
Abstract
Abstract
Sleeve gastrectomy operations have become popular among restrictive obesity surgeons, due to its effectiveness for losing weight and acceptable complication rates. However, leakage is a significant problem in these operations. In this ex vivo study, we tried to understand mechanisms of leakage and to examine the effects of two different types of frequently referred reinforcement techniques using sutures. The resected gastric specimens that were removed during sleeve gastrectomy operations were used in this ex vivo study. Foley catheters were inserted to stomach from two different areas along the greater curvature of stomach, and one of these catheters was connected to monitoring apparatus with intra-abdominal pressure measurement system. The other Foley catheter was connected to syringe apparatus with 1000 cc physiological saline. No reinforcement procedure was applied to staple line in the first group. In the second group, staple line was sutured continuously with 2/0 knotless absorbable suturing material. In the third group, continuous suturing was applied using 2/0 knotted absorbable sutures. Next, stomach was filled with physiological saline, and the site of leak and the pressure value at the level of leakage were noted. Pressure values that caused leakage in no reinforcement suture, knotless suture, and knotted suture groups were 42.7 (±1), 98.7 (± 3.9), and 97.7 (±4.1) mmHg, respectively. The pressure difference between the groups was statistically significant (P = .000). As for the site of leaks, 26 (58%) were in corpus, 14 (31%) were in antrum, and 5 (11%) were in fundus, and there was no significant difference between the groups in terms of leakage sites (P = .97). In sleeve gastrectomy operations, reinforcement of staple line using either knotless or knotted sutures may help to prevent leakage.
Introduction
S
Materials and Methods
This study was initiated following its approval by Kecioren Training and Research Hospital's Ethics Committee. The study group was selected among individuals aged between 18 and 60 years old who were registered for sleeve gastrectomy by the surgical team after their application to Kecioren Training and Research Hospital's General Surgery Clinics for obesity surgery. All participants have signed informed consent form, declaring their voluntary participation in the study. Those who had connective tissue diseases or those whose gastric tissues were damaged during removal in the operation were excluded from the study. For each case, age, sex, height, weight, and additional disease information were recorded.
Without any delay following removal of the specimens, they were measured for height, width at upper third (fundus), width at middle third (corpus), and width at lower third (antrum). Width measurements were performed from the middle of the section that is being measured. Two incisions, 0.5 cm each, were made at greater curvature of the stomach, away from the staple line for insertion of Foley catheters. The surrounding area was sutured with 2/0 silk purse-string suture. The balloons of Foley catheters were filled with 5 cc physiological saline solution and Foley catheters fixated. One of the Foley catheters was attached to AbViser® intra-abdominal pressure measurement system and Nihon Kohden® monitoring apparatus. The other Foley catheter was connected to 1000 cc physiological saline using AbViser syringe apparatus (Fig. 1). Groups were determined randomly. No reinforcement was applied in the first group. In the second group, staple line was sutured continuously with 2/0 knotless poliglactin absorbable suturing material. In the third group, continuous suturation was made using 2/0 knotted poliglactin absorbable suturing material. Serosal to serosal Lembert suture was performed by the same surgeon in suture groups (knotless and knotted). In this procedure, our aim was to imbricate the serosal surfaces to cover the staple line. Next, stomach was filled with physiological saline, 0 mmHg pressure level was adjusted, and the apparatus was clamped below the measurement transducer. Then, while filling the stomach with physiological saline, site of leakage was detected and recorded as upper third (fundus), middle third (corpus), and lower third (antrum); and the pressure level causing leakage was recorded (Figs. 2 and 3).

Pressure mechanism with AbViser® intra-abdominal pressure measurement system and Nihon Kohden® monitoring apparatus.
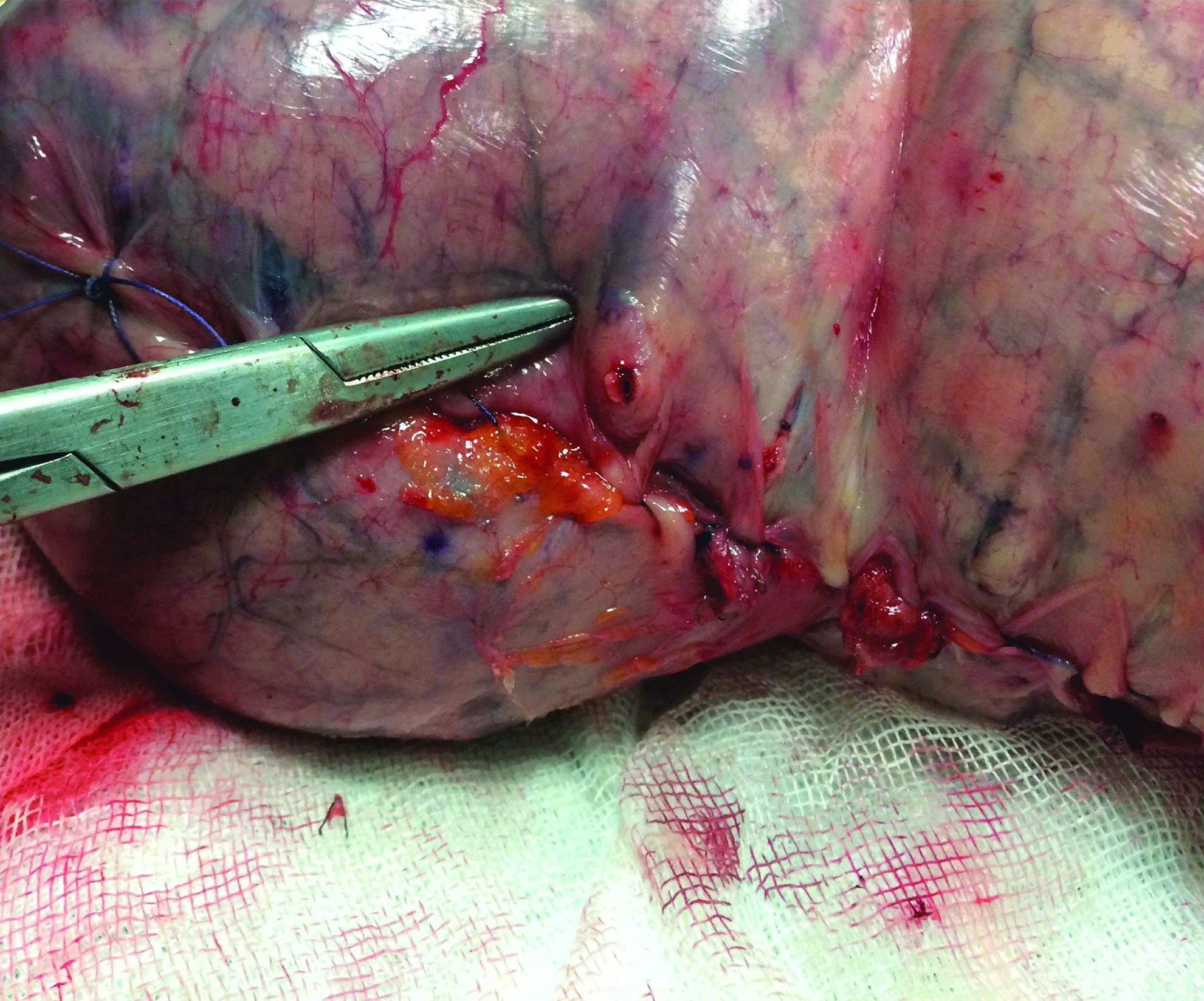
Reinforcement of staple line with knotless suture, after application of pressure.
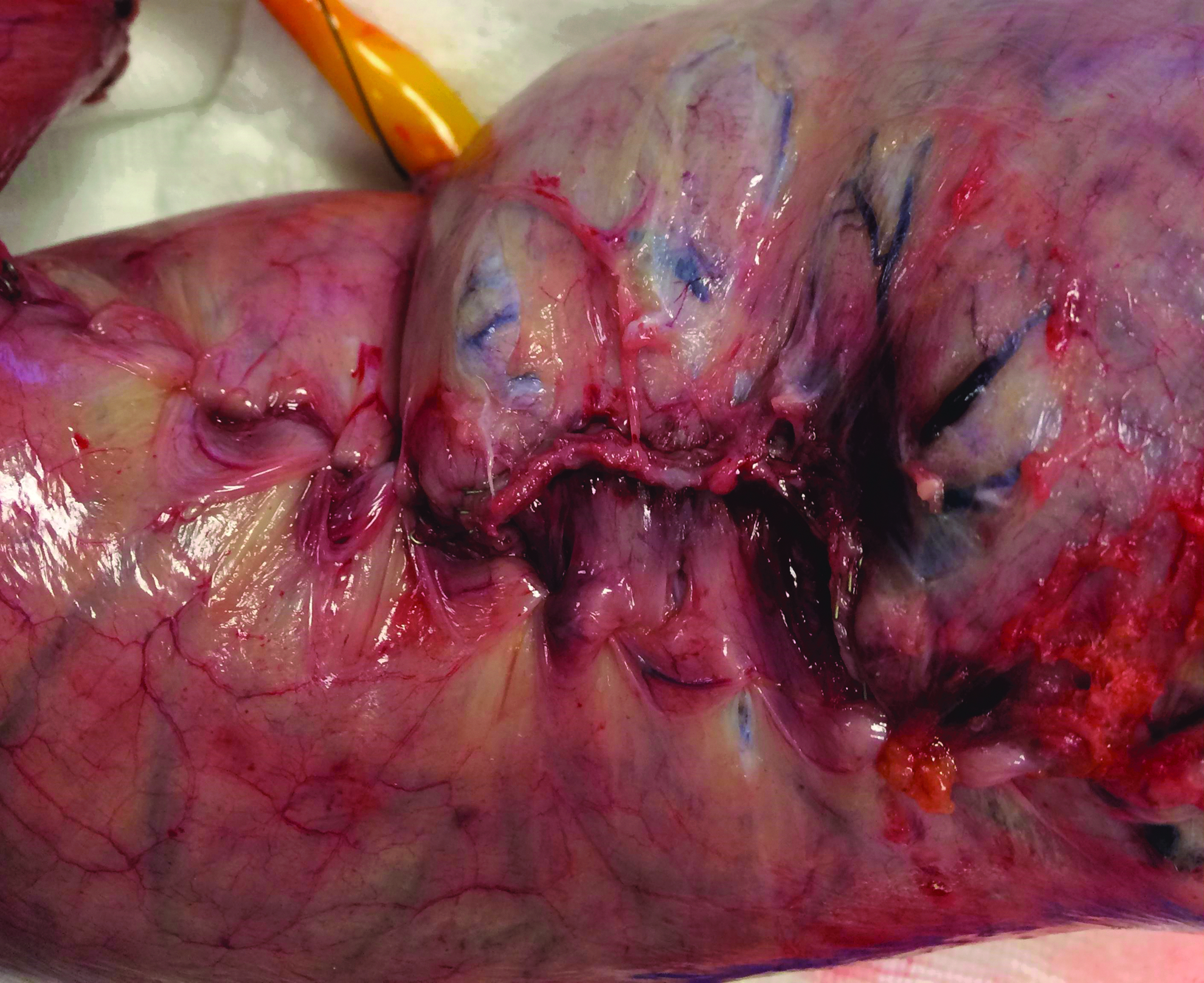
Reinforcement of staple line with knotted sutures, after application of pressure.
Statistical analysis was carried out with SPSS 22 software. Comparison of sex and leakage site across the groups was made using chi-square test. Evaluations between control, normal suture, and knotted suture groups, and normality assessment were examined through visual and analytic methods. For normally distributed data, one-way ANOVA was used to compare variables between groups. Homogeneity of variances was evaluated with Levene test. In case there was a significant difference between groups, paired post hoc comparisons were made using Tukey test. For non-normally distributed data, Kruskal–Wallis test was used for comparison of variables between groups. Paired comparisons were made using Mann–Whitney U test and were evaluated after Bonferroni correction. P level below .05 was accepted as statistically significant.
Results
The study was conducted on gastric tissues of 45 cases that were removed during laparoscopic sleeve gastrectomy operation. Of these cases, 14 (31%) were male and 31 (69%) were female. Mean age was 38.1 (±9.4) years and mean body mass index (BMI) was 45.5 (±6.2) kg/m2. Twenty-five (56%) cases had at least one comorbidity such as diabetes mellitus, hypertension, chronic obstructive pulmonary disease, or sleep apnea. There was no significant difference between the groups regarding age, sex, BMI, and comorbidity state (P = .4, P = .3, P = .4, and P = .5). For no reinforcement suture (sutureless), knotless suture, and knotted suture groups, the average lengths of the removed stomach tissue were 24.0 (±1.0), 26.0 (±0.8), and 23.0 (±0.9) cm, respectively; upper third (fundus) width was 4.9 (±0.2), 4.9 (±0.2), and 4.5 (±0.2) cm, respectively; middle third (corpus) width was 4.5 (±0.2), 4.3 (±0.2), and 4.0 (±0.1) cm, respectively; lower third (antrum) width was 3.5 (±0.2), 3.1 (±0.2), and 3.2 (±0.1) cm, respectively. There was no significant difference between the groups regarding length and width at fundus, corpus, and antrum (P = .06, P = .3, P = .2, P = .4). For sutureless, knotless suture, and knotted suture groups, pressure levels causing leakage were 42.7 (±1), 98.7 (±3.9), and 97.7 (±4.1) mmHg, respectively. There was a statistically significant difference between groups regarding pressure levels (P = .000) (Fig. 4). When the origin of this difference was analyzed with the post hoc Tukey test, it was observed that the difference between sutureless group and other groups continued to exist; however, the difference between knotless suture and knotted suture groups did not reach a statistically significant level. As for the leakage sites, 26 (58%) were in corpus, 14 (31%) were in antrum, and 5 (11%) were in fundus; and there was no difference between the groups regarding leakage site (P = .97).
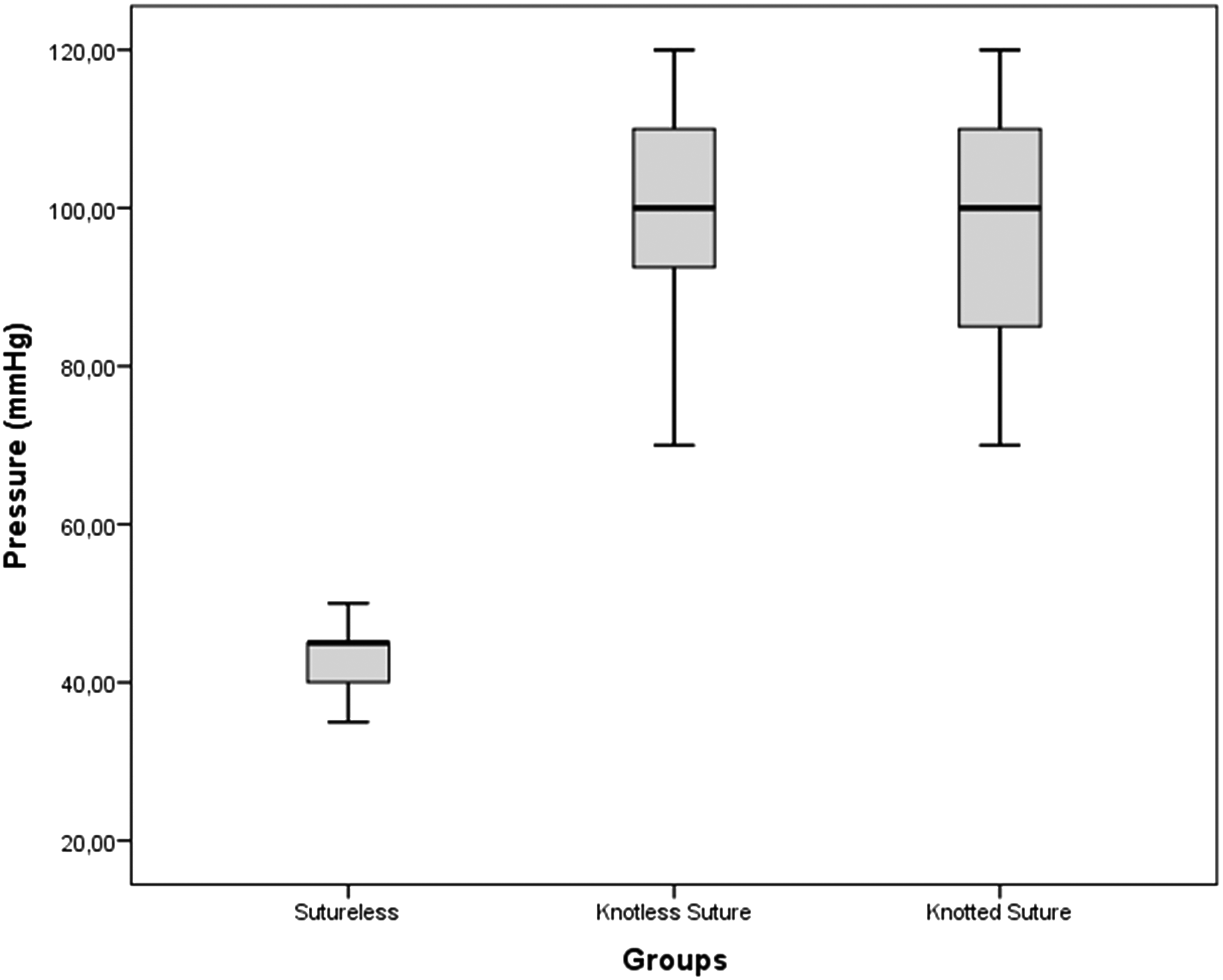
Groups' pressure levels causing leakage.
Discussion
Most frequent complications observed following sleeve gastrectomy operations are bleeding and leakage. Bleeding occurs generally from the staple line or due to insufficient closure of perigastric vascular structures. The etiology of leakage is a bit more complicated, and various reasons were blamed responsible, including thermal injury caused by surgical energy devices, intragastric pressure elevations, and inadequate closure with staples. To prevent the bleeding and leakage complications, various techniques reinforcing the staple line have been used, although their use is somewhat controversial. 8 Suturation of the staple line is among the most commonly used methods for reinforcement of the staple line. In this study, we reinforced staple line by different saturation techniques in resected gastric tissues and, thus, examined the effects of these reinforcement techniques ex vivo.
Reinforcement of staple line with sutures is a widely used technique for avoiding complications like bleeding and leakage. However, there is a controversy on its results. In their meta-analysis, Gagner and Buchwald 9 showed that reinforcement of staple line with sutures decreased leakage rates, whereas in another meta-analysis, Parikh et al. 10 reported that this procedure did not reduce leakage. Results of ex vivo studies are not so much complicated as in in vivo studies. Studies have mostly showed that reinforcement of staple line required a greater pressure for occurrence of leakage. Consistent with the findings in literature, we observed in this study that the pressure level that caused leakage was significantly higher in the groups in which staple line was reinforced with sutures (Group 2 and 3) in comparison to the group no reinforcement was applied (Group 1). As opposed to the in vivo studies, reinforcement of staple line has inarguably favorable results in ex vivo studies, whereas this effect is controversial in in vivo studies.8–10 This suggests a complex dynamics in the etiology of leakage.
As in other surgical applications, knotted sutures are extensively used also in sleeve gastrectomy operations owing to their ease of use, increased wound-holding capacity, and reduced scar formation. 7 In this study, we compared continuous reinforcement procedures performed with two different kinds of sutures (knotless absorbable and knotted absorbable) with the reinforcement-free group. The effect of suture type on leakage pressure has not been studied before. We did not observe difference between the two commonly used suture types, knotless absorbable and knotted absorbable sutures, in terms of leakage pressure. Clinical studies evaluating the effects of reinforcement of staple line on leakage using various suture types may guide surgeons while choosing the sutures that they will use.
Detection of leakage following sleeve gastrectomy is quite difficult. Presence of a long staple line makes it harder to find the leakage site. Related studies have emphasized the difficulty of localization of the site of leakage. However, leaks commonly occur in gastric fundus, and this fact eases the work of surgeons. 3 In this study, 28 of the total gastric tissues had a leak in corpus, 11 had a leak in antrum, and only 6 cases had a leak in fundus region. This may be explained by the dissimilarity between the sizes of resected and left gastric tissues. In addition, complex etiopathogenesis of leakage following sleeve gastrectomy operations may be the origin of the case. It points to the fact that the leakage problem does not occur solely due to mechanical issues, but physiological factors related to circulation and wound healing may also play a role.
One limitation of this study is that this study design was based on mechanical factors, and other physiological factors that play a role in etiopathogenesis of leakage were not investigated. In addition, the examined gastric tissues and left gastric tissues were not exactly the same. Ex vivo studies designed to take all these factors into account can provide significant contributions. The other limitation of this study is that all resected specimens did not have the same shape. Staple lines had straight or zig-zag shape in this study. These zig-zag intersections may be weak compared to other sections. We didn't take into consideration these changes because we used random assignment. However, it would be better if resected specimens were classified according to shapes of the staple line.
Reinforcement of a long gastric staple line, either with knotless or knotted sutures, was shown to increase bursting pressures in our ex vivo model. Further studies to investigate the effect of reinforcement techniques on leaks after laparoscopic sleeve gastrectomy operations are indicated.
Footnotes
Disclosure Statement
No competing financial interests exist.