
Abstract
Abstract
Background:
The identification of retropubic vasculature is not easy under the pressure of insufflated gas during totally extraperitoneal (TEP) inguinal hernioplasty. We aimed to present the usefulness of a maneuver that allows the clear identification of retropubic vasculature.
Methods:
Vascular anatomy on the retropubic surface in 364 patients who underwent the TEP procedure from January 2005 to September 2015 was evaluated. In patients after July 2014, the pressure in the workspace was decreased from 14 to 8 mmHg before fixation of the mesh to clearly identify the veins. The results before and after July 2014 were compared.
Results:
Demographic features were not significantly different between two periods. The number of hemipelvises in the first and second periods was 398 and 77, respectively. The rate of identification of venous corona mortis was 31% in the second period, whereas it was 1.0% in the first period (P = .000). The identification of thick (5.5% versus 10.3%; P = .123) and thin (22.8% versus 36.3%; P = .014) arterial structures and their sum were increased in the second period (28.4% versus 46.7%; P = .002). The rate of retropubic bleeding was zero in the second period, while it was 1.5% in the first period.
Conclusions:
During TEP hernioplasty, the pressure of insufflated gas more than 10 mmHg in the preperitoneal space hinders the correct identification of vessels on the retropubic surface. The proposed maneuver, to decrease the pressure in the workspace to 8 mmHg, can provide clear identification of all vessels, which decreases the potential risk of vascular injury.
Introduction
A
Currently, laparoscopic approaches, transabdominal preperitoneal repair, or totally extraperitoneal (TEP) for inguinal hernia repair have been widely accepted as first line surgical treatment for all groin hernias, inguinal or femoral, unilateral or bilateral, primary or recurrent. 9 Therefore, the retropubic vascular anatomy should be well known by surgeons working in the field of hernia surgery.
The risk of laceration of venous structures during dissection or fixation of synthetic mesh on Cooper's ligament with titanium tacks is more subtle compared with an arterial injury, due to the sealing effect of the pressure of insufflated carbon dioxide in the preperitoneal space. Therefore, a venous injury can be evident in the early postoperative period as a huge hematoma in the pelvic region.6,10
Generally, during the TEP procedure, the preperitoneal space is inflated by 12–14 mmHg of warmed carbon dioxide.11,12 Likewise, we had been performing TEP procedures under pressure of 14 mmHg up to July 2014. In that period, venous structures were not prominent to get our attention during dissection. Our case series, including that period, the rate of identification of prominent venous structures was 1%. 13 The venous pressure in the pubic area in a patient at rest in the supine position is nearly 10 mmHg. 14 Therefore, pressure exceeding this level would collapse the venous structures.
Based on these data, Dr. Ates first identified that the retropubic venous structures had been invisible under the pressure of 14 mmHg; therefore, to decrease the pressure to 8 mmHg before the fixation of synthetic mesh on Cooper's ligament by titatinum tacks could be useful for the clear identification of venous structures clearly. In this study, we aimed to present the effect of this maneuver proposed for the identification of retropubic vascular structures under the pressure of 8 mmHg in patients who underwent TEP hernia repair.
Materials and Methods
Patients who underwent TEP hernia repair from January 2005 to September 2015 in the Malatya State Hospital Department of General Surgery and the Inonu University Faculty of Medicine were included. All of the operations have been performed by two surgeons, M.A and A.D. Vascular anatomy of the retropubic area has been specifically explored in each patient. Data were collected prospectively and the study was prepared retrospectively. A written consent for surgical intervention was obtained from each patient.
Definition of CMOR and vasculature of retropubic area
Any aberrant obturator vessel originated from an inferior epigastric artery/vein, then crossed the superior pubic ramus and moved toward the obturator foramen, here forming an anastomosis with branches of the ordinary obturator artery/vein was defined as CMOR, in this study (Fig. 1A). In addition, aberrant obturator vessels following the same path without formation of an anastomosis were also included in the definition of CMOR (Fig. 1B). Furthermore, although it was not included in the definition of CMOR, a pubic branch of the inferior epigastric artery running parallel to the superior border of the pubic ramus toward the symphysis pubis and here separating to its terminal branches was also considered.

Schematic illustrations of corona mortis.
The origin, thickness, and presence of pulsation were noted to identify the nature of vascular structures. To estimate the thickness of anastomosing artery, the tip of an endodissector (EndoDissect®, Covidien) 2 mm in diameter was used. The vessels were considered as thick (≥2 mm) or thin (<2 mm) according to this measurement. Vascular injuries were also enrolled.
Grouping and technical details of the proposed maneuver
The operations were carried out in the standard manner previously described elsewhere. 13 All of the operations were performed by the same surgical team. The study period was divided into two segments: the first from the beginning to July 2014 and the second from August 2014 to the end of study.
During the first period, the preperitoneal space was filled with warmed CO2 at the level of 14 mmHg to provide a workspace, and this pressure was maintained during the entire TEP procedure. During the second period, the pressure in the preperitoneal area was decreased to 8 mmHg just before the fixation of the mesh for 20–30 seconds. After identification of the vascular structures under this low pressure, it was increased to 14 mmHg again to provide the safe manipulations during the placement and fixation of the mesh. Two examples of the improved identification of venous CMOR under the pressure of 8 mmHg are shown in Figures 2 and 3. An example is also shown in Supplementary video (Supplementary Data are available online at www.liebertpub.com/lap).
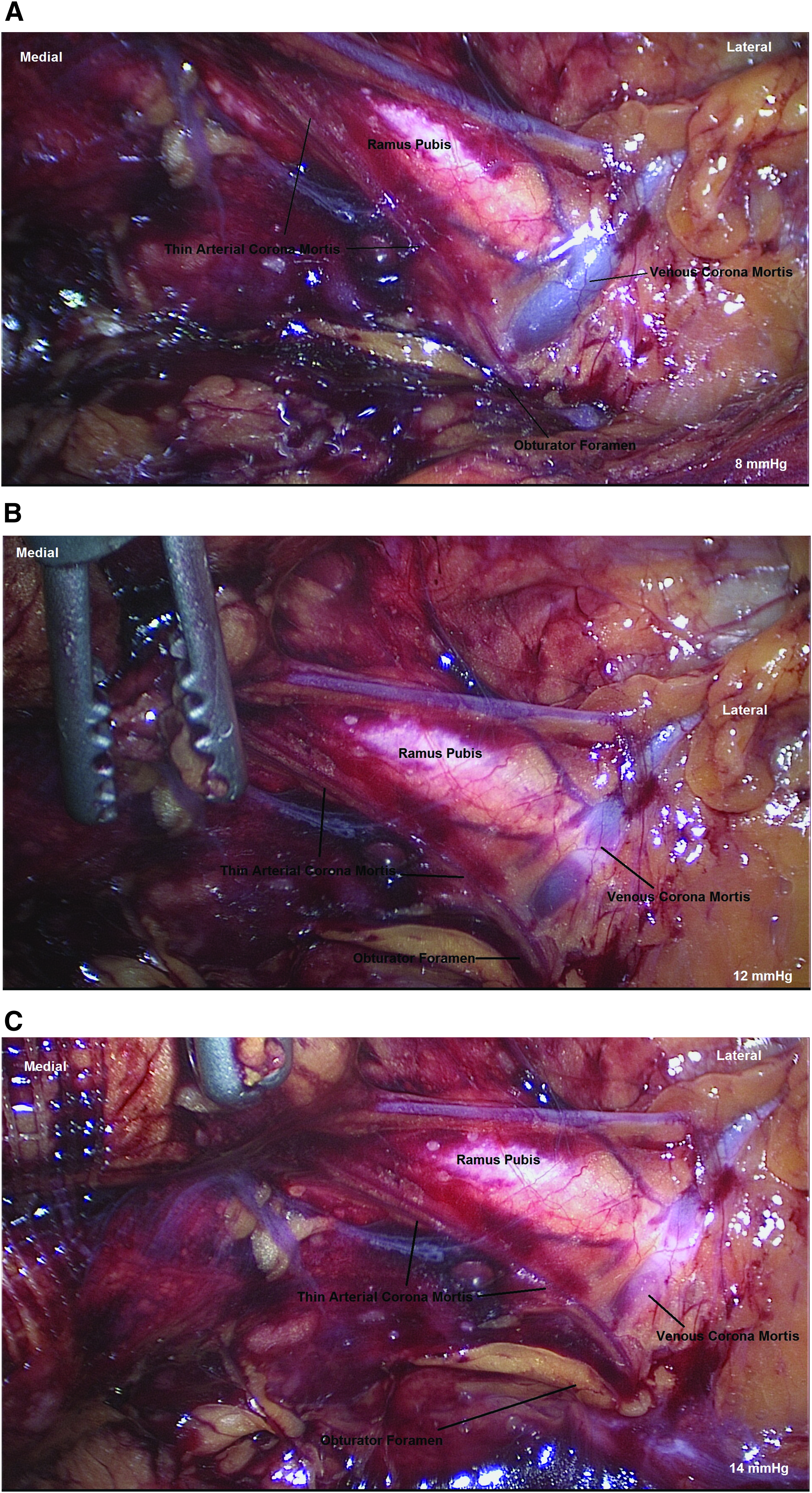
Retropubic view of right inguinal area.
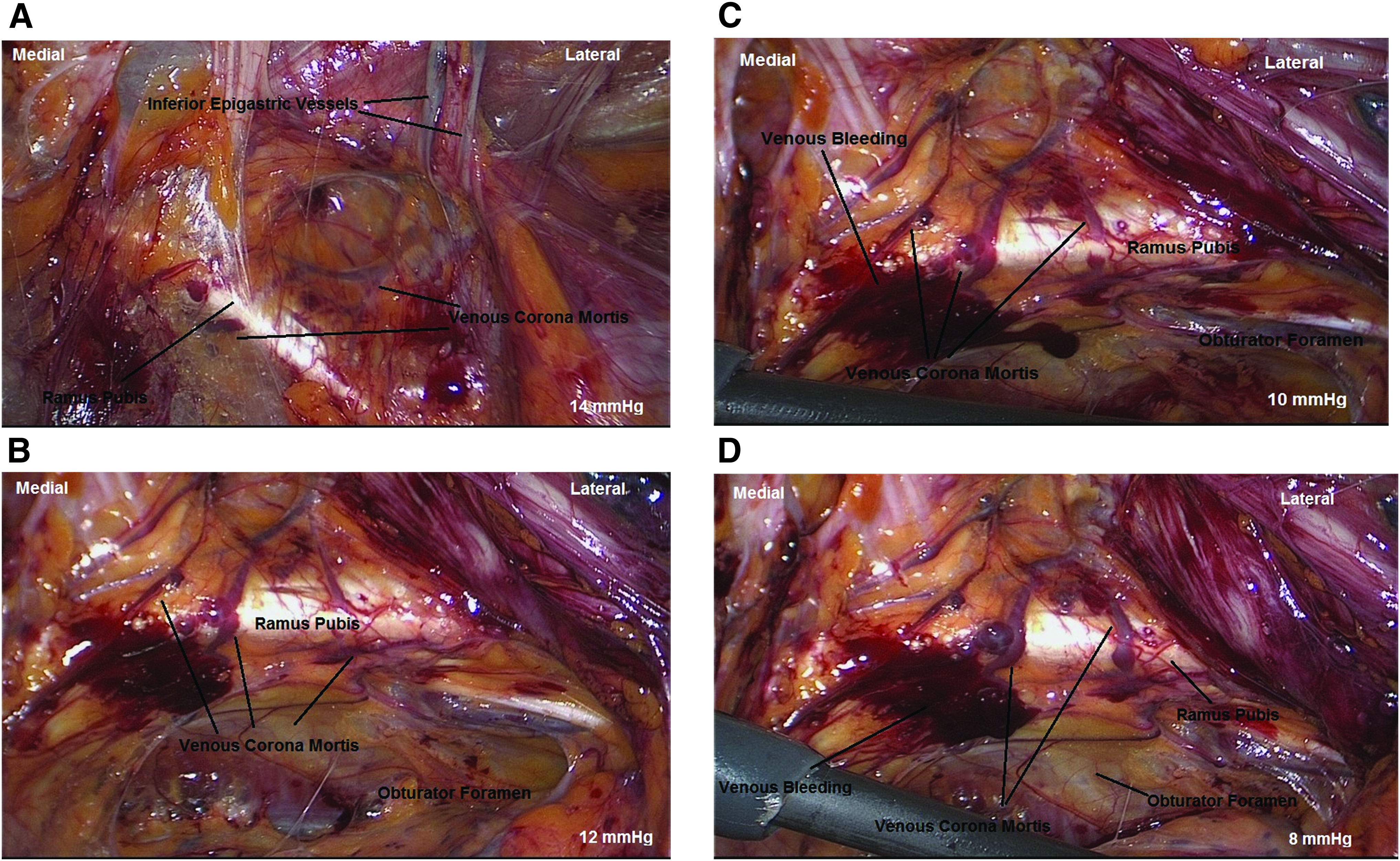
Retropubic view of right inguinal area in another patient.
To identify all vascular structures, the retropubic area was inspected carefully in all of the patients, and the vascular structures were noted at the end of each operation. Very thin venous structures on the retropubic area and Cooper's ligament were ignored. Basic demographic parameters, including age and gender, presence and type of retropubic vascular structures, and intraoperative and early postoperative bleeding from retropubic area, were compared between groups.
Statistical analysis
The SPSS 20.0 (SPSS, Inc.; IBM Corporation, Armonk, NY) software was used for statistical analysis. Normally distributed continuous variables were expressed as mean (± standard deviation) and compared using a t-test. Nominal data were expressed as case numbers and percentages and were compared using Fisher's exact test. All tests were two sided. A value of P < .05 was accepted as statistically significant.
Results
From January 2015 to September 2015, 475 hemipelvises in 364 patients who underwent the TEP procedure were considered. The general features of the study population are detailed in Table 1.
Although the primary target of this maneuver was to identify the venous structures clearly, the identification of thin (22.8% versus 36.3%; 0.014) arterial CMOR was significantly increased in the second period. In addition, the rate of identification of thick arterial CMOR was also incresed in the second period; however, the difference was not statistically significant (5.5% versus 10.3%; P = .123). Furthermore, the rate of identification of all arterial structures was also significantly improved in the second period (28.4% versus 46.7%; P = .002 for all arterial CMOR and 45% versus 68.8%; P = .000 for all arterial structure, including the pubic branch of the inferior epigastric artery).
Venous CMOR were not properly identified in the great majority of the cases in the first period. A prominent venous CMOR was identified in only four cases (1.0%). However, veins on retropubic surface were identified more easily during the second period (31.2%) (P = .000).
The comparison of the results of two periods is detailed in Table 2. Intraoperative bleeding due to injury of thin (<2 mm) arterial CMOR during stapling of tacks was seen in six hemipelvises of six patients in the first period. After the stapling of the tacks, it was not possible to control the bleeding even with simple laparoscopic methods while a relatively huge prosthetic mesh covered the vision. Therefore, we convert to open surgery, simple tamponade with a gauze for 10 minutes was successful in two cases, and bipolar cauterization was used in the remaining four cases. Although intraoperative bleeding from retropubic area was not significantly different between the two periods, it was not seen in the second period. In patients with intraoperative bleeding from the retropubic area, we were obliged to convert to open surgery to provide hemostasis.
Bold values: P < 0.05 is statistically significant.
Discussion
The definiton of CMOR remains controversial in the literature.3,5,6,12 While Darmanis et al. 5 only accepted the aberrant obturator vessels forming anastomosis around the obturator foramen as CMOR, Lau and Lee 6 and Rusu et al., 3 like us, define CMOR as any vessel coursing over the superior pubic ramus with or without formation of anastomosis. Berberoğlu et al. 1 define the CMOR as “the communicating vein” between the external iliac and obturator veins over the superior pubic ramus. We thought that the term Corona Mortis, as the name suggests, defines the trap on the retropubic area for surgeons, because it is not a standard anatomical structure.1–6,13 Therefore, we adopted all of the aberrant obturator vessels as CMOR, whether it forms an anastomosis or not.
Postoperative retroperitoneal hematoma due to the injury of an arterial CMOR after TEP hernia repair was previously reported. 7 In addition, the injury of aberrant obturator vessels can occur during open inguinal or femoral hernia repair. 10 Therefore, sufficient exposure to the retropubic area is crucial especially during laparoscopic approaches.
The identification of vascular structures on the retropubic surface before fixation of a mesh to Cooper's ligament has great importance to prevent a vascular injury. However, some challenges face surgeons in the exploration of retropubic area. Lau and Lee 6 concluded that, on the retropubic area, arterial injury can be easily recognized during the TEP procedure; however, venous injury can be masked by the sealing effect of the pressure of insufflated carbon dioxide, which would be presented as postoperative hemorrhage. Indeed, we also saw the confusing effect of produced pressure in preperitoneal space on the identification of vessels on superior pubic ramus or Cooper's ligament in our case series.
TEP hernia repair is generally performed under the pressure of 12 mmHg of warmed carbon dioxide. 11 In our operations, we have preferred to work under 14 mmHg during TEP procedure to provide sufficient exposure and comfortable manipulations. These levels of pressure exceed the normal superficial venous pressure of a patient in the supine position at rest, which is approximately 10 mmHg on the pelvic region. 14 This is the simple mechanism of the sealing effect on veins that hinders the correct identification of these vessels.
At the end of first period of our case series, we became aware of this problem. To solve it, we have been decreasing the pressure in the preperitoneal space to 8 mmHg just before the fixation of the mesh to identify vascular structures on the retropubic surface. After the identification of vessels, the pressure was returned to the level of 14 mmHg to provide safe and comfortable manipulations. According to the results of the comparison of our two periods, it is clear that this maneuver provides correct identification of venous CMOR (P = .000). In addition to venous structures, the identification of thin arterioles below 2 mm was also increased significantly in the second period (P = .014).
According to the previous knowledge about peripheral venous pressure, 14 venous structures could be evident under any pressure below 10 mmHg in the pelvic region. However, we proposed the pressure of 8 mmHg, which is the lower limit for safe visualization in preperitoneal space according to our experience, and inspection under 8 mmHg provides a more prominent view to veins and also to very thin arterioles.
An interesting result of the current study was the increase in the identification of larger (>2 mm) arterial structures. Although the difference was not statistically significant (P = .123), the identification rate of these larger arteries increased almost twofold in the second period (5.5% versus 10.3%). In our case series, arteries were identified by the inspection of the pulsation. Although we referred to “large arteries,” this term alluded a relatively larger size. Actually, arterial structures on the retropubic surface were not really “large” in size; therefore, the identification of relatively larger arteries was also not easy. After the proposed maneuver, 4–6 mmHg of decrease in pressure was provided that made it possible to see more prominent pulsation of these arteries. We believe that the increase in the identification of larger arteries was dependent upon this. This is another benefit of the proposed maneuver.
When we evaluated the clinical results of these corrections in identification of the vessels, there was no statistically significant difference between the two periods (P = .595) regarding intraoperative bleeding complication. This can be due to the relatively small number of cases in the second period. However, intraoperative retropubic bleeding was not seen in the second period against six cases (1.5%) of bleeding from thin arterioles in the first period that obliged us to convert to open surgery. Therefore, we believe that this difference could be statistically insignificant, but it was clinically significant.
In the first period of our cases, the incidence of arterial CMOR and total number of arterial structures, including pubic branch of the inferior epigastric artery, were 22.8% and 45.0%, respectively. However, in the second period, incidence of arterial CMOR, total number of arterial structures, and venous CMOR were 46.7%, 68.8%, and 31.2%, respectively. As anatomical data, the proposed maneuver provided more reliable in vivo results. However, there has been great variation about the incidence of arterial or venous CMOR.
In the studies performed on cadavers, the ranges for arterial and venous CMOR were 15%–69% and 20%–70%, respectively.2–5,15–19 Berberoğlu et al. 1 revealed the presence of venous communication between external iliac and obturator veins in 34 of 36 laparoscopic pelvic dissections. However, they did not report the level of pressure in their workspace. In another study, including living patients who underwent the TEP procedure, Lau and Lee 6 reported the incidence of arterial CMOR as 22% and venous CMOR as 27%, which were more than our results in the first period and slightly less than in the second period. We thought that the differences in incidences were related to the lower level of pressure in the workspace during the identification of vessels, which were 14 mmHg in our first period, 8 mmHg in our second period, and 10 mmHg in the study of Lau and Lee. 6
Although the mentioned results were generally optimistic, some confusing points should be explained. The number of cases regarding the bleeding complication only included bleeding that existed just before the fixation of the mesh. Hence self-limiting and insignificant hemorrhages occurring during dissection like those shown in Figure 3 were excluded in this study. Low pressure (below 10 mmHg) in workspace is necessary to provide an excellent vascular identification during entire dissection. However, it seems to be impossible to safely work under the pressure lower than 10 mmHg during entire dissection. Therefore, we proposed to decrease the pressure of the workspace just before the fixation of the mesh for a limited time to prevent vascular injuries by tacks. Nevertheless, it should be kept in mind that too aggressive blunt dissection along the pubis can have the similar risk with the fixation of the mesh for vascular injury on retropubic surface.
The main limitation of this study is its retrospective nature, despite the collection of the data prospectively by the same surgical team. In this study, we would like to honestly admit that, as our experience and attention to retropubic vasculature increases, an increase in the identification of retropubic vessels could be possible. However, the differences between the groups were very high in some specific parameters that could exclude this reducing effect in reliability. In addition, although the quantitative results were sufficient to perform statistical analyses, there were relatively fewer patients in the second period. The final limitation relates to the methodology, as the diameters of arterial structures were measured by a relatively subjective method.
In conclusion, the pressure of insufflated carbon dioxide more than 10 mmHg in the preperitoneal space during TEP hernia repair hinders the correct identification of vessels on the retropubic surface, which is critical especially during the fixation of mesh by tacking on to Cooper's ligament. The proposed maneuver, to decrease the pressure in the workspace to 8 mmHg just before the fixation of mesh, can provide more reliable identification of the vessels, especially veins and very thin arteries, which prevents the potential risk of vascular injury.
Footnotes
Acknowledgment
The abstract has been presented as an oral presentation in fifth Congress of Turkish National Hernia Surgery, October 22nd–25th, 2015, Mugla, Turkey.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.