
Abstract
Abstract
Background:
It is commonly believed that eating habits, specially the sweet eating habit, can predict results after bariatric surgery; for this reason, it is considered one of the selection criteria when deciding the surgical technique. However, there is not enough evidence of its impact on the results after sleeve gastrectomy (SG).
Objective:
To evaluate the relationship between the sweet eating habit and weight loss after SG.
Design:
Cross-sectional retrospective study.
Material and Methods:
Group A: nonobese subjects, and group B: patients who underwent SG and had ≥6 months follow-up. Demographics, anthropometrics, percentage excess weight loss (%EWL) at 6, 12, and 24 months, and eating habits before surgery were analyzed. Sweet eating consumption was classified as follows: mild, moderate, and severe. Uni- and bivariate logistic regression analysis according to each variable was performed.
Results:
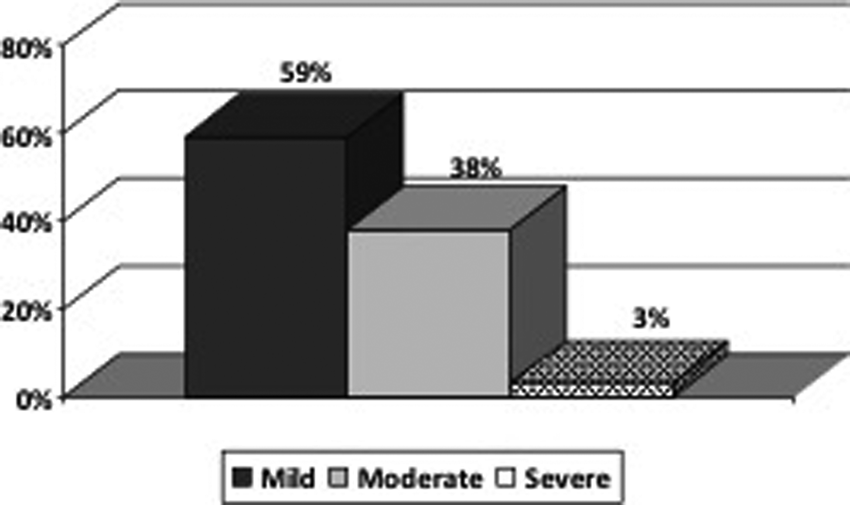
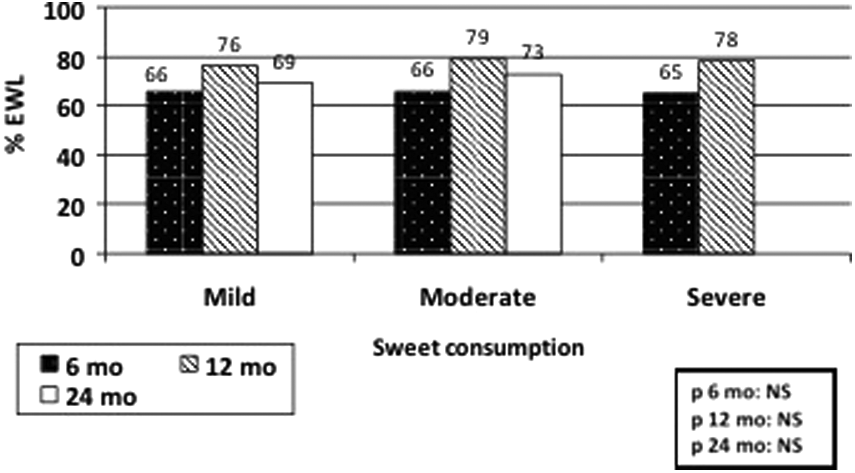
Between 2006 and 2011, 157 patients underwent SG at our institution; 36% were male, age 41 years old, and initial body mass index 46 kg/m2. Mean %EWL at 6, 12, and 24 months was 66%, 77%, and 70%, respectively. Sweet eating consumption: Mild: 59%; Moderate: 38%; and Severe: 3%. No difference was found in sweet eating patterns among groups A and B; %EWL for mild, moderate, and severe sweet eaters at 6 months was 66 ± 16, 66 ± 14, and 65 ± 10, respectively (P = non-significant [NS]). The same analysis was made at 12 months: 76 ± 20, 79 ± 18, and 78 ± 11 (P = NS). At 24 months, only mild and moderate sweet eaters were available for comparison: 69 ± 23 and 73 ± 19, respectively (P = NS).
Conclusion:
Preliminary data suggested that preoperative sweet eating habit would not predict results after SG in terms of weight loss.
Introduction
O
Bariatric surgery represents the most effective tool to accomplish long-term weight loss and resolution or improvement of comorbidities in morbidly obese patients.3,4 The majority of patients who undergo bariatric surgery will achieve favorable results, but still, 15%–20% of them will not attain the expected outcome. 5 Failure after bariatric surgery is multifactorial, and it is related mostly to patient's characteristics, technical reasons, and follow-up quality, among others.
For this reason, detection of factors that can affect the results after bariatric surgery becomes essential. Among predicting factors, eating habits are one of the most important, being the sweet eating habit one of the most relevant. 6
Which surgery would be ideal for the sweet eating patient is still a controversial topic in the literature. On one hand, some authors consider that sweet eaters should be offered gastric bypass surgery due to the benefits of dumping syndrome, while restrictive procedures would not have room for these types of patients. 7 On the other hand, some other authors state that purely restrictive procedures like the adjustable gastric band could be offered to this kind of patients, without compromising the outcomes.8,9 This matter remains controversial among procedures like vertical banded gastroplasty, gastric bypass, and adjustable gastric band; however, data evaluating outcomes after SG in this subgroup of patients are scarce in the literature. SG is a novel procedure that has been showing encouraging results, not only demonstrated by weight loss but also by resolution or improvement of comorbid conditions. 10 Surprisingly enough, there is increasing evidence that this operation is not only a restrictive procedure but also some hormonal changes are involved in its mechanism of action, justifying excellent results in the short and medium term.10,11–13 The action of ghrelin has been already demonstrated after SG. It has also been shown that this orexigenic hormone is produced mainly in the stomach fundus, and its level significantly decreases after SG, remaining low over time.11,14
In this context, the inquiry on which would be the effect of the sweet eating habit on patients undergoing SG arises, and the evaluation of this phenomenon is the purpose of this study.
Materials and Methods
This was a cross-sectional retrospective study of a patient cohort who underwent SG between 2006 and 2011 at the Bariatric Surgery Program at Hospital Privado Centro Médico de Córdoba.
There were two groups of subjects:
Group A, was used as a control group and it was composed by:
• Healthy nonobese individuals (nonoperated). • Both female and male. • ≥18 years old. • Answering a questionnaire about sweet eating habits.
Group B, was the focus of our study:
• Obese patients who underwent SG. • Both female and male, ≥18 years old. • Follow-up ≥6 months, periodically, with the multidisciplinary team (twice/month during the first year and every 6 months after that). • Answering a questionnaire about preoperative sweet eating habits.
Demographics and questionnaire results were compared between these two groups.
Subsequently, the following results in Group B were analyzed after surgery:
Demographic data:
• Gender. • Age at the time of the surgery. • Time elapsed since surgery.
Anthropometric data:
• Body mass index (BMI) using the Quetelet formula [weight (kg)/height2 (cm)]; weight was measured using an electronic scale (SYSTEL®) and height was calculated with the altimeter without shoes. • Percentage excess weight loss (%EWL) was calculated as follows: [(initial weight − current weight)/(initial weight − ideal weight)] × 100; %EWL was evaluated at 6, 12, and 24 months postop.
Results in terms of weight loss (%EWL) were classified as follows (Baltasar Success Classification):
Excellent: >65% EWL and BMI <30 kg/m2.
Good: 50%–65% EWL and BMI 30–35 kg/m2.
Poor: <50% EWL and BMI >35 kg/m2.
Questionnaire
Eating habits were investigated to determine preoperative sweet eating pattern, using an adapted questionnaire from the “Anti-Cancer Council of Victoria Food Frequency Questionnaire, Australia,” considering eating customs in the Argentinean population (Appendix 1). This questionnaire was given to the patient after the operation, during one of the follow-up visits.
The questionnaire consisted of a list of 10 groups of sweets where the patient had to select the frequency of consumption in a range from 1 (never) to 10 (3 or more times per day). The minimum score was 10 (if the patient marked “never” for all the items), 100 being the maximum score.
Sweet consumption was classified according to the score as follows:
• Mild: 10–39 points. • Moderate: 40–69 points. • Severe: ≥70 points.
Statistical analysis
Uni- and bivariate logistic regression analysis according to each variable was performed, using the Data Analysis and Statistical Software, version 11.
Results
Group A (nonobese healthy individuals) was composed by 50 subjects; 21 (42%) were male; and mean age was 34 ± 9 years (range 24–61). Initial BMI was 23 ± 3 kg/m2 (range 18–28). Group B (obese subjects) was composed by 157 patients; there were 57 (36%) male; and mean age was 41 ± 10 years (range 19–66). Initial BMI was 46 ± 8 kg/m2 (range 35–86), and mean excess weight was 58 ± 23 kg (Table 1).
BMI, body mass index; NS, non-significant.
Sweet consumption
Group A
Mean score of sweet consumption was 40 ± 11 (range 19–71); female group had a greater score, although the difference was not statistically significant.
When patients were classified according to the score, 98% of them were within the mild and moderate category.
Group B
Mean score of sweet consumption was 38 ± 14 (range 10–73); female group had a greater score, although the difference was not statistically significant.
When patients were classified according to the score, 97% of them were within the mild and moderate category (Tables 2 and 3; Figs. 1 and 2).

Group A, distribution of categories according to gender.
Group B, distribution of categories according to gender.
When analyzing sweet consumption upon gender, male group score was distributed mostly within the lower categories in both groups (Table 4A, B).
Relationship between weight loss and sweet consumption
Patients from Group B were reevaluated at 6, 12, and 24 months after surgery; the percentage of patients in follow-up was as follows: 157 (100%), 111 (71%), and 23 (15%), respectively. Evolution of BMI at 6, 12, and 24 months was: 33 ± 5 (range 25–55), 30 ± 5 (range 20–51), and 33 ± 9 (range 22–56), respectively; %EWL was 66% ± 15 (range 32–101) at 6 months, 77% ± 19 (range 30–129) at 12 months, and 70% ± 22 (range 28–113) at 24 months (Table 5).
BMI, body mass index; %EWL, percentage excess weight loss; SD, standard deviation.
At 6, 12, and 24 months follow-up, %EWL did not show statistically significant difference among categories (Table 6) (Fig. 3).
Relationship between weight loss and sweet consumption.
% EWL, percentage excess weight loss.
Nine (5.7%) patients were not considered successful after surgery (%EWL <50); all of them belonged either to the mild 7 (78%) or moderate 2 (22%) sweet consumption categories. None of them fell in the severe category.
Discussion
There are scarce data in the literature about the relationship between the sweet eating behavior and weight loss after bariatric surgery. This report is not intended to draw any early conclusions about this matter; however, this is an observation from our experience from our patient population.
Upon reviewing publications considering bariatric surgery in general, two authors reported that “sweet eaters” would have worse results in terms of weight loss than “nonsweet eaters,” two authors did not find any link between these variables, and another one considered sweet eating behavior as a predicting factor of good results.7,8,15–17
In 1996, Sugerman et al. published a prospective randomized study comparing vertical banded gastroplasty and gastric bypass surgery in “sweet eater” versus “nonsweet eater” patients. They concluded that the sweet eater patients should be offered gastric bypass. 7 Certainly, this study established among the bariatric surgeons' community, the concept of not offering restrictive procedures to sweet eater patients. Sixteen years later, Hudson et al. from Australia qualified this concept as a myth in regards to the adjustable gastric band. 9
Sugerman argued that gastric bypass would show better results compared to purely restrictive procedures, due to the dumping syndrome associated to this procedure. This would prompt the patients to avoid the sweet eating behavior due to the malaise caused by this syndrome. 7 Interestingly enough, some SG patients also experienced symptoms suggesting the presence of dumping syndrome. This observation was confirmed by Tzovaras et al., who conducted a study with 31 patients to whom dumping syndrome was induced by administration of glucose. They concluded that SG could become a valid alternative for sweet eater patients. 18
Ruiz-Tovar et al. 17 conducted a study on 50 patients undergoing sleeve gastrectomy (SG). They evaluated the effect of preoperative eating habits and preoperative weight loss on these patients. They observed that at 24 months, %EWL in sweet eaters was 78.3% versus 93.9% in nonsweet eaters (P < .001). They concluded then that preoperative sweet eating behavior affected SG outcomes.
One of the weak points of our study is the short-term follow-up. Even though major weight loss was observed during the first 6 months of follow-up, it would be interesting to know the evolution over time. There are some published data with more than 5 years follow-up, showing steady weight loss after SG, although there is a considerable weight regain rate, similar to the one reported for long-term follow-up after gastric bypass.11,12,19 Under these circumstances, Sugerman observed the evolution in gastric bypass patients. He concluded that even though the difference was not statistically significant at 1, 2, and 3 years, “nonsweet eater” patients showed better weight loss than “sweet eater” patients. Therefore, short- and long-term results in our patients need to be elucidated.
Although this was not the primary objective of this study, we cannot avoid wondering about two topics that still have no clear answer, thus making more difficult patient evaluation in our daily practice:
• When could the patient be considered a “sweet eater”? • How and when is the best way to evaluate this patient?
The ideal questionnaire for evaluating sweet consumption should be simple for the patient to respond, easy to understand, reproducible, and as precise as possible. However, it is well known that there is an underestimation from the patient's point of view while answering about his/her own food eating habits on these type of questionnaires (even more when referring to sweet and fatty food). 20
There are diverse methods to evaluate sweet eating habits. Different items like caloric intake coming from sweet food, type of food consumed, frequency, and relationship between sweet intake and emotional factors, among others can be inquired.7,9,21 We utilized the “Anti-Cancer Council of Victoria Food Frequency Questionnaire, Australia” (sweets section) adapted to similar type of food for our region, like Hudson et al. did. 9 Three groups were considered according to the score: mild, moderate, and severe sweet consumption. To somehow validate our results, we compared questionnaire results between two groups: nonobese subjects versus obese patients. Interestingly enough, no difference was found either in the sweet eating score or in the distribution among the different categories of sweet consumption between the two groups. Moreover, distribution of categories upon gender was similar among groups.
Regarding the timing of the sweet consumption evaluation, there is some variability within the literature. Some authors like Sugerman evaluated the eating pattern during the preoperative period. Some others did it postoperatively, inquiring about the preoperative habits. 7 It turns out difficult to decide which would be the best timing. The theoretical advantage of filling out the questionnaire during the preoperative period and, therefore, obtaining contemporary data contrasts with the fear or the fantasy that the patient could have about his/her answers interfering with the timing or even the approval of the operation. In that sense, when the patient is interrogated during the postoperative period, less conditioning factors could be present, especially if the patient had favorable outcomes like the group analyzed in this report. In our experience, the questionnaire was administered during the postoperative period, like other authors did. 9
We were able to evaluate 157 patients, with 111 of them being reevaluated at 12 months. Almost all of the patients (97%) fell within the first two categories (mild and moderate) of sweet consumption. When our primary objective was evaluated, no statistically significant difference in terms of weight loss was found among the different groups at any time in the follow-up period. Mean score for sweet consumption was 38 (range 10–73). This result was just slightly inferior to Hudson's experience using the same questionnaire, but for adjustable gastric band surgery. 9 This mild difference cannot be attributed to eating habits in our region, since there is no control group in our study. Similar to Hudson's experience, there was no difference between men and women when comparing sweet eating habits (P = NS). 9
Interestingly enough, failure rate in terms of weight loss was low, considering that only nine patients (5.7%) had a %EWL below 50. This high success rate should not be surprising if we consider that there was short-term follow-up and that this was a selected group of compliant patients who had regular follow-up by the multidisciplinary team. Moreover, these encouraging results could be matched with those reported in the literature, where the SG has comparable outcomes to those after gastric bypass surgery, the Gold Standard operation.10,22–24
Conclusion
Our preliminary data suggested that preoperative sweet consumption does not predict outcomes after SG in terms of weight loss in the short-term follow-up. Longer follow-up in a larger group of patients is needed to draw better conclusions.
Disclosure Statement
No competing financial interests exist.
Footnotes
| Per month | Per week | Per day | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Never | ≤1 Time | 1–3 Times | 1 Time | 2 Times | 3–4 Times | 5–6 Times | 1 Time | 2 Times | ≥3 Times | |
| Chocolates | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Jam, honey, caramel | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Pastries, cakes, sweet tart dough, etc. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Chocolate milk, condensed milk | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Ice cream, popsicles, etc. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Sugared cereals, cereal bars, sweet popcorn | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Cookies or filled cookies | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Candies, sugared gum, lollipops | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Regular soda, regular juice, sweet beverages | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Sugar | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |