
Abstract
Abstract
Background:
Esophagectomy and esophageal reconstruction with organs other than the gastric tube are complicated and difficult surgical procedures. We developed a new method of thoracoscopic esophagectomy with intrathoracic esophagojejunostomy in the upper mediastinum when the gastric tube cannot be used as an esophageal substitute for reconstruction.
Materials and Methods:
Total gastrectomy, preparation of pedicled jejunal conduit, and transhiatal lower mediastinal dissection were done under laparotomy. Upper and middle mediastinal dissection was performed thoracoscopically. After esophageal transection with a linear stapler above the arch of the azygos vein, an anvil was inserted transorally. A circular stapler–inserted jejunal conduit was introduced to the upper mediastinum via the transhiatal route with relaparotomy. Esophagojejunostomy was completed by double stapling technique.
Results:
We completed this procedure for 10 consecutive cases without conversion to thoracotomy. The median operation time, amount of blood loss, duration of intrathoracic anastomosis, and number of dissected total and thoracic nodes was 741 (665–1019) minutes, 835 (380–2090) ml, 94.5 (70–211) minutes, and 59 (16–165) and 30 (10–54) nodes, respectively. There was no anastomotic leakage, conduit necrosis, or hospital mortality. Two cases showed delayed anastomotic stenosis. The median body weight loss 3 months after surgery was 13.9%. The overall 5-year survival rate was 90% (stage I, 100% and stage III, 83.3%).
Conclusions:
Thoracoscopic esophagectomy with intrathoracic esophagojejunostomy is safe and curative. This operation can be performed as a minimally invasive surgical procedure for esophageal cancer patients in whom the stomach cannot be used as a reconstruction conduit.
Introduction
I
The optimal esophageal substitute after esophagectomy remains controversial. A recent study showed that the jejunum was superior to the colon for reconstruction after esophagectomy, along with gastrectomy, with respect to short-term results (less anastomotic leakage and shorter hospital stay) and long-term results (less body weight loss). 4
The jejunum is uniquely suited for esophageal reconstruction because it is relatively abundant, does not require formal preparation, is typically free of disease, has a lumen size similar to that of the esophagus, and has intrinsic peristalsis. 5 Although a disadvantage of this subcutaneous reconstruction method is that it is the longest route, jejunal reconstruction after esophagectomy has generally been performed by lifting the conduit via the subcutaneous route because of easier management of postoperative complications (e.g., anastomotic leakage and intestinal necrosis) compared with posterior mediastinal reconstruction and the convenience of microvascular anastomosis with the internal thoracic vessels.3,4,6–8
We have reported the usefulness of intrathoracic esophagojejunostomy in the upper mediastinum by pedicled jejunum after esophagectomy and total gastrectomy. 9 This method can be applicable to upper esophageal cancer, unless the cervical esophagus is involved. It also enables us to shorten the complicated and laborious process of microvascular anastomosis. The reconstruction is performed under thoracotomy and laparotomy. Recently, we changed the thoracic procedure to a method that consisted of thoracoscopic mediastinal dissection and thoracoscopic esophagojejunostomy. In this article, we introduced our ingenuity of newly developed method and the results of thoracoscopic esophagojejunostomy with mediastinal dissection.
Materials and Methods
Patients
We performed a retrospective review of consecutive esophageal cancer patients in whom the gastric tube could not be used who underwent surgery from 2009 onward. All patients underwent thoracoscopic radical esophagectomy and total gastrectomy by laparotomy with reconstruction by thoracoscopic esophagojejunostomy in the upper mediastinum using the pedicled jejunum. The Kanazawa University Hospital database was searched after Institutional Review Board approval. The demographic characteristics, operative details, and postoperative outcomes were collected and analyzed. Tumors were staged according to the TNM classification of the American Joint Committee on Cancer and the Union Internationale Contre le Cancer 7th edition. Thoracoscopic esophagectomy is approved by Japanese governmental health insurance. Thoracoscopic intrathoracic esophagojejunostomy was approved by the Review Committee in Department of Gastroenterological Surgery, Kanazawa University. All the patients gave informed consent before treatment.
Surgical technique
All patients underwent entire mediastinal lymph node dissection and esophageal resection under thoracoscopic surgery. Upper abdominal lymph node dissection, including the perigastric and celiac nodes, was performed under laparotomy. The whole stomach was removed from each of the four patients who underwent synchronous gastrectomy. The remnant stomach was removed in all six patients who underwent prior gastrectomy. Cervical node dissection (i.e., three-field lymph node dissection) was performed in three patients with apparent upper mediastinal node metastasis.
The operation was started with the abdominal procedure and continued with thoracic dissection and intrathoracic anastomosis (Fig. 1). In the supine position after laparotomy, the availability of jejunal construction was confirmed by observation of regional vascular anatomy using transillumination as described by Blackmon et al. 5 In most cases, the fourth branch of the superior mesenteric artery functioned as the distal vascular pedicle to the mobilized jejunal conduit, with transection of the second and third branches. After demonstration of adequate collateral circulation by Doppler ultrasonography with test clamping, the mesenteric vessels proximal to the pedicle were ligated and divided close to their origin. The intact vessel network between each branch was preserved, if at all possible. The jejunum was divided ∼20 cm distal from the Treitz ligament.
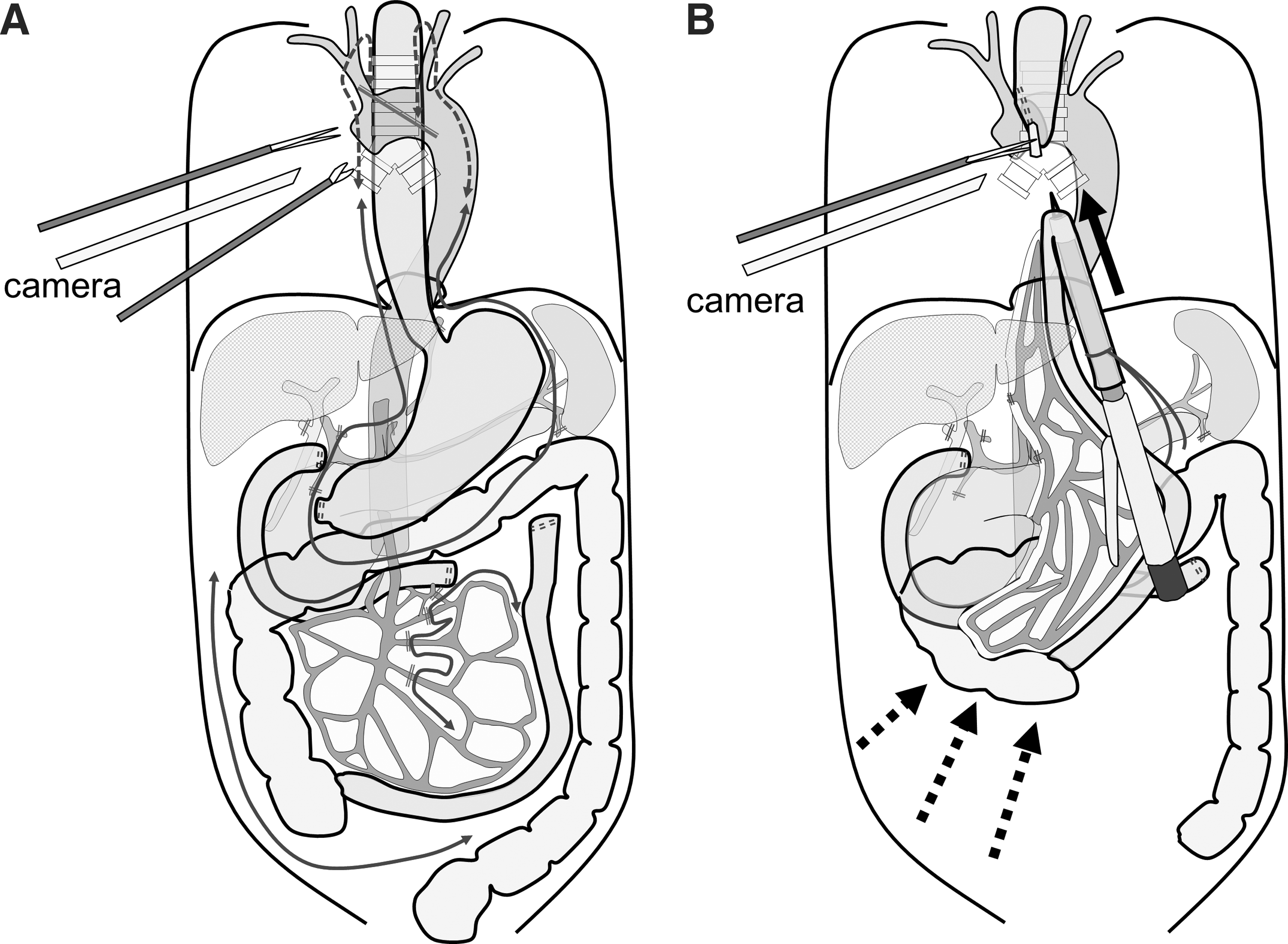
Schematic illustrations of thoracoscopic esophagectomy and total gastrectomy
As a refinement to elongate the jejunal conduit, the ileum and right colon were mobilized from the retroperitoneum to free the fixation of the mesentery at the right lower retroperitoneum. In this technique, the highest point of the jejunal conduit shifts cranially without further ligation of vascular loops between the sacrificed jejunal branches. Total gastrectomy with abdominal lymph node dissection and transhiatal lower mediastinal dissection was performed through laparotomy.
After temporary abdominal closure, the patient was situated in the left lateral oblique position. Thoracoscopic esophagectomy with upper and middle mediastinal dissection was performed in the left lateral position by bed rotation as described previously. 10 The position of the surgeons and video monitors and sites of the thoracoports and the laparotomy are shown in Figure 2. The esophagus was divided by a 60-mm linear stapler at the upper mediastinum above the arch of the azygos vein to ensure the oral surgical margin from the tumor. A 25-mm anvil (OrVil; Covidien, Mansfield, MA) was inserted transorally. 11 The oral gastric tube was advanced through the edge of the esophagostomy of the esophageal stump and removed through one of the thoracoscopic ports. The anvil was then ready for connection to the 25-mm circular stapler.
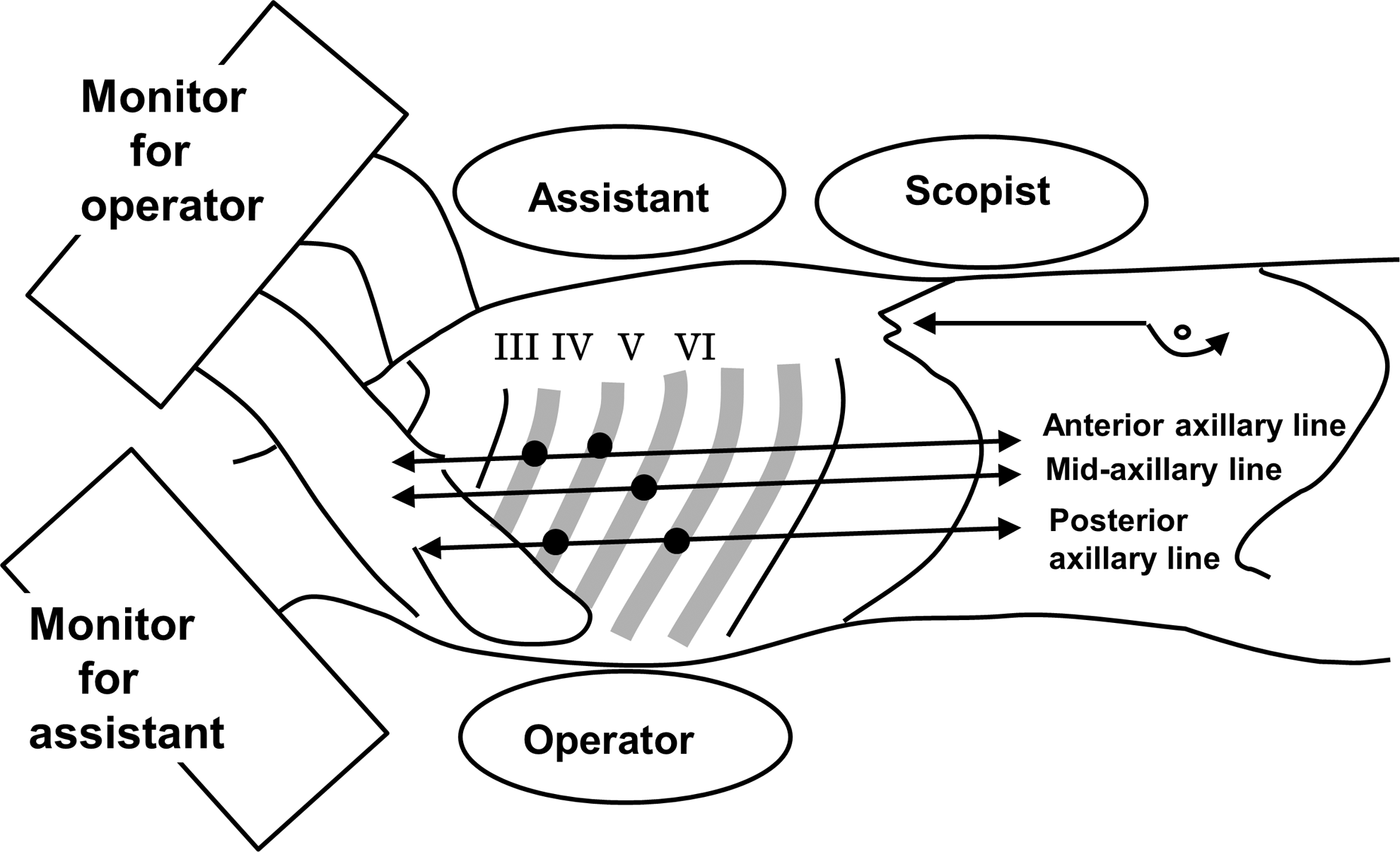
Position of the surgeons and video monitors and sites of the thoracoports and laparotomy. Five 12-mm thoracoports (black dots) were inserted during the thoracoscopic procedure.
The reconstruction procedure was performed in the left lateral oblique position under relaparotomy. After confirmation of the circulation of the pedicled conduit, a jejunal conduit was introduced to the upper abdomen via the retrocolic route. To make the long jejunal stump, marginal vessels proximal to the anastomotic point were transected. A circular stapler (EEA XL, 25 mm; Covidien) was introduced into the jejunal conduit from the oral end of the conduit and fixed by ligation (Fig. 3A). The circular stapler–inserted pedicled jejunal conduit was introduced into the right thoracic cavity from the enlarged esophageal hiatus via the retrocolic route and placed in the upper mediastinum (Fig. 1B).
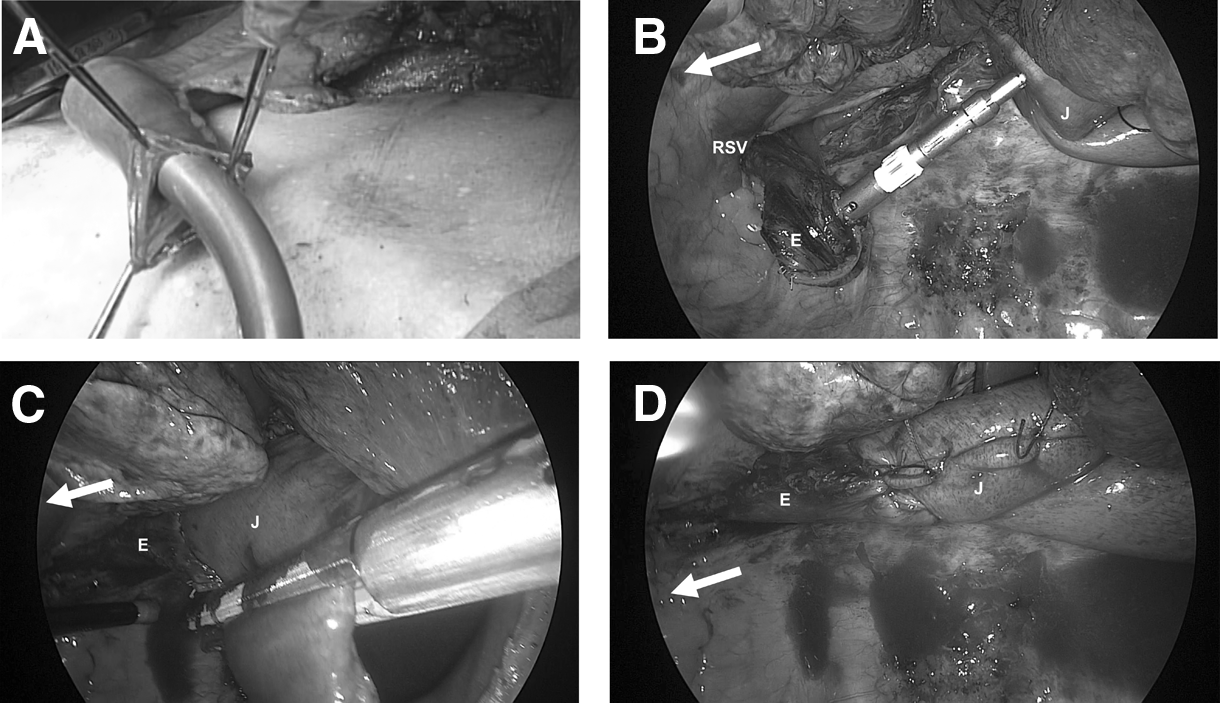
Procedure of thoracoscopic intrathoracic esophagojejunostomy.
The spike from the circular stapler was advanced through the jejunal conduit and connected to the anvil (Fig. 3B). After completion of end-to-side intrathoracic esophagojejunostomy by firing the staple, the stapler was removed from the stump by cutting the ligation of the jejunal stump and circular stapler. The jejunal stump was closed with a linear stapler (Fig. 3C). An additional seromuscular suture to cover the exposed staple at the jejunal and esophageal stump was added (Fig. 3D). Reconstruction with the pedicled jejunal conduit by the Roux-en-Y method was completed with abdominal side-to-end jejunojejunostomy.
Results
We performed thoracoscopic esophagectomy and esophagojejunostomy in the upper mediastinum for 10 consecutive patients with esophageal cancer in whom the gastric tube could not be used from 2009 onward. Six patients underwent prior gastrectomy and Billroth I reconstruction, and four had simultaneous gastric cancer that had arisen in a location in which the gastric tube could not be created after resection. The causes of prior gastrectomy included one gastric ulcer, one gastric leiomyoma, and four gastric cancers. The simultaneous gastric cancers included one case with multiple early gastric cancers in the gastric antrum and corpus and three cases with advanced or submucosal cancer that required dissection of perigastric nodes along the greater curvature by transection of the right gastroepiploic artery and vein.
The demographics of the 10 patients who underwent thoracoscopic esophagectomy with esophagojejunostomy are shown in Table 1. Although we performed additional cervical lymph node dissection for three cases with upper mediastinal lymph node metastasis, no cervical lymph node metastasis was found by pathological examination. Preoperative chemotherapy was performed in six cases with advanced esophageal or gastric cancer. No adjuvant chemotherapy was performed in any cases.
There was no conversion to thoracotomy, and we completed the procedure for all 10 patients. The median operation time, amount of blood loss, and number of dissected total and thoracic nodes was 741 (665–1019) minutes, 835 (380–2090) ml, and 59 (16–165) and 30 (10–54) nodes, respectively (Table 2). The median duration of thoracoscopic intrathoracic anastomosis was 94.5 (70–211) minutes. The median body weight loss 3 months after surgery was 13.9%. Thereafter, the patients maintained their body weight. The operative mortality and morbidity are shown in Table 3. There was no anastomotic leakage, conduit necrosis, or hospital mortality. Two cases showed delayed anastomotic stenosis. These patients were managed safely by endoscopic balloon dilation therapy.
ARDS, acute respiratory distress syndrome.
To determine the radicality of the procedure, we investigated the overall survival (Fig. 4). The median observation time was 2.83 (0.67–5.99) years. During this period, three stage III patients showed recurrence and were treated by radiotherapy. One patient died of recurrent disease 6 months after initiation of therapy. The other patients survived until present. The overall 5-year survival rate was 90% (stage I, 100% and stage III, 83.3%).
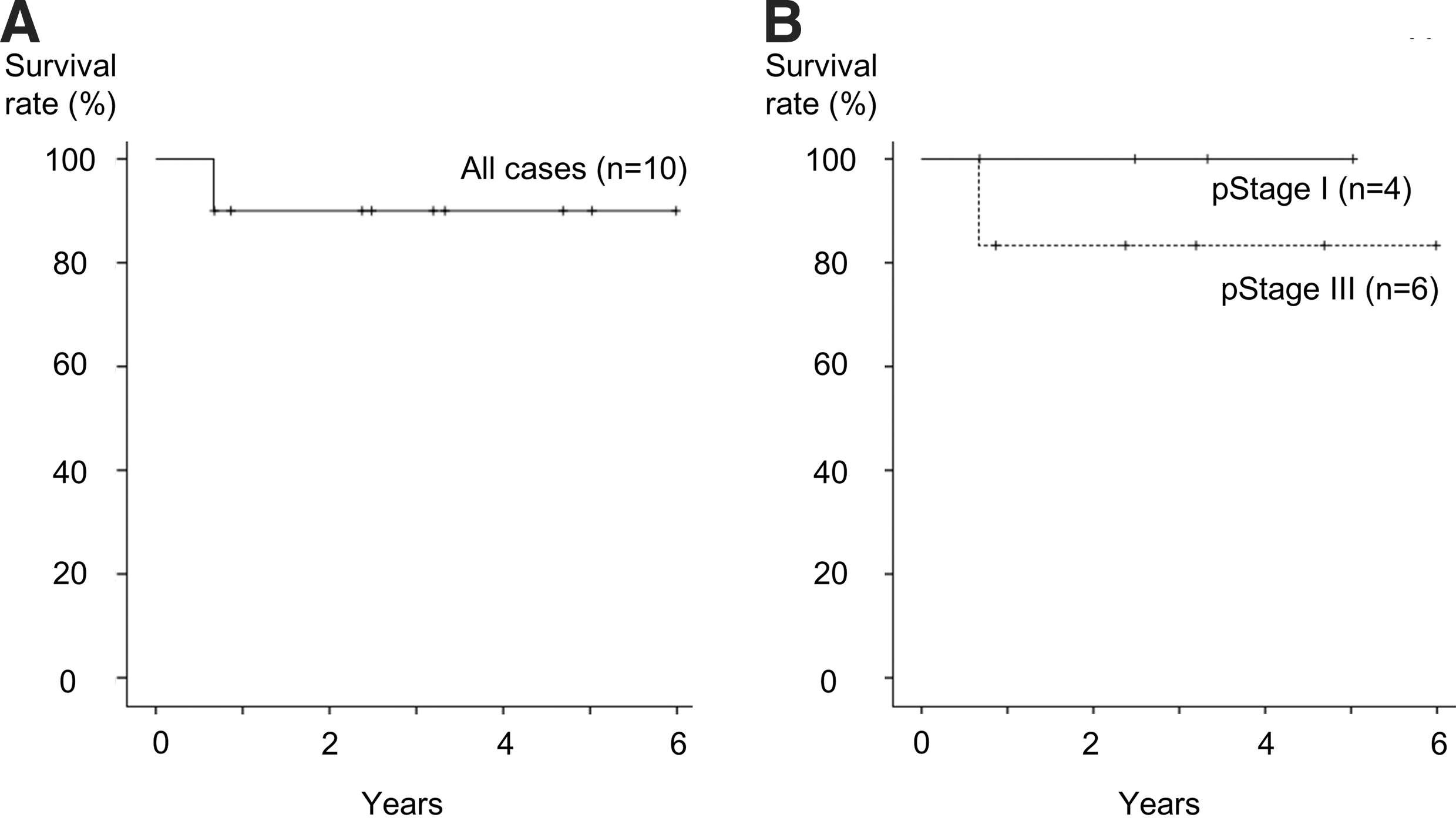
Overall survival curves of the patients who underwent thoracoscopic esophagectomy with intrathoracic esophagojejunostomy.
Discussion
We reported the surgical procedure and results of 10 cases who underwent thoracoscopic esophagectomy and total gastrectomy followed by thoracoscopic intrathoracic esophagojejunostomy in the upper mediastinum. The procedure could be done safely without conversion to thoracotomy, anastomotic leakage, or conduit necrosis.
Although surgery is the mainstay in treatment of esophageal cancer, reconstruction using an organ other than the stomach after esophagectomy is still a complex and difficult procedure. The difficulty of jejunal reconstruction is mainly attributable to the limitation in extension because of the length of the short pedicle. Generally, the first portion of the jejunum used as a graft has more than three jejunal arteries. These mesenteric vessels connect with one another, forming several short vascular loops through the collateral vessels. Therefore, several main jejunal arteries and veins must be sacrificed to create a jejunal conduit of adequate length. Previous reports showed that at least the second and third jejunal vessels must be severed to create a long jejunal graft.3–5
In our institution, we try to preserve the vascular connection between the mesenteric vessels, to create the jejunal conduit with sufficient circulation, because the connecting flow of the marginal vessels is not promising. The number of transected mesenteric vessels depends on the length of the vascular loop between each mesenteric vessel. We have transected one or two mesenteric branches in creating a pedicled jejunal conduit until present.
A further procedure to overcome the limitation of the extension length of the jejunal conduit is mobilization of the right colon and ileum from the retroperitoneum. According to this technique, elongation of the pedicled vessels can be achieved without further ligation of vascular loops between the sacrificed jejunal branches because the superior mesenteric artery and vein proximal to the pedicled jejunal vessels can be used as a portion of the pedicle. Our method overcomes two mutually exclusive events: preservation of circulation in the jejunal conduit and long extension length of the pedicled vessels of the jejunal conduit.
Intrathoracic anastomosis, first reported by Lewis 12 , is applicable in most cases of thoracic esophageal cancer because the majority of such cancers arise in the middle to lower thoracic esophagus. Recently, several methods to perform thoracoscopic esophagogastrostomy have been reported. Generally, thoracoscopic anastomosis was done using linear13–15 or circular11,16 staplers. Anastomosis by linear and circular staplers is performed by side-to-side and end-to-side anastomosis, respectively. Side-to-side anastomosis needs more length of both the esophageal stump and the conduit than end-to-side anastomosis requires. We chose circular stapling with end-to-side anastomosis to perform esophagojejunostomy in the upper mediastinum because of the limitation of the length of the esophageal stump and conduit. We placed a 25-mm anvil transorally using OrVil (Covidien) after dividing the esophagus by a linear stapler at the upper mediastinum. The oral gastric tube of the OrVil was advanced through the esophagostomy of the esophageal stump by cutting the left edge of the stump and removing it through one of the thoracoscopic ports to make double stapling. The weakest crossing point of the stapler was visible from the thoracoscope after completion of the anastomosis. The crossings of the staple lines were oversewn to reinforce the anastomosis by additional muscular suturing.
For thoracoscopic circular stapling, a previous study showed insertion of the circular stapler from the intercostal space.11,16,17 We have previously experienced such a case with a narrow intercostal space. In that case, a large thoracotomy was necessary to insert the circular stapler. We developed a new method to insert the circular stapler from the enlarged esophageal hiatus. In this technique, the jejunal conduit can be safely introduced to the upper mediastinum, and the entire anastomosis process could be easily observed by thoracoscopy. In most cases, the highest point of the elevated conduit is situated about 15 cm distal to the top end of the jejunal stump. After marking the highest point with a stitch, most of the mesenteric vascular bed of the jejunal stump distal to the stitch was dissected. Jejunal stump elongation by removal of the mesentery made it easy to hold the jejunum after insertion of the circular stapler from the jejunal stump.
Complications after jejunal reconstruction occur in the context of insufficient circulation. Therefore, additional microvascular anastomosis is advocated.3,7 However, we are convinced that intrathoracic anastomosis is the ideal route of reconstruction for jejunal conduit because that is the shortest route. Although microvascular anastomosis cannot be performed in cases of posterior mediastinal reconstruction, we safely performed intrathoracic esophagojejunostomy without anastomotic leakage or conduit necrosis. 9 In the present study, we successfully completed thoracoscopic anastomosis without anastomotic leakage, conduit necrosis, or surgical mortality. The notable complication of delayed anastomotic stenosis occurred in two cases. The stenosis could be successfully managed by postoperative endoscopic dilation therapy in these two cases. Further attention may be needed to maintain sufficient circulation in the conduit.
Mediastinal lymph node dissection was performed using the combination of a transhiatal approach in the lower mediastinum and a thoracoscopic approach in the upper and middle mediastinum. We dissected all regional mediastinal lymph nodes, including upper mediastinal lymph nodes along bilateral recurrent laryngeal nerves. The number of retrieved mediastinal lymph nodes was consistent with that in our method of radical esophagectomy. 10 However, three patients showed recurrent laryngeal nerve palsy postoperatively. Permanent palsy was found in two cases. In one case, we had to dissect the left recurrent laryngeal nerve to distinguish tumor involvement from lymph node metastasis. The suspected cause in another case was transection of unpredictable right nonrecurrent laryngeal nerve during cervical lymph node dissection. One patient showed transient palsy. Recurrent nerve palsy triggered subsequent pulmonary complications, including pneumonia and acute respiratory distress syndrome. Although avoidance of laryngeal nerve injury may be difficult under special circumstances, as in our cases, further attention to avoid recurrent laryngeal nerve palsy is needed.
Overall survival was favorable at present although 6 of 10 cases had advanced disease. Further observation is necessary to confirm the long-term survival benefit of the thoracoscopic dissection procedure.
In conclusion, thoracoscopic intrathoracic esophagojejunostomy with pedicle jejunal reconstruction can be performed safely in combination with thoracoscopic radical esophagectomy using our newly developed technique. Thoracoscopic esophagectomy with intrathoracic esophagojejunostomy can be performed as a minimally invasive surgical procedure for the esophageal cancer patients in whom the stomach cannot be used as a reconstruction conduit.
Footnotes
Disclosure Statement
No competing financial interests exist.