
Abstract
Abstract
Background:
Because laparoscopic liver resection (LLR) has a steep learning curve, analyzing experience is important for trainees. Several authors have described the learning curve of LLR, without comparing the learning curves between major and minor LLR.
Methods:
Perioperative data were retrieved from the medical records of 170 consecutive patients who underwent LLR by a single surgeon at a tertiary hospital. Learning curves were generated and compared between major and minor LLR using cumulative sum control charts and the moving average.
Results:
Major and minor LLR was performed in 96 and 74 patients, respectively. The learning curves showed a steady state after case 50 for major LLR. Because of discordant results in minor LLR, subgroup analyses were performed, showing competency in LLR after cases 25 and 35 for left lateral sectionectomy and tumorectomy, respectively. Transfused red blood cell volume (0.6 versus 2.2 packs, P < .001) decreased after achievement of competence in major LLR. Blood loss exceeding 500 mL (odds ratio 2.395, 95% confidence interval 1.096–5.233, P = .028) was independently associated with LLR failure.
Conclusions:
The number of cases required to accomplish LLR differed according to the extent of resection. Extensive blood loss was independently associated with LLR failure.
Introduction
S
One of the main methods of analyzing experience is the learning curve, which can be evaluated using the cumulative sum control chart (CUSUM) and the moving average (MA). 6 Several authors have reported learning curves for LLR, but they were not compared between different extents of liver resection. 7 Because the technical difficulties of LLR differ according to the extent of liver resection, the learning curve for LLR should be analyzed after considering the surgical extent. Furthermore, most studies compared perioperative data between two or three phases without considering the accomplishment of the learning curve. 8 Therefore, the aims of this study were to determine the number of cases taken to accomplish the learning curve for LLR and to compare the learning curves between major and minor LLR.
Methods
Patient population, study design, and data collection
We retrieved the electronic medical records of 170 consecutive patients who underwent LLR by a single surgeon at Gyeongsang National University Hospital between December 2008 and August 2015. The surgeon had extensive experience of open liver resection. Patients were divided into two groups, according to whether they underwent major or minor LLR. Minor liver resection was defined as liver resection, including one or two segments, and major liver resection was defined as liver resection of three or more segments. 4 Preoperative data included age, sex, body mass index, American Society of Anesthesiologists score, liver function tests, virologic status, and indocyanine green retention rate after 15 minutes. Intraoperative variables included the extent of liver resection, conversion to open surgery, operation time, use of the Pringle maneuver, estimated blood loss, and the number of packed red blood cells (pRBCs) transfused during surgery. Postoperative data included the type and severity of postoperative complications, pathologic diagnosis, and duration of hospital stay. This study was approved by the Institutional Review Board of Gyeongsang National University Hospital.
Surgical procedures
After induction of general anesthesia, the patient was placed in the French position and adjusted to the right or left side in the reverse Trendelenburg position according to the resection site. The endoscopist stood between the patient's legs and the assistant was on the left side of the patient. The surgeon stood on the right side of the patient. An umbilical port was used for the endoscope. Two 11 mm ports were inserted into the subcostal area and additional ports were placed in the left subcostal area for the assistant. Intraoperative ultrasonography was used to detect the tumor site and determine the adequate resection margin. In major LLR, inflow control was performed first. Minor LLR was performed after tumor detection without inflow control. The hepatic parenchyma was transected with ultrasonic shears and a Cavitron Ultrasonic Surgical Aspirator (Integra Lifesciences Corp., Plainsboro, NJ). The laparoscopic Pringle maneuver was used to minimize bleeding during parenchymal transection. After transection, we applied a fibrin-based collagen fleece onto the cut surface and placed drains around the transection site.
Statistics
The CUSUM method was initially developed to evaluate industrial processes and its main advantage is its ability to visualize a specific achievement. 9 The positive and negative slopes of the curve indicate failure and success, respectively. Previous studies defined failure as conversion to open surgery. In our study, surgical failure was expanded to include R1 resection and postoperative major complications of grade III or worse according to the Clavien–Dindo classification because of the low conversion rate (n = 5, 2.9%). CUSUM was defined as CUSUM = Σ (Xi − Xo). Xi is an individual attempt and is assigned scores of 0 or 1 for successful surgery and surgical failure, respectively. Xo is the predetermined acceptable failure rate for the procedure. The acceptable failure rate and targeted success rate were set at 10% and 90%, respectively, which were selected based on a previous study. 6 The cumulative sum was presented graphically, and accomplishment of the learning curve is depicted as a continual fall in the curve after reaching a peak.
Changes in the mean operation time and the estimated blood loss are objective methods of assessing the learning curve. However, the fluctuations in the means were too great to observe clear changes in these variables. Therefore, the MA method was used to assess changes in these variables, by creating averages of different subsets of the full data set and was defined as MA = (X0 + X1 + X2 +…+ XN)/N. N was defined as 15, after which the fluctuations started to smooth out.
Continuous data are presented as the mean ± standard deviation. The χ2 test was used to compare categorical variables and the independent-samples t test was used to compare continuous variables among the study groups. Binary logistic regression was used to identify factors associated with LLR failure. In all tests, two-sided P values of < .05 were regarded as significant. SPSS® version 21.0 (SPSS, Inc., Chicago, IL) was used for all analyses.
Results
Patient characteristics
Preoperative, operative, and postoperative characteristics of the major and minor LLR groups are shown in Table 1. Of 170 evaluated patients, 96 underwent minor LLR and 74 underwent major LLR. In terms of preoperative data, the proportion of men (68.8% versus 45.9%, P = .003), proportion of patients with an American Society of Anesthesiologists score of ≥3 (37.5% versus 13.5%, P = .001), and the mean indocyanine green retention rate after 15 minutes (17.2% versus 7.4%, P < .001) were greater in the minor LLR group than in the major LLR group. There were no significant differences in the other preoperative variables between the two groups.
Results are presented as the n (%) of patients or mean ± standard deviation.
LLR, laparoscopic liver resection; ASA, American Society of Anesthesiologists; HBsAg, hepatitis B surface antigen; HCV, hepatitis C virus; ICG-R15, indocyanine green retention rate after 15 minutes; pRBCs, packed red blood cells; HCC, hepatocellular carcinoma.
Regarding operative data, 5 (2.9%) patients were converted to open surgery because of bleeding (n = 3), severe adhesion (n = 1), and for oncologic safety (n = 1). The open conversion rate was similar in both groups. The mean operation time (291.7 versus 217.9 minutes, P < .001) and estimated blood loss (522.2 versus 402.5 mL, P = .020) were significantly greater in the major LLR group than in the minor LLR group. The mean number of pRBCs transfused during surgery was 1.4 in both groups.
Overall, 40 (23.5%) patients experienced postoperative complications. The complication rate (26.0% versus 20.3%, P = .466) and severity (14.5% versus 20.2%, P = 1.000) were not significantly different between the two groups. The mean hospital stay was 12.2 days. The most common indications for LLR were hepatocellular carcinoma (n = 81, 47.6%) and metastatic tumor (n = 18, 10.6%).
Learning curves for major and minor LLR
The treatment failure rate was 18.8% (n = 32/170). Reasons for treatment failure included conversion to open surgery, R1 resection, and development of a major complication in 5, 2, and 25 patients, respectively. The CUSUM is shown in Figure 1a. Both major and minor LLR groups showed steep decreases in the curves, and the learning curve was accomplished after 50–55 and 35–40 cases for major and minor LLR, respectively. The MA for operation time and estimated blood loss is shown in Figure 1b and c, respectively. The operation time decreased gradually and reached a steady state after cases 50–60 and 55–60 for major and minor LLR, respectively. The estimated blood loss reached a steady state after cases 50–55 and 65–70 for major and minor LLR, respectively. Based on the CUSUM and MA data, it seems the learning curve for major LLR was accomplished after ∼50 cases.

CUSUM
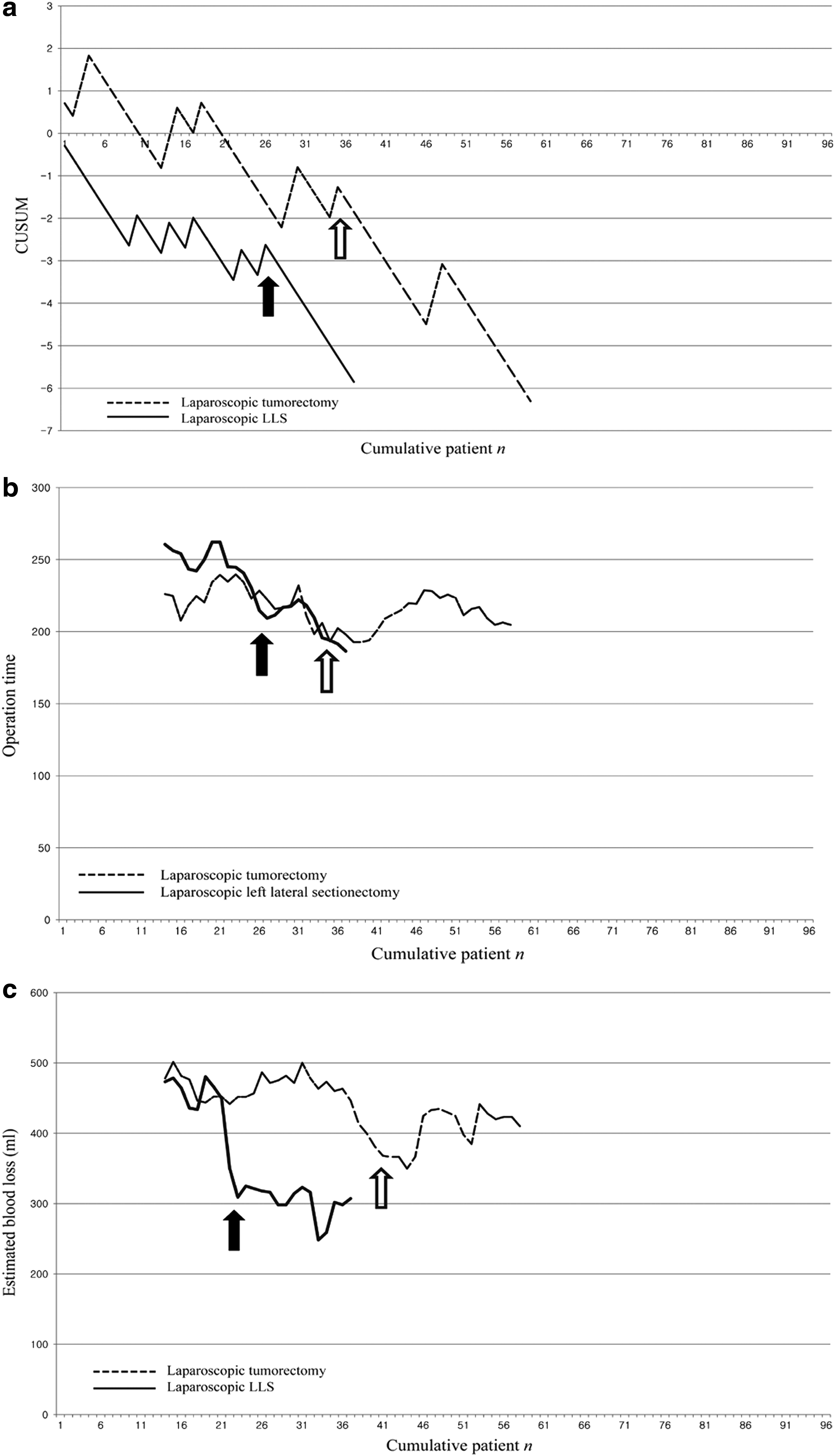
Because the accomplishment of minor LLR was discordant between the CUSUM and MA data, we performed subgroup analyses to determine the cause of this discordance. Patients were divided into two groups according to whether they underwent laparoscopic tumorectomy (n = 59) or LLS (n = 37), and the learning curves were compared between these two subgroups. CUSUM analysis showed decreases in the learning curves after cases 35–40 and 25–30 for tumorectomy and LLS, respectively (Fig. 2a). The MA for operation time reached a steady state after cases 35–40 and 20–25, and the MA for estimated blood loss reached a steady state after cases 35–40 and 25–30 for tumorectomy and LLS, respectively (Fig. 2b, c). Therefore, based on these subgroup analyses, the learning curves for tumorectomy and LLS were achieved by cases 35 and 25, respectively. These values were similar to the CUSUM for minor LLR as shown in Figure 1a.
CUSUM
Comparison of perioperative outcomes according to the accomplishment of the learning curve
Because of subjective limitations pertaining to graphical analyses, the perioperative outcomes were also compared between cases of LLR performed before (phase 1) and after (phase 2) the learning curves were accomplished according to the type of procedure. In tumorectomy, the mean age was higher in phase 2 than in phase 1 (65.6 versus 59.4 years, P = .003). However, there were no significant differences in operation time (216.2 versus 214.4 minutes, P = .932), estimated blood loss (416.4 versus 427.0 mL, P = .901), or the number of transfused pRBCs (1.1 versus 1.4 packs, P = .603) between the two phases. The postoperative outcomes were similar in both phases.
In LLS, the preoperative variables were not significantly different between the two groups. The operation time was shorter in phase 2 than in phase 1, with a difference that was marginally significant (190.8 versus 237.5 minutes, P = .065). Estimated blood loss was also less in phase 2, but the difference was not statistically significant (306.2 versus 401.0 mL, P = .362).
In major LLR, the preoperative data were not different between phases 1 and 2, except for virologic status, because hepatitis B viral infection was significantly more frequent in phase 2 than in phase 1 (20.8% versus 6.0%, P = .041). Furthermore, a greater proportion of patients in phase 2 underwent surgery for malignant disease compared with patients in phase 1 (66.0% versus 34.0%, P = .012). Blood loss (578.4 versus 405.4 mL, P = .061) and the number of transfused pRBCs (2.2 versus 0.6 packs, P < .001) were significantly greater in phase 1 than in phase 2. The postoperative complication rate, severity, and mean hospital stay were not significantly different between phases 1 and 2 for major LLR (Table 2).
Results are presented as the n (%) of patients or mean ± standard deviation.
LLR, laparoscopic liver resection; ASA, American Society of Anesthesiologists; HBsAg, hepatitis B surface antigen; HCV, hepatitis C virus; ICG-R15, indocyanine green retention rate after 15 minutes; pRBCs, packed red blood cells.
Risk factors for failed LLR
Binary logistic regression was performed to identify preoperative and intraoperative variables associated with LLR failure, which was defined as conversion to open surgery, R1 resection, or major complications. In univariate analyses, blood loss exceeding 500 mL (P = .022) and two or more transfused pRBCs (P = .025) were associated with LLR failure. In the multivariable analysis, only blood loss exceeding 500 mL (odds ratio 2.395, 95% confidence interval 1.096–5.233, P = .028) was independently associated with LLR failure (Table 3).
OR, odds ratio; CI, confidence interval; BMI, body mass index; ASA, American Society of Anesthesiologists; pRBCs, packed red blood cells.
Discussion
This study analyzed the learning curves for LLR according to the extent of the procedure. One surgeon accomplished learning curves for major LLR, LLS, and tumorectomy after 50, 25, and 35 cases, respectively. Operation time, intraoperative blood loss, and the number of transfused pRBCs decreased in phase 2, after accomplishing the learning curve. Intraoperative blood loss exceeding 500 mL was independently associated with LLR failure.
Although LLR is widely performed, the most frequent types of LLR are tumorectomy and LLS. 10 Major LLR is still reserved for experienced surgeons because the surgeon needs sufficient experience to perform delicate procedures, including clarifying anatomical variation, dissection of the hepatic hilum, inflow control, parenchymal dissection of cirrhotic liver, and management of critical intraoperative bleeding or bile leakage.4,10 Therefore, it is essential to monitor and analyze the outcomes of LLR for training purposes. 11 The most widely used methods for analyzing the learning curve are CUSUM and MA. 9 These approaches have advantages in terms of visually identifying the point of accomplishing the learning curve. 12 In medical fields, learning curves have been used to evaluate progress in achieving competence in endoscopic ultrasonography, colonoscopy, endovascular abdominal aortic aneurysm repair, and advanced laparoscopic surgery.12–16
CUSUM analysis was performed with a target success rate of 90%, and the criteria for LLR failure were conversion to open surgery, R1 resection, or major complications of grade 3 or worse according to the Clavien–Dindo classification. In earlier studies, LLR failure was defined as conversion to open surgery and its rate ranged from 2.4% to 17.2%. 11 Because the conversion rate was low in our study, we included other variables with conversion to open surgery, as in an earlier study, which reported the learning curve of laparoscopic colectomy. 6
In our study, the learning curves for major LLR, LLS, and tumorectomy were accomplished after 50, 25, and 35 cases, respectively. Similar results were reported in previous studies. For example, Nomi et al. also used the CUSUM to analyze operation time, which reached a steady state after 45 cases in major LLR. 11 In a study using the difficulty scoring system for LLR, 50 cases were suggested to be the minimal number for high-level LLR. 5 The present study also revealed that the CUSUM and the MA for operation time and blood loss reached steady state after 50 cases in major LLR. However, the learning curve for minor LLR is controversial. Although Vigano et al. reported that 60 cases was the smallest number for safe minor LLR, other studies suggested that 15–43 cases were required to overcome the learning curve for minor LLR.7,17–19 We also observed discordant results between the CUSUM and MA analyses for minor LLR. Therefore, we performed subgroup analyses after dividing the patients into those who underwent tumorectomy or LLS. The learning curves for LLS and tumorectomy were reached after 25 and 35 cases, respectively. Contrary to our expectations, the learning curve for laparoscopic tumorectomy was high. Some reasons are that patients who underwent parenchyma-sparing tumorectomy have liver cirrhosis and surgery was performed in posterosuperior segments, which led to greater blood loss and longer operation time.20,21
The ability to visualize the learning process is an advantage of the CUSUM and MA methods. However, determining the exact point of accomplishment is subjective. Therefore, we compared the perioperative outcomes between patients in phases 1 (i.e., before accomplishing the learning curve) and 2 (i.e., after accomplishing the learning curve). In major LLR, a greater proportion of patients in phase 2 had malignant disease compared with patients in phase 1. Estimated blood loss was lower in phase 2, with marginal significance, and the number of pRBCs transfused decreased significantly in phase 2 compared with phase 1. As previously reported, accomplishment of the learning curve was associated with improved outcomes such as decreased operation time, lower conversion rate, reduced blood loss, fewer postoperative complications, and shorter hospital stay. 7 Furthermore, several studies showed that risk factors for conversion to open surgery included major LLR and use of the Pringle maneuver.7,11,21 The present study revealed that the estimated blood loss was associated with failed LLR. Therefore, to safely perform LLR, it is important to consider whether the surgical technique and extent are appropriate for the surgeon's experience and the patient's characteristics. Furthermore, reducing intraoperative blood loss using Pringle's maneuver or by performing meticulous parenchymal transection is essential to avoid conversion to open surgery or major complications.
This study has several limitations. In particular, the analyses were limited to procedures performed by a single surgeon. Because there may be interindividual variability in achieving the learning curve of LLR, we must also consider the experience of other surgeons to establish learning curves for LLR. In addition, the number of evaluated patients was too small to show significant differences between phases 1 and 2 in laparoscopic tumorectomy or LLS.
Conclusion
Based on the results of this study, the necessary number of cases to achieve a stable learning curve for LLR differs according to the extent of liver resection. Our results suggest that a surgeon needs to perform LLR in 50, 25, and 35 cases for major LLR, LLS, and tumorectomy, respectively. Intraoperative blood loss exceeding 500 mL was independently associated with LLR failure. These findings suggest the need to establish a comprehensive training protocol for LLR and to standardize the key LLR procedures. Furthermore, clinical trials of LLR need acceptable criteria for experienced surgeons.
Footnotes
Disclosure Statement
No competing financial interests exist.