
Abstract
Abstract
Background:
We evaluated the feasibility of a three-port totally laparoscopic distal gastrectomy (TLDG) as a reduced port laparoscopic surgery for the treatment of early gastric cancer (EGC).
Materials and Methods:
In total, 110 patients who underwent three-port TLDG (n = 25) and four-port TLDG (n = 85) were enrolled. A propensity score matching analysis was used to compensate for the differences between the groups in age, gender, body mass index, Eastern Cooperative Oncology Group classification, and comorbidity. After the matching, operative details, pathological features, and short-term postoperative outcomes were compared between groups.
Results:
By propensity score matching, 25 matched pairs were created, and no characteristic difference was observed between the groups. Operating time was significantly shorter in the three-port TLDG group than in the four-port TLDG group (139.4 ± 39.4 minutes versus 184.8 ± 42.1 minutes, respectively; P < .001). Duration until discharge was significantly shorter in the three-port TLDG group than in the four-port TLDG group (8.2 ± 5.6 days versus 10.2 ± 6.6 days, respectively; P < .046). Regarding pathological features, including TNM stage, no significant difference was observed between the groups.
Conclusions:
The three-port TLDG is a practical method as a reduced port surgery and has better short-term outcomes than the four-port TLDG for the treatment of EGC.
Introduction
R
Surgical treatment for gastric cancer has also focused on MIS.6,7 The first surgical treatment using laparoscopy for gastric cancer was performed as a laparoscopy-assisted technique with a minilaparotomy. 8 However, after the first totally laparoscopic distal gastrectomy (TLDG), using a linear stapler for a patient with a benign gastric ulcer in 1992, a totally laparoscopic approach was applied to gastric cancer and is now used commonly in the treatment of early gastric cancer (EGC).9–11 This totally laparoscopic approach can reduce scarring dramatically, with the exception of the minilaparotomy, and many other techniques to reduce scars have been tried in the laparoscopic treatment of gastric cancers. 12
In fact, although the goal of MIS might be single-incision laparoscopic surgery or natural orifice translumenal endoscopic surgery, these techniques have several limitations because of conflicts between instruments and limited visual fields.13–16 Thus, it may be considered that the minimum number of ports needed for a safe and comfortable operation is three: two for the operator and the other for the camera. Reduced port laparoscopic gastric cancer surgery using four ports has occasionally been reported.6,17 However, there have been few studies of three-port laparoscopic gastrectomies in the treatment of gastric cancer. Thus, a three-port TLDG, which would be a desirable MIS technique in gastric cancer, was compared with a four-port TLDG in this study.
Materials and Methods
Patients and data collection
Of all patients with clinically EGC, 110 who underwent TLDG at the Uijeongbu St. Mary's Hospital between 2012 and 2015 were enrolled in the present study. All operations were performed by a single gastric cancer specialist (author LHH). Of the 110 patients, 85 underwent a four-port TLDG and 25 underwent a three-port TLDG.
Demographic, clinical, and pathological characteristics, operative details, and short-term postoperative outcomes—collected retrospectively from the hospital's Gastric Cancer Patient Registry—were compared between groups. Perioperative clinical characteristics were classified according to the Eastern Cooperative Oncology Group (ECOG) classification. 18 Pathological stage was classified according to the Seventh American Joint Cancer Committee (AJCC) TNM. Histological cancer type was categorized as differentiated or undifferentiated. Poorly differentiated tubular adenocarcinoma, signet ring cell adenocarcinoma, and mucinous adenocarcinoma were assigned to the undifferentiated group.
This study was approved by the Institutional Review Board of the Ethics Committee of the College of Medicine, The Catholic University of Korea (UC15RISI0106). Patient records were anonymized and deidentified before analysis.
Surgical procedures
The three-port TLDG was performed through a 12-mm port located in the umbilical area, mainly for camera work, a 12-mm port located in the right lower quadrant (RLQ) area, and a 5-mm port located in the right upper quadrant area. The four-port TLDG was performed using the same locations as the three-port TLDG, with an additional 5-mm port in the left lower quadrant (LLQ) area (Fig. 1). During the four-port TLDG, the first assistant or scopist used the port in the LLQ area. Conventional laparoscopic instruments, including a rigid laparoscope, were used in each operation.
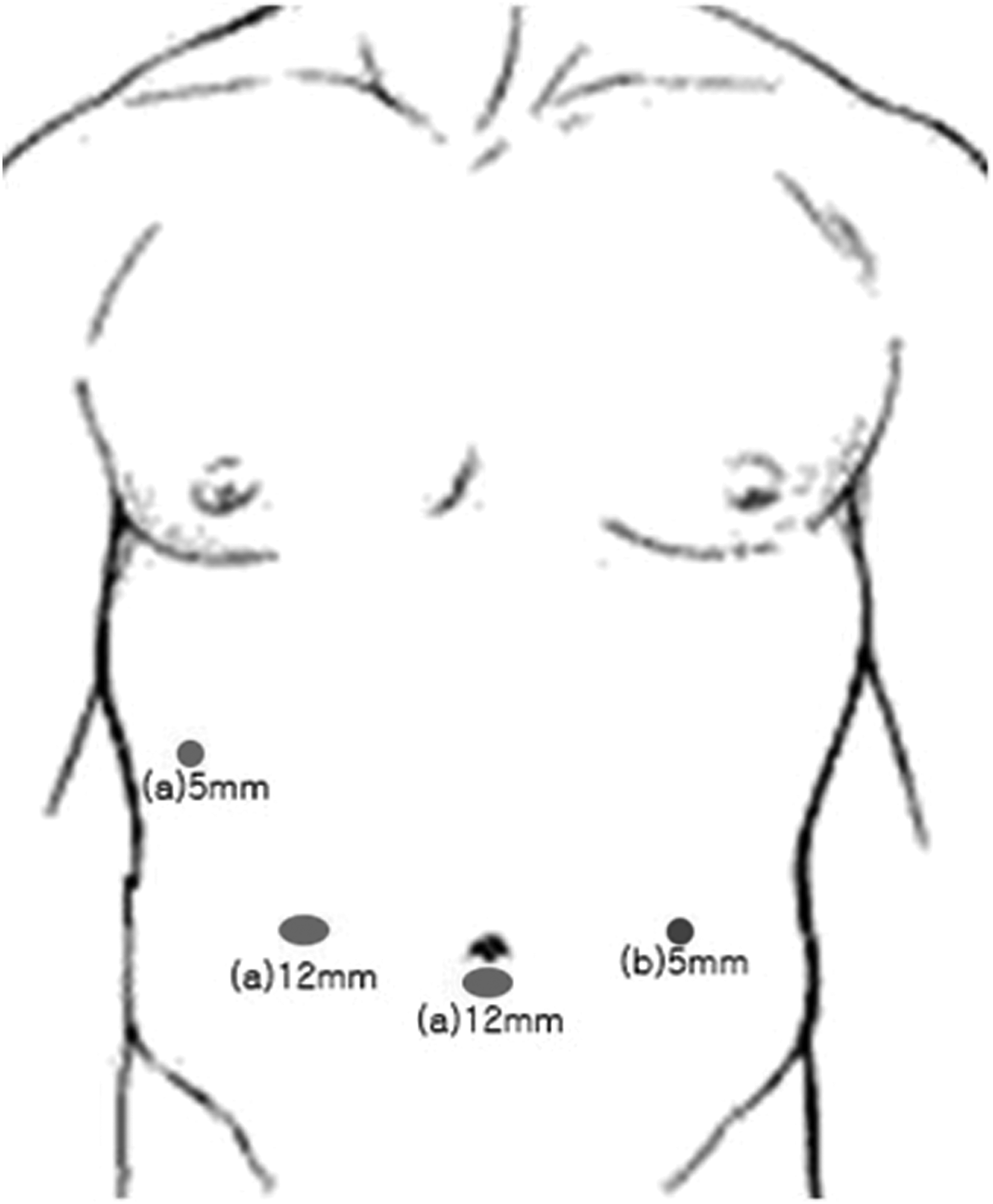
Port location of each technique.
Reconstruction was performed by intracorporeal anastomosis with a linear stapler. The linear stapler was used through the RLQ or the umbilical 12-mm port for anastomosis. The umbilical port site was extended vertically by 2.5–3 cm, and a specimen was extracted via the extended umbilical site.
Propensity score matching and statistical analyses
Propensity score matching was conducted to adjust for differences between the groups in patient characteristics that are directly related to short-term outcomes. Propensity scores were obtained using binary logistic regression with covariates of age, gender, body mass index (BMI), ECOG classification, and comorbidity. Subsequently, the three-port TLDG group was 1:1 matched to the four-port TLDG group based on the top 25 propensity scores.
The χ2 test or Fisher's exact test was used to compare categorical variables between groups. Student's t-test and the Mann–Whitney U-test were used to compare continuous variables before and after propensity score matching, respectively. Statistical analyses were performed with the SPSS for Windows software (version 13.0; SPSS, Inc., Chicago, IL). Values of P < .05 were considered to indicate statistical significance.
Results
Patient characteristics are shown in Table 1. First, the characteristics of the 25 patients who underwent the three-port TLDG and the 85 patients who underwent the four-port TLDG were compared. The mean BMI was significantly lower in the three-port TLDG group than in the four-port TLDG group (22.4 ± 2.6 kg/m2 versus 24.7 ± 3.8 kg/m2, respectively; P = .006). Additionally, although not statistically significant, the four-port TLDG group included one patient whose ECOG performance status was three. After the propensity score matching, 25 well-matched pairs were created. The mean BMI then showed no significant difference between groups (22.4 ± 2.6 kg/m2 versus 22.1 ± 3.0 kg/m2, respectively; P = .634). There was no patient whose ECOG performance status was three in either group. Among the other preoperative factors, such as age, gender, and comorbidity, which influence the operation and postoperative course, none showed a significant difference between the groups (Table 1).
BMI, body mass index; ECOG, Eastern Cooperative Oncology Group; SD, standard deviation.
There was no significant difference between the groups with regard to the reconstruction method, extent of lymph node dissection, or combined operation. However, operating time was significantly shorter in the three-port TLDG group than in the four-port TLDG group (140.2 ± 41.1 minutes versus 182.2 ± 48.1 minutes, respectively; P < .001). Estimated blood loss was almost equal between groups (Table 2). With respect to pathological features, including TNM stage, no significant differences were observed between the groups (Table 3).
AJCC, American Joint Cancer Committee.
While there were no significant differences in postoperative course, including the mean duration to flatus and soft diet between two groups, the three-port group had a significantly shorter mean duration of discharge than the four-port group (8.2 ± 5.6 days versus 10.2 ± 6.6 days, respectively; P = .046). Morbidity in the three-port group was somewhat lower than that of the four-port group, but the difference was not statistically significant. No death was reported in either group (Table 4).
Within 30 postoperative days.
Discussion
Reduced port surgery (RPS) simply means a laparoscopic surgery that is performed with fewer ports than in conventional laparoscopic surgery in that field. RPS has several benefits, such as improved cosmetic outcomes, decreased pain, and reduced analgesic requirements due to the reduced scarring; thus, there is a trend toward RPS being used more widely within laparoscopic surgery.12,19,20 However, the reduction in assistance associated with fewer ports requires higher surgical skill of the operator and/or the use of special instruments, such as flexible scopes, curved graspers, and specialized needles.13,15,16 RPS depends mainly on surgeons' abilities to overcome the loss of assistance associated with fewer ports and the insufficient development of specialized instruments for RPS.
The present standard treatment for EGC is five-port laparoscopic surgery. Although the method can be changed according to the preference of the operator, the ports are usually used as follows: one umbilical port for a camera, two right side ports for the operator, and two left side ports for the assistant. In cases of extracorporeal anastomosis, a new minilaparotomy, or a laparotomy that is extended from one of the five port sites, is used to anastomose and eliminate specimens. 10 Recently, a four-port laparoscopic gastrectomy has been performed commonly as a comfortable RPS. 17 Thus, the present study compared a three-port TLDG with a four-port TLDG to assess whether a three-port TLDG is a satisfactory RPS for EGC.
Before the propensity score matching, several differences were seen between the groups. First, the number of patients in each group was quite different. Second, the ECOG classification was different between the groups, although not significantly; one patient in the four-port TLDG group belonged to the third grade of ECOG. Finally, and most importantly, the mean BMI was significantly lower in the three-port group than in the four-port group. BMI has been considered as a crucial factor with respect to the difficulty of surgery, especially with a laparoscopic approach. Higher BMI can cause a longer operation time, more intraoperative blood loss, and a higher rate of postoperative complications after laparoscopic gastrectomy because such patients tend to have excessive intra-abdominal fat and a thick abdominal wall such that the operator's dexterity is diminished.21–23 Thus, our initial data were not appropriate to compare the groups fairly and accurately. Therefore, we used propensity score matching to compensate for such selection biases. As a result, 25 well-matched pairs were created, and there were no significant differences in preoperative characteristics between the groups.
In laparoscopic surgery, making a countertraction is necessary for a good visual field. The first assistant usually conducts the counter-retraction to press tissues or pull adjacent organs through one or two ports. However, a counter-retraction can also be made using special instruments, such as articulated forceps and specialized sutures, and consequently, the ports can be reduced.24,25 Moreover, an operator who is an expert surgeon can reduce ports even without using special instruments. 12 First, gravity can be used. According to changes in the patient's position, such as Trendelenburg, reverse Trendelenburg, tilting right, and tilting left, a counter-retraction can be achieved by the weight of the organs. In fact, most operators do use position changes in open surgery and laparoscopic surgery to ensure a good visual field. Second, a physiological attachment can be used. There are many physiological attachments around the stomach, such as the gastrocolic and hepatoduodenal ligaments; they can play a role as anchors for tissue traction, and the need for assistants' hands can be reduced. Third, appropriate use of the right hand of the operator, such as for dissecting with pressing or pulling, can help the operator to perform two or three actions at once. Such methods can be used to achieve countertraction without special instruments if applied appropriately. Thus, a three-port TLDG should be an option for an expert surgeon with or without special instruments.
The present study showed that the operating time was significantly shorter in the three-port TLDG group. The reduced operating time was due to several reasons. First, unnecessary actions, which might be caused by the first assistant, were decreased according to the reduced number of instruments required. Moreover, the visual field through the laparoscopic camera focused on the instruments of the operator only, which can prevent unpredictable injuries that develop from blind areas. Subsequently, the time to wrap up the operation, with respect, for example, to remnant bleeding control and operation field inspection, could be shortened. Additionally, the opening and closing time of port sites—even though they are only a few minutes in duration—could be reduced. The time for discharge in the three-port TLDG group was significantly shorter than that of the four-port TLDG group. Such a result might be caused by the relatively higher morbidity in the four-port TLDG group, although the difference was not statistically significant.
The present study had several limitations. First, the data were collected retrospectively. Second, the four-port TLDG was generally performed earlier than the three-port TLDG, and the surgical quality associated with port reduction might have improved with the passage of time. However, before performing the RPS, the operator was already an experienced laparoscopic gastric cancer surgeon, and the reduced operating time was not associated with a learning curve. From another perspective, the results demonstrated that three-port TLDG could be a useful method for skillful surgeons. In addition, propensity score matching was used to overcome the inevitable selection bias.
In conclusion, a three-port TLDG showed improved short-term outcomes, such as operating time and time for discharge. These results indicate that three-port TLDG, which could be considered a neo-RPS for EGC, has operative feasibility compared with a four-port TLDG. Long-term outcomes of three-port TLDG, including survival, need to be determined. Three-port TLDG appears to be a safe and practical reduced port surgical method for the treatment of EGC.
Footnotes
Acknowledgment
This study was supported by grants from the National Research Foundation of Korea (nos. 2012R1A1A1043576 and 2015R1A1A1A05028000).
Disclosure Statement
No competing financial interests exist.