
Abstract
Abstract
Background:
There is no consensus on the optimal technique for hiatal hernia (HH) repair, and considerable recurrence rates are reported. The aim of this study was to evaluate the perioperative outcomes, quality of life (QoL), and recurrence rate in patients undergoing robot-assisted laparoscopic HH repair.
Materials and Methods:
All patients who underwent robot-assisted laparoscopic HH repair between July 2011 and March 2015 were evaluated. The procedure consisted of hernia sac reduction, crural repair without mesh, and Toupet fundoplication. Postoperative radiological imaging or endoscopy was performed in all symptomatic patients to exclude recurrence. Perioperative results were collected retrospectively from the patient records. QoL was evaluated with Short Form-36 (SF-36), Gastroesophageal Reflux Disease–Health-Related Quality of Life (GERD-HRQOL), and Gastrointestinal Quality of Life Index (GIQLI) questionnaires.
Results:
A total of 40 patients were identified. The majority (75%) had a type III HH. Median operation time was 118 (62–173) minutes; median blood loss was 20 (10–934) mL, and one procedure was converted to an open procedure. In 6 (15%) patients, postoperative complications occurred, including 2 grade II and 1 grades I, III, IV, and V, according to the Clavien–Dindo classification. Median hospital stay was 3 (1–15) days. At a median follow-up of 11 months, radiological imaging was performed on indication in 12 (30%) patients, and 1 recurrence was found. Overall QoL scores were satisfactory, and there was no difference related to the time elapsed since surgery.
Conclusion:
Robot-assisted laparoscopic HH repair followed by Toupet fundoplication demonstrated a very low short-term recurrence rate. Postoperative morbidity was minimal, and a satisfactory QoL was achieved.
Introduction
F
The use of robot-assisted laparoscopic surgery (RAS) has increased in the last few decades for a variety of surgical procedures. It is suggested that RAS allows surgeons to operate more precisely during difficult procedures compared to conventional laparoscopy due to the three-dimensional view and the enhanced manipulation of instruments. 3 Only a few studies evaluated RAS for HH repair, showing promising initial results.4–7 Unfortunately, these studies did not standardize their intraoperative techniques. The aim of this study was to evaluate robot-assisted laparoscopic HH repair without mesh, followed by a Toupet fundoplication with regard to recurrence, perioperative outcomes, and quality of life (QoL).
Materials and Methods
Patients
All patients with radiological or endoscopic confirmation of HH and treated with robot-assisted laparoscopic HH repair between July 2011 and March 2015 were evaluated. During this study period, all consecutive patients who underwent elective surgical HH repair were operated with RAS. Patients undergoing redo surgery or emergency repair were excluded. Patients with type I HH only underwent surgery when symptomatic. Baseline characteristics and presenting symptoms were collected retrospectively from the electronic patient records. HH type (I–IV), length (distance between the z-line and the diaphragmatic impression), and size (proportion of the stomach located in the thorax) were scored by reviewing the radiological, upper endoscopic, and perioperative findings. Institutional Review Board approval was obtained, and informed consent requirement was waived for this study.
Surgical procedure
All patients underwent robot-assisted laparoscopic HH repair without mesh reinforcement combined with a Toupet (270° posterior) fundoplication. Surgery was performed by an experienced robotic upper gastrointestinal surgeon (J.P.R. or R.v.H.) and conducted with the da Vinci™ Surgical System (Intuitive Surgical, Sunnyvale, CA).
Patients had general anesthesia and were placed in a supine position. A nasogastric tube was placed to decompress the stomach. After sterile exposition and open introduction, a 12-mm blunt-tip port was placed in the upper abdominal midline, and a pneumoperitoneum was established. A 30° scope was inserted, followed by three robotic ports and one laparoscopic assistant port (Fig. 1). The da Vinci arms were docked to the camera port and the robotic ports.
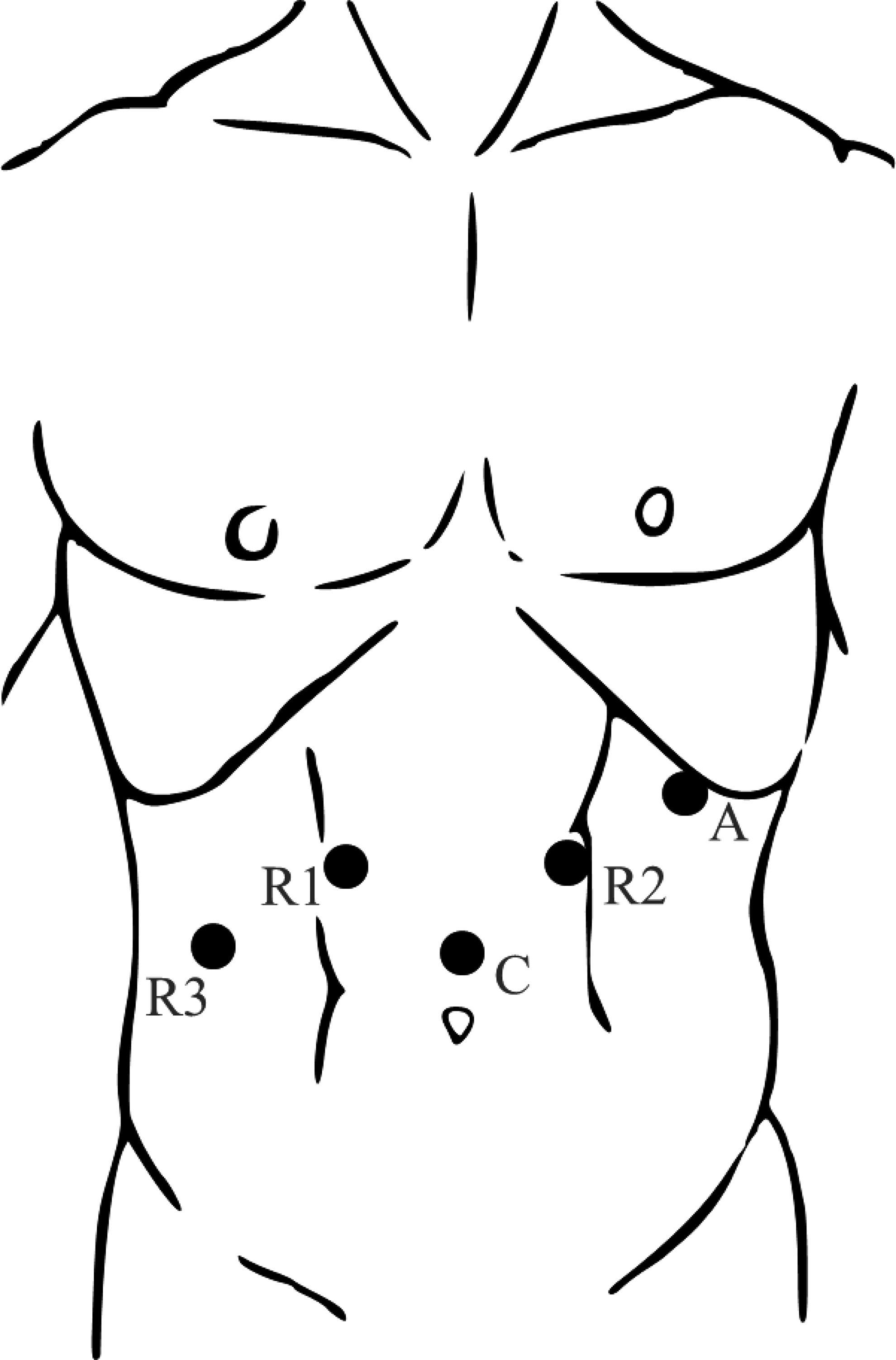
Trocar placement. A, assistant port; C, camera port; and R1, R2, and R3, robotic ports.
The first step was to establish adequate exposure of the surgical area. Liver retraction was performed, and the omental bursa was opened at the lesser omentum. The next step was to remove the hernia sac and stomach from the mediastinum. The hernia sac was dissected completely from the mediastinal structures but not excised. The mediastinal esophagus was mobilized up to the level of the pulmonary vein to obtain enough esophageal length to pull the stomach back into the abdomen. An esophageal lengthening procedure was not performed in any of the patients. The vagal nerves and aorta were identified and preserved. The short gastric arteries and fat pad overlying the gastroesophageal junction were preserved.
Next, the hiatal defect was repaired by posterior approximation of the left and right crus with three Mersilene-0 sutures without using a mesh. In addition, a Toupet fundoplication (270° posterior) was performed. The fundus was attached to the esophagus bilaterally and the right crus with three Mersilene-0 sutures. Finally, the hemostasis was checked; the ports were removed under direct vision, and fascia and skin were closed.
Perioperative outcomes
Intraoperative outcomes were operating time (minutes), blood loss (mL), and conversions. The operating time included the docking time but excluded the setup and demounting time of the da Vinci system. After surgery, the nasogastric tube was removed. On the first postoperative day, patients were given oral liquids and stimulated to mobilize. Normal diet usually started on the second postoperative day. Patients could be discharged from the hospital after complete mobilization and adequate pain control. Postoperative outcome values were operation-related complications, hospital stay (days), reoperation within 30 days, and mortality. Complications were scored using the Clavien–Dindo classification. 8
Follow-up
Patients had regular follow-up 6 weeks after hospital discharge at the outpatient clinic. Patients were discharged from regular follow-up if symptoms were absent. Any symptom (reflux, dysphagia, or pain) was considered a reason for imaging or endoscopy. Only in completely asymptomatic patients, additional investigations were abandoned. Recurrence was defined as a radiological or endoscopic confirmed HH. QoL was evaluated ≥3 months after surgery with three validated questionnaires. The first was the Short Form-36 (SF-36) questionnaire used for general QoL. The second was the Gastrointestinal Quality of Life Index (GIQLI) questionnaire used for gastrointestinal-specific QoL. The third was the Gastroesophageal Reflux Disease–Health-Related Quality of Life (GERD-HRQOL) questionnaire used for reflux-specific QoL.9–14 Patients who were unable to speak or read were excluded from QoL evaluation.
Statistical analysis
Data were analyzed using the IBM SPSS Statistics Version 20 for Windows. Median values and range were calculated for continuous variables with an abnormal distribution and for the QoL questionnaires. Percentages were calculated for dichotomous variables. The Mann–Whitney U test was used for nonparametric data. Data were considered significant if P < .05.
Results
Patients
A total of 40 patients underwent robot-assisted laparoscopic HH repair without mesh, followed by a Toupet fundoplication during the selected period. Baseline characteristics and the presenting symptoms are presented in Table 1. Median age was 62 (26–80) years; 14 (35%) patients were male, and median body mass index was 27.0 (21.3–40.7) cm/kg2. The majority of the patients had an American Society of Anesthesiologists (ASA) score of 2 (68%). The most common presenting symptom was reflux (58%), followed by dysphagia (55%). Upper endoscopy was the most commonly used diagnostic modality (93%), followed by computed tomography (CT; 50%). Most patients (83%) had a paraesophageal hernia (PEH), and the most prevalent hernia (75%) was a type III hernia. The majority (24/40, 60%) of patients had an HH with more than 50% of the stomach in the thorax. Hernia length and size are shown in Table 2.
Values are presented as median (range).
ASA, American Society of Anesthesiologists; BMI, body mass index.
Distance between the z-line and the diaphragmatic impression.
Proportion of the stomach located in the thorax.
PEH, paraesophageal hernia.
Perioperative outcomes
Perioperative outcomes are presented in Table 3. Conversion to an open procedure occurred in 1 (2.5%) patient due to intraoperative splenic injury, which was managed spleen preserving. Median operation time was 118 (62–173) minutes, and median blood loss was 20 (10–934) mL. Median duration of hospital stay was 3 (1–15) days. In 6 (15%) patients, postoperative complications occurred: 1 patient had a lung atelectasis (grade I), 2 had a wound infection (Clavien–Dindo grade II), 1 had a trocar hernia (Clavien–Dindo grade III), 1 had a mediastinitis (Clavien–Dindo grade IV) based on an infected seroma (CT scan, endoscopy, and diagnostic laparoscopy did not show a perforation), and 1 had a perforation of the cecum leading to death (Clavien–Dindo grade V). The patients who had the trocar hernia, mediastinitis, and perforation of the cecum needed a reoperation within 30 days. Autopsy and a multidisciplinary team meeting concluded that the case in which postoperative death occurred was most probably caused by the patients' history of chronic laxantia use and not related to the HH surgery.
Results are presented as median (range).
Follow-up
Median follow-up time was 11 (0–39) months. Postoperative imaging was conducted in 12 (30%) symptomatic patients. Five (12.5%) patients had a CT scan, 2 (5.0%) patients had upper endoscopy, and 5 (12.5%) patients had both. Recurrence was found in 1 patient (2.5%), presenting with symptoms of reflux, and could be managed conservatively with antiacidial drugs. The use of antacids or acid reducers was less common in the postoperative phase compared to the preoperative phase (42% versus 94%, P < .001).
Quality of Life
The questionnaire response rate was 87.5% (35/40 patients). Patients not able to complete the questionnaires had an intellectual disability (n = 2), were deceased (n = 1), or did not respond (n = 2). The median GIQLI (gastrointestinal-specific QoL) score was 112 (range 56–141), and median SF-36 (general QoL) physical condition score and mental condition score were 38.1 (range 20.6–57.8) and 56.6 (range 25.5–66.8), respectively, and the median GERD-HRQOL (reflux-specific QoL) score was 4.0 (range 0–21). No significant difference in QoL related to the time elapsed since surgery was demonstrated (Table 4).
Values are presented as median (range).
GERD-HRQOL, Gastroesophageal Reflux Disease–Health-Related Quality of Life; GIQLI, Gastrointestinal Quality of Life Index.
Discussion
This study demonstrated a low clinical recurrence rate of robot-assisted laparoscopic HH repair, followed by a Toupet fundoplication after a follow-up of 11 months. Furthermore, perioperative outcomes, such as blood loss, operation time, morbidity, and QoL scores, were satisfactory.
Following surgical HH repair, a considerable recurrence rate remains the most important postoperative problem. The recurrence rate of 2.5% found in this study is lower than that reported in a recent meta-analysis on conventional laparoscopic HH repair, which reported a recurrence rate between 10% and 26%. 2
A possible explanation for the low recurrence rate could be the use of RAS for HH repair. This allowed for a precise dissection of the complete hernia sac from the mediastinum. With conventional laparoscopic instruments, the freedom of motion of the surgeon's hand is limited during this step in the procedure since all instruments have to work through the opening in the diaphragm and therefore are in a parallel position comparable to single-incision surgery. 15 RAS allows surgeons to operate with greater ease due to the three-dimensional view and the enhanced manipulation.3,16 Therefore, complete mobilization of the esophagus up until the level of the pulmonary veins is possible. In our experience, adequate mobilization of the esophagus obviates the use of an esophageal lengthening procedure. Furthermore, the suturing of the crural repair and fundoplication is well facilitated by robotic assistance. The only other study that evaluated HH recurrence rate following RAS conducted by Draaisma et al. reported a recurrence rate of 12.5% 1 year after surgery. 6 However, it needs to be stressed that in their study, a routine radiological follow-up was performed in all patients and fundoplication was not a standard procedure. In the current study, radiological imaging was only performed when patients were symptomatic. This protocol was chosen since a previous study showed that in only 20%–30% of the patients with a radiographic recurrence a reoperation was needed, which was primarily driven by the degree of symptoms. 13
Another explanation for the low recurrence rate could be the intraoperative techniques used.17,18 Considering there is no consensus on the preferred fundoplication type during HH repair, 1 this study performed a Toupet fundoplication in all procedures. In contrast to a Nissen fundoplication, which is the predominantly used fundoplication in other studies on HH repair, we attach the Toupet fundoplication to the crus.6,19–21 Attaching the fundoplication to the crus could act as a buttress and therefore support the HH repair and prevent recurrence by anchoring the stomach in the abdomen. In addition, the telescope phenomenon, as occasionally described following Nissen fundoplication, cannot occur following a Toupet fundoplication. 22
Regarding the use of a mesh during HH repair, the literature is not conclusive.23,24 In the present study, no mesh was used. Since the Toupet fundoplication is attached to the crus, it may act as a buttress for the diaphragm, diminishing forces on the sutured cruroplasty. Therefore, performing a Toupet fundoplication after an adequate sutured cruroplasty obviates the use of a mesh.
The perioperative results in the current study were similar to those of other studies on HH repair5,6,19 with comparable blood loss, operation time, and morbidity rates. Regarding QoL, this study reported a gastrointestinal-specific QoL (GIQLI) comparable to a study on laparoscopic HH repair but lower than the general population.14,21 Furthermore, the general QoL (SF-36) physical component was lower and the mental component was higher compared to a study on laparoscopic HH repair. 19 Last, the reflux-specific QoL (GERD-HRQOL) was comparable to one study on RAS for HH repair. 6 This study presented 1 (2.6%) case of in-hospital mortality in a patient with a type IV hernia and ASA III. Death occurred after perforation of the cecum diagnosed on postoperative day 8 not related to the hernia repair surgery. The mortality rate in this study is comparable to that of a large retrospective study (n = 662) on laparoscopic HH repair, which reported an in-hospital mortality of 1.7%. 19
Due to the retrospective design of this study, several limitations should be discussed. First, this study has a relatively small study population. Nevertheless, this is the second largest cohort described in the literature on robot-assisted laparoscopic HH repair and the only one with a standardized operative procedure. Second, this study included patients with type I hernia, whereas other studies only included patients with PEHs.6,19–21 We chose to include patients with type I hernia if they were symptomatic and underwent the same procedure (primary HH repair and Toupet fundoplication) as the PEHs, thus allowing to evaluate perioperative outcomes similarly. Third, regarding the fact that recurrent HH can occur years after surgery, the follow-up in this study was relatively short (<1 year). 19 Furthermore, no control group was available in this study, which makes it difficult to compare the results to studies on laparoscopic HH repair or other intraoperative techniques. Last, QoL was not measured preoperatively, and therefore, no baseline comparison could be made.
To further investigate the use of RAS for HH repair, more research is needed. Ideally, future studies should standardize their intraoperative techniques. Furthermore, these studies should include a cost-effectiveness analysis and a surgeon ergonomics questionnaire to feed the ongoing debate of the additive value of RAS. Due to the relatively low incidence of HH, these trials should have a multicenter character.
In conclusion, robot-assisted laparoscopic HH repair demonstrated low short-term recurrence rates with morbidity and QoL comparable to the literature on laparoscopic repair.
Footnotes
Acknowledgments
All authors have contributed to the article and reviewed the article before submission. The authors state that they had full control of the design of the study, methods used, outcome parameters and results, analysis of data, and production of the written report.
Disclosure Statement
No competing financial interests exist.