees of freedom; LSD, laparoscopic splenectomy and esophagogastric devascularization; OSD, open splenectomy and esophagogastric devascularization.
Meta-analysis of estimated intraoperative blood loss
Seventeen RCTs7–19 (Wang Z; Jiang S; Wu L; Huang XW, unpublished data) have evaluated the estimated intraoperative blood loss. Heterogeneity analysis of the operative time was significant difference (P < .00001; I2 = 100%), and a random effect model was used. The results showed that the estimated intraoperative blood in the LSD group was less than OSD group (MD = −330.62, 95% CI [−552.35 to −88.90]; P = .007) (Fig. 3).
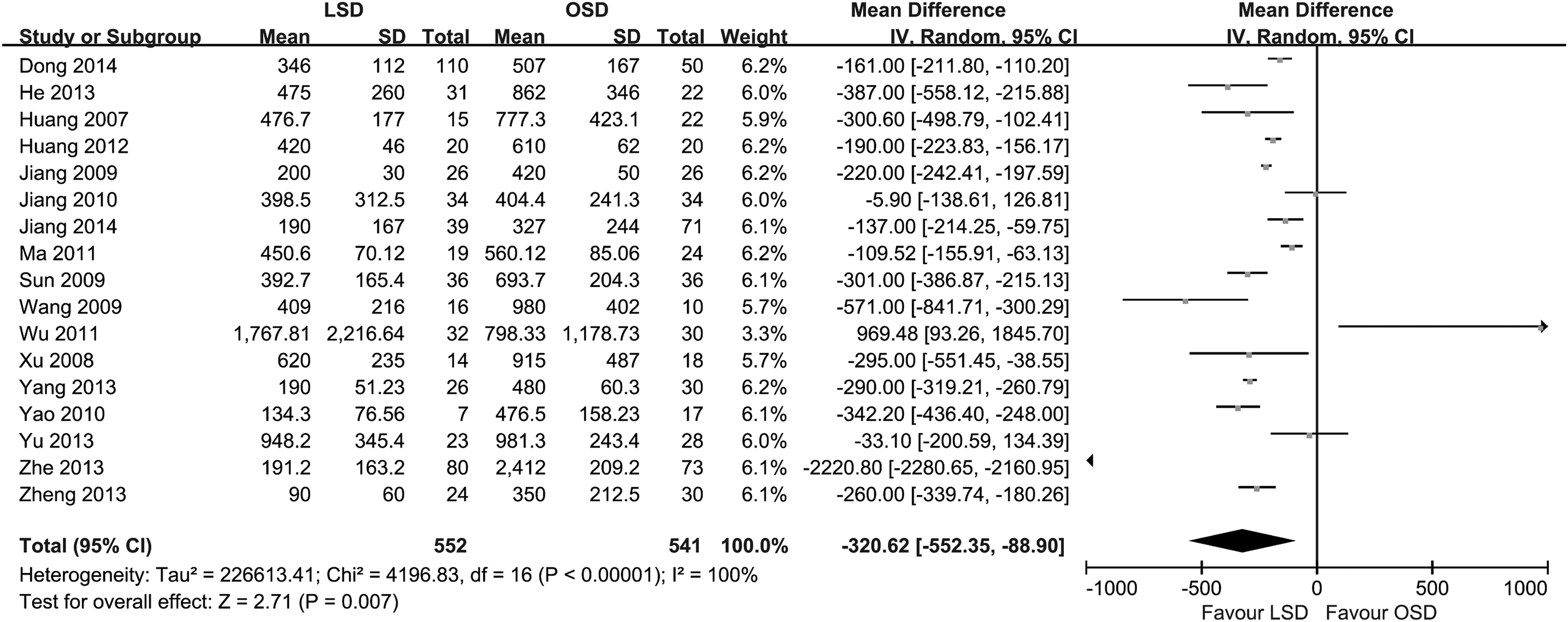
Meta-analysis of assessing the estimated intraoperative blood loss. Test for heterogeneity: chi-squared test with its df and P value; inconsistency among results: I2 test for overall effect; Z statistic with P value. CI, confidence interval; df, degrees of freedom; LSD, laparoscopic splenectomy and esophagogastric devascularization; OSD, open splenectomy and esophagogastric devascularization.
Meta-analysis of time of oral intake
Twelve RCTs (Wang Z; Jiang S, unpublished data)7–11,13–16,18 have evaluated the time of oral intake. Heterogeneity analysis of the operative time was significant difference (P < .00001; I2 = 78%), and a random effect model was used. The results showed that the estimated intraoperative blood in the LSD group was shorter than OSD group (MD = −29.08, 95% CI [−35.28 to −22.88]; P = .007) (Fig. 4).
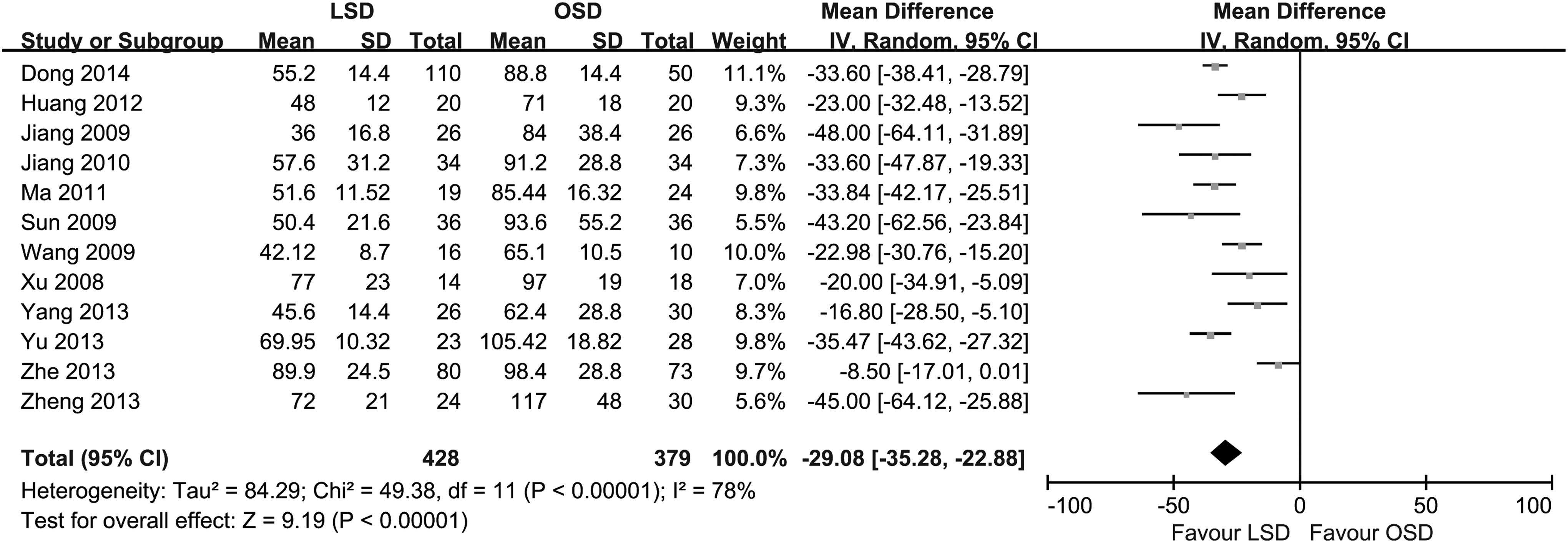
Meta-analysis of assessing the time of oral intake. Test for heterogeneity: chi-squared test with its df and P value; inconsistency among results: I2 test for overall effect; Z statistic with P value. CI, confidence interval; df, degrees of freedom; LSD, laparoscopic splenectomy and esophagogastric devascularization; OSD, open splenectomy and esophagogastric devascularization.
The time of postoperative hospital stay and hospitalization costs
Fifteen RCTs (Wang Z; Jiang S; Wu L; Huang XW, unpublished data)7,10–19 have evaluated the time of postoperative hospital stay. Heterogeneity analysis of the operative time was significant difference (P < .00001; I2 = 98%), and a random effect model was used. The results showed that the time of postoperative hospital stay in the LSD group was shorter than OSD group (MD = −4.19, 95% CI [−6.19 to −2.19]; P < .0001) (Fig. 5). Six RCTs (Wang Z; Wu L; Huang XW, unpublished data)11,12,14 have evaluated the hospitalization costs. The results showed that the time of hospitalization costs in the LSD group has no significant difference from the OSD group (MD = 834.89, 95% CI [−467.21–2136.99]; P = .21).
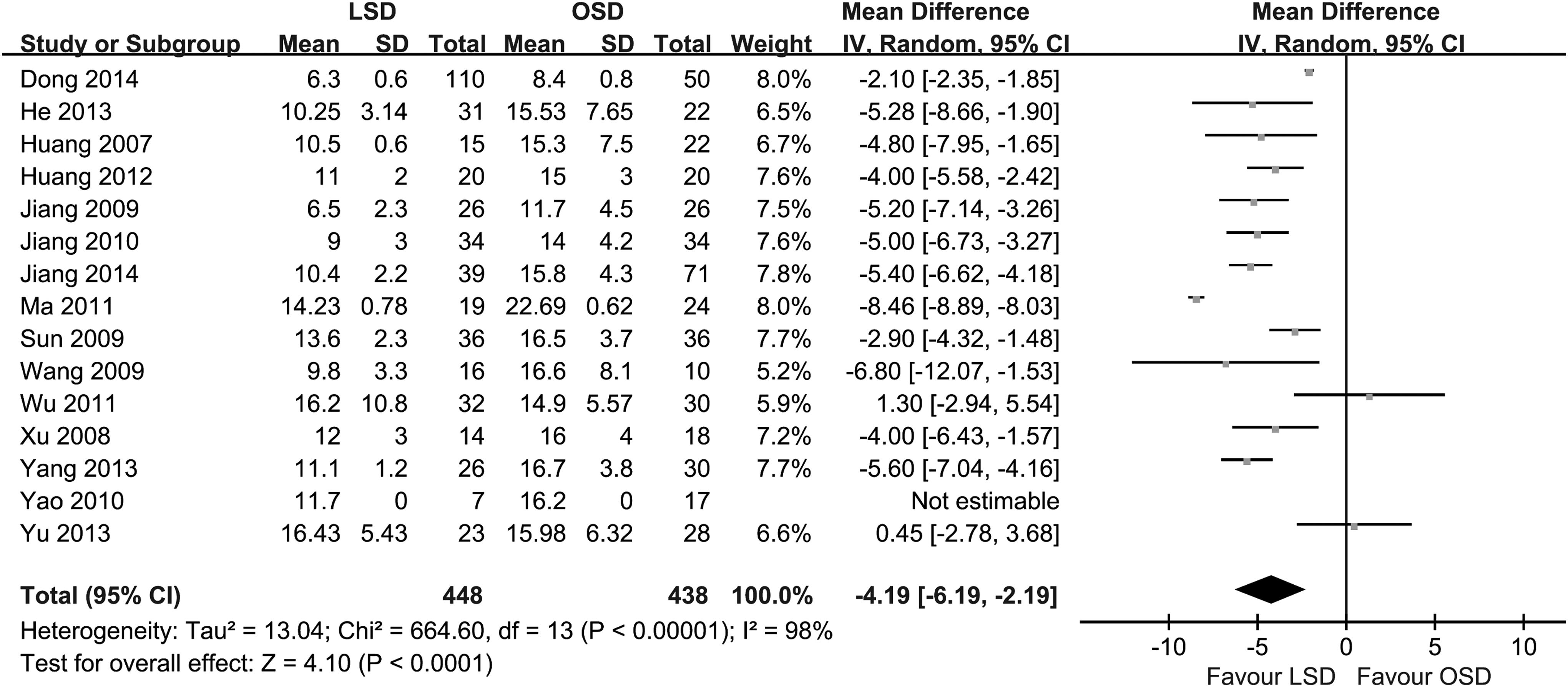
Meta-analysis of assessing the time of postoperative hospital stay. Test for heterogeneity: chi-squared test with its df and P value; inconsistency among results: I2 test for overall effect; Z statistic with P value. CI, confidence interval; df, degrees of freedom; LSD, laparoscopic splenectomy and esophagogastric devascularization; OSD, open splenectomy and esophagogastric devascularization.
Meta-analysis of the time of postoperative complications
Eleven RCTs (Wang Z; Jiang S; Wu L; Huang XW, unpublished data)7,8,10,11,16–18 have evaluated the postoperative complications. Heterogeneity analysis of postoperative complications was not different (P = .53; I2 = 0%), and a fixed effect model was used. The results showed that the postoperative complications in the LSD group were lower than the OSD group (Odds Ratio = 0.43, 95% CI [0.29–0.64]; P < .0001) (Fig. 6).

Meta-analysis of assessing the postoperative complications. Test for heterogeneity: chi-squared test with its df and P value; inconsistency among results: I2 test for overall effect; Z statistic with P value. CI, confidence interval; df, degrees of freedom; LSD, laparoscopic splenectomy and esophagogastric devascularization; M-H, Mantel-Haenszel; OSD, open splenectomy and esophagogastric devascularization.
Publication bias
Funnel plots were drawn to observe the publication bias for the above analysis; the results showed less publication bias for the analysis of operation time, time of oral intake, time of postoperative hospital stay, and hospitalization costs. However, the analysis for intraoperative blood loss suggested the presence of publication bias.
Discussion
Portal hypertension is a common condition secondary to liver cirrhosis and is highly prevalent in China, which is hemodynamically defined as a pathological increase in the portal pressure gradient. 20 The common problems associated with liver cirrhosis patients, such as liver failure and hepatic encephalopathy, with portal hypertension often have the life-threatening complications of hypersplenism and esophagogastric variceal bleeding (EGVB). EGVB is a life-threatening situation with mortality rates of at least 20%. 21 Surgery is one of the most important ways, in which portal hypertension can be treated, and at present, there are many alternatives, including endoscopic sclerotherapy and banding, transjugular intrahepatic portosystemic shunt, splenorenal shunt, and ED.22–25 As an effective treatment for EGVB and hypersplenism due to portal hypertension (PH), OSD has been widely accepted clinically for many years.26,27 However, it is excessively invasive in terms of blood loss and wound pain, which may aggravate liver function impairment and ascites and be associated with high rates of morbidity and mortality, especially in those with advanced cirrhosis. In recent years, advances in endoscopic technology provided a new treatment for such patients. And the preliminary research in recent years shows that LSD in the treatment of liver cirrhosis with portal hypertension has the obvious advantage of being minimally invasive. 28
It was showed in the results of this study that estimated intraoperative blood loss and postoperative complications of LSD were lower than the OSD group, which expressed that patients would have the benefit of a minimally invasive procedure. Estimated intraoperative blood loss in the laparoscopic group was less, may be the abdominal mirror has amplification effect on local anatomic structure, which makes the operation field clearer and avoids unnecessary vascular injury. Application of laparoscopic operation instruments, such as ultrasonic knife and LigaSure, can reduce the hemorrhage. 29 Postoperative complication rate of LSD was less than the OSD, which probably due to laparoscopic operation has fine operation, small incision, light operation stress response, and little effects on the immune system of patients with minimal invasive advantage. And compared with OSD, operation time of LSD was longer, which was depended on the proficiency of endoscope, qualification of operation, and so on. With the development of laparoscopic technique, operation time will be shortened gradually. Compared with the OSD group, the LSD group has small incision, less pain, early ambulation, and eating, so patients recovered quickly. Although the laparoscopic operation will inevitably require the use of laparoscopic operation instruments, such as disposable biological vascular clamp and titanium clip, which increases operation costs, the postoperative hospital stay of LSD was shorter than the OSD group, which made the LSD group hospitalization costs similar to the OSD group.
There were many limitations to this study. Literature retrieval may not be comprehensive. As the literature language has restrictions and limited resources, we searched the main web database, but still have undetected literature, gray literature, and other issues; the research data are not included in the evaluation system and may affect the results. Because of the medical ethical reasons, it is very difficult to carry out RCT of clinical development. Clinical controlled trials included in this article have low literature quality and were easy to cause the bias. All articles were from one nation in this study, which make limitations of sample source research in the literature and publication bias.
In conclusion, the publications reviewed revealed LSD and OSD to be safe and effective in the setting of liver cirrhosis and portal hypertension. From the comparison articles, LSD appears to be superior to OSD regarding blood loss, hospital stay, complication rate, and time of oral intake. However, it is difficult to draw firm statistical conclusions due to lack of high-quality evidence. There is an urgent need for RCTs of laparoscopic surgery in cirrhotic patients.
Footnotes
Disclosure Statement
No competing financial interests exist.