
Abstract
Abstract
Background:
Jejunal diverticulitis is a rare clinical entity often overlooked by physicians as a cause for abdominal pain. Although diagnostic capabilities improved in recent years, there is little data about diverticular disease in the proximal small bowel. The aim of this study is to present the clinical course and management in a series of eight cases of jejunal diverticulitis and possible therapeutic interventions.
Methods:
A cohort retrospective analysis of all patients admitted for acute jejunal diverticulitis between January 2010 and June 2015 was conducted. Patient demographics, clinical, and surgical outcome were recorded and analyzed.
Results:
Eight patients were admitted for acute jejunal diverticulitis with a mean age of 72.1 (range 55–87) years. Clinical presentation included six patients (75%) with a sealed perforation and only one patient demonstrated distant pneumoperitoneum. All patients were treated initially without surgery and only one patient required surgery because of diverticular complications. Recurrent episodes occurred in two patients (25%). Colonoscopy was performed in all patients after hospitalization that revealed large bowel diverticulosis in all patients (100%). Median follow-up was 8.2 months (3–15 months).
Conclusion:
Jejunal diverticulitis can be initially treated conservatively but complicated disease should be considered for surgical management. Further study is required on the relationship between small and large bowel diverticulosis.
Introduction
I
There is little data about the cause of jejunal diverticulitis, and clinical presentation can vary. The improvement in diagnostic imaging technologies, mainly computerized tomography (CT), contributes to the diagnosis of this rare entity, but there is lack in management recommendations. The dramatic changes in treatment paradigms of large bowel diverticulitis in recent years may reflect treatment modalities for jejunal diverticulitis.
The aim of this study is to report our experience with management of jejunal diverticulitis and to review the current literature about this rare clinical entity.
Patients and Methods
All patients admitted to the hospital for acute diverticulitis between January 2010 and June 2015 were entered into a retrospective database. Patients admitted for diverticulitis were identified from the hospitals' medical records. The database was reviewed for patients admitted for jejunal diverticulitis; eight patients admitted for jejunal diverticulitis were identified, and their charts were retrospectively reviewed for dual graphics and clinical characteristics, imaging reports, treatment, length of stay, and postdischarge follow-up. Imaging studies reviewed by a radiologist confirmed the diagnosis of jejunal diverticulitis and associated complications.
The study was approved by the local Institutional Review Board.
Results
Out of 325 patients admitted for acute diverticulitis between January 2010 and June 2015, eight patients (0.02%) admitted for jejunal diverticulitis were identified, four males and four females, with a mean age of 72.1 years (range 55–87). Patients' demographics and Charlson score of comorbidities are outlined in Table 1.
BMI, body mass index.
All eight patients presented with abdominal pain, most commonly left upper quadrant and periumbilical pain, and underwent a CT, confirming the diagnosis of jejunal diverticulitis (Figs. 1 and 2).
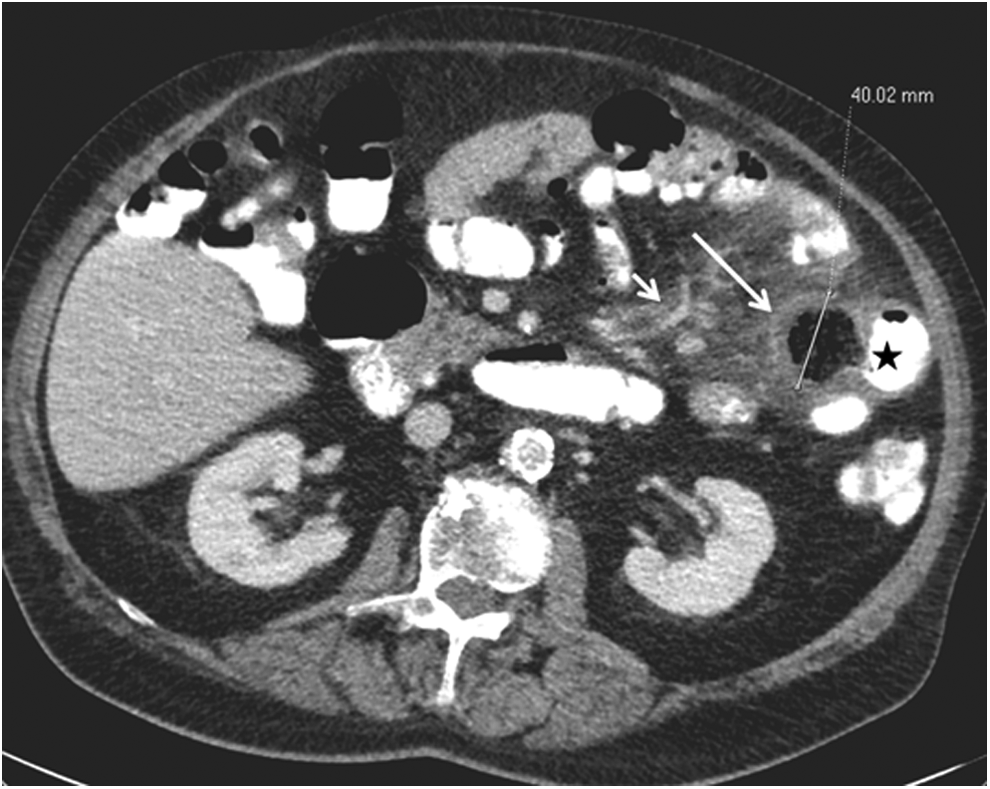
Seventy-nine-year-old patient that presented with left upper quadrant pain and leukocytosis. Axial CT slice postoral and intra-venous contrast administration demonstrated a 4 cm diverticula (long arrow) adjacent to mid jejunum bowel loop (star). Marked mesenteric fat stranding, enlarged lymph node, and blood vessel congestion are seen (short arrow).

Coronal CT slice of the same patient, showing the inflamed diverticula (long arrow).
All patients were assessed by a surgeon in the emergency department and half of patients presenting with signs of local peritonitis and elevated white blood cell (WBC) count and C-reactive protein (CRP) were common (WBC, mean 13.7, range 7.4–26). All patients underwent a CT scan on admission, and the diagnosis of jejunal diverticulitis was based on imaging findings and clinical presentation. CT findings demonstrated multiple small bowel diverticula in five patients (62.5%) with a sealed perforation in six patients (75%). All patients were treated with IV antibiotics, NPO, and fluid support with resolution of symptoms in seven out of eight patients (87.5%) without the need for surgical intervention. Length of stay averaged at 6.75 days. One patient presented with jejunal diverticulitis and a liver abscess, presumably originating from the small bowel inflammation and needed a percutaneous drainage. After drainage, the liver abscess reduced in size and the patient was discharged. One month later, the patient was readmitted because of abdominal pain; an enlarged intraabdominal abscess between jejunal bowel loops and enlargement of the liver abscess were seen in a repeated CT scan. The patient was taken to the operating room where a small bowel resection was performed with primary anastomosis.
All patients were followed up for a mean period of 8.2 months (range 3–15 months) and routine colonoscopy was recommended to all patients. All patients (100%) were found to have large bowel diverticulosis. CT enterography was performed in five patients (62.7%) as part of their follow-up. Two patients (25%) suffered from repeat abdominal pain and surgery was discussed, and nonsurgical management with follow-up only was selected in both cases. Both did not suffer further complications.
Discussion
Small bowel diverticula are commonly seen in the duodenum and the ileum. Jejunal diverticulosis is the rarest type, consisting only of 18% of small bowel diverticula. 1 Although the exact cause of jejunal diverticula is unclear, it has been potentially linked to intestinal dysmotility disorders, 2 previous surgery,3,4 and obstructing enteroliths.5–7
Although often asymptomatic, clinical manifestations of jejunal diverticulosis may include abdominal pain, changes in bowel habits, and malabsorption. 8 Jejunal diverticulitis usually manifests with abdominal pain, local tenderness, and systemic signs of inflammation such as elevated WBC count and CRP. In our series, peritoneal irritation signs were found on physical examination in half of the patients. Jejunal diverticulitis may present with complications, including intestinal perforation, abscess, fistula, and gastrointestinal bleeding.1,9 Intestinal obstruction is a rare complication that may be related to motility disorders. 10 Liver abscess is mentioned in one report in the literature, where Hoover et al. described a patient with hematogenous spread from a perforated jejunal diverticulitis, 11 similar to the case we presented. In our report, we describe a liver abscess because of jejunal diverticulum, which was treated with percutaneous drainage effectively resolving the liver abscess. Eventually, surgery was required for the jejunal diverticulum.
Prior to the introduction of CT scans, diagnosis of jejunal diverticulitis was difficult and relied mainly on barium studies, 12 and complications of jejunal diverticula such as inflammation, abscess, and perforation were mainly diagnosed at surgery. The increased use of CT scans led to improved diagnostic results, turning the CT scan into the gold standard diagnostic means for discovering jejunal diverticula and their complications.13–15 The impact of CT scans on diagnosis led to a more conservative approach in treatment, which is nowadays the standard of care for uncomplicated jejunal diverticulitis. 16 In our series, we have found that all patients with jejunal diverticulitis were also found to have large bowel diverticulosis. This could perhaps be related to the suggested etiology for diverticula of the small bowel that may be correlated with intestinal motility disorders.
The management of jejunal diverticulitis is still controversial, with various results in the literature. Most publications are case report and the lack of large clinical studies makes the choice of the therapeutic regimen difficult. Reviewing the literature in recent years shows that similarly to the trends in the treatment of large bowel diverticulitis, nonsurgical management of jejunal diverticulitis is often selected in cases without free perforation. 17 Spasojevic et al. 18 reviewed past series and compared operated patients with patients treated without surgery and demonstrated satisfactory results with the nonsurgical treatment. Kouraklis et al. 9 recommended that patients with chronic refractory symptoms, including pain and gastrointestinal bleeding, should be offered elective surgery with resection and primary anastomosis, which showed good surgical outcome. 19 This policy should be reconsidered in cases having long effected segments of small intestine with multiple diverticula. Complicated and urgent cases warrant a more aggressive approach, including emergent surgery in patients with free perforations of the small bowel and in patients with diffused peritonitis or clinical instability. These patients usually undergo primary resection with or without anastomosis,8,20 but a more recent series suggested laparoscopic lavage and drainage as a possibility in some cases with sealed perforation without obstruction or fistula. 18 Complicated cases warrant surgery, but these can have severe postoperative complications,21,22 including significant morbidity and mortality rates,18,23 similar to the outcome of the single patient who underwent surgery in our series.
In the current series, nonsurgical management was chosen for all patients initially, with good clinical outcomes. Except for one patient with a liver abscess and recurrent jejunal abscess, all other patients were treated without surgery. On longer follow-up, surgery was considered in two additional cases because of continuing abdominal pain. Our series supports the nonoperative approach in patients without significant complications.
Based on the favorable results of nonoperative management in this series, and in line with the previous report of Spasojevic et al., 18 we believe that the nonoperative approach should be considered initially in patients with jejunal diverticulitis without major complications. CT scan is a useful imaging tool in the diagnosis of jejunal diverticulitis and its complications, and can help to distinguish between uncomplicated diverticulitis of the jejunum and complications that require emergent surgery. Despite being one of the largest series in the literature, the number of patients in this series is too small to draw firm conclusions, and the retrospective nature of this study may also impact the results and level of recommendation. Another limitation is the difficulty in identifying patients with jejunal diverticulitis, as not all patients presenting with abdominal pain undergo CT scans for diagnosis, possibly blurring the real incidence rate. Multicenter prospective studies should help determine the proper treatment of jejunal diverticulitis in the future, although those are unlikely because of low incidence. Another alternative is population based studies to help determine better management recommendations.
Conclusion
Jejunal diverticulitis is a rare entity and may often be treated without surgery. Complicated cases as well as refractory cases with continuing symptoms often require surgery. Large multicenter studies should determine treatment paradigms in patients with diverticulitis of the jejunum.
Footnotes
Disclosure Statement
No competing financial interests exist.