
Abstract
Abstract
Laparoscopic repair of ventral hernias gained strong popularity in the late nineties with some of the early enthusiasm lost later in time. We review the current status and challenges of laparoscopy in ventral hernia repair and best practices in this area. We specifically looked at patient and hernia defect factors, technical considerations that have contributed to the successes, and some of the failures of laparoscopic ventral hernia repair (LVHR). Patients best suited for a laparoscopic repair are those who are obese and diabetic with a total defect size not to exceed 10 cm in width or a “Swiss cheese” defect. Overlap of mesh to healthy fascia of at least 5 cm in every direction, with closure of the defect, is essential to prevent recurrence or bulging over time. Complications specifically related to surgical site occurrence favor the laparoscopic approach. Recurrence rates, satisfaction, and health-related quality of life results are similar to open repairs, but long-term data are lacking. There is still conflicting data regarding ways of fixating the mesh. The science of prosthetic material appropriate for intraperitoneal placement continues to evolve. The field continues to be plagued by single author, single institution, and small nonrandomized observational studies with short-term follow-up. The recent development of large prospective databases might allow for pragmatic and point-of-care studies with long-term follow-up. We conclude that LVHR has evolved since its inception, has overcome many challenges, but still needs better long-term studies to evaluate evolving practices.
Introduction
T
Ventral hernias are primary in nature and incisional hernias result from a prior incision or trauma; they are often discussed together, but it is becoming common to treat these as separate entities.6,7 Popular techniques for open ventral hernia repairs (OVHR) were described by Rives (retromuscular), 8 Stoppa (preperitoneal), 9 and Wantz. 10 Further development and advances in the field led to techniques creating myofascial flaps by component separation of the lateral abdominal wall to aid in repair.11,12 These all proved to be effective, however, with associated morbidity. After Karl Leblanc's initial description of the laparoscopic ventral hernia repair (LVHR) with mesh, this minimally invasive technique gained popularity and was adopted by surgeons over the ensuing years. The principles of LVHR incorporate Pascal's Principle of hydrostatics, in which equal forces in an enclosed fluid space act equally at all points. In addition, those forces that cause hernia formation are the same forces, which, after repair, are used to secure the mesh in place. 13 Proponents of laparoscopic repair reported decreased hospital stay, decreased pain, decreased wound infection rates, and earlier return to work among the advantages for this approach.3,14,15
LVHR became the operation of choice for many surgeons.16,17 However, there is a learning curve associated with it.13,18 Early in its adoption, support was limited to single-institution studies.3,19,20 This was further validated by prospective randomized trials with short-term data, which showed noninferior results compared to the open procedure, and in some situations, improvement in outcomes.15,21,22 Despite these reports, only 22%–27.4% of incisional hernia repairs were performed by a laparoscopic approach, and its use among surgeons lagged compared to other complex laparoscopic procedures.23–25 Widespread adoption may have been prevented by the relative advanced nature of this technique. 26 As time progressed, momentum shifted with less enthusiasm in the literature toward laparoscopic repair than previously reported.27–30 Experts in the field realized that laparoscopy should not be applied to all patients 31 and preoperative selection was important to determine the best patients for this approach. The one clear benefit overall, compared to the open repair, remained the decreased wound infection rate due to smaller incisions and less dissection.15,32 However, skepticism built based on reports of late recurrences due to slow migration and contracture of mesh, bulging, and other complications.27,28,30,33,34 It also appeared that when complications occurred, they were more severe with up to 23% requiring surgical intervention.15,27,28,35 Over time, this led to a paradigm shift back to the open repair, particularly for large hernias.
For nearly 25 years, LVHR has been an option for surgeons. Controversies persist, and evaluation of published reports has yet to definitively answer questions regarding the best indications and techniques for laparoscopic repair. In recent years, reports have been published to guide the operative workup and provide algorithms for laparoscopic surgery.36,37
Our review of the current topics surrounding laparoscopic repair of ventral hernia will examine ventral hernia factors, patient factors, technical challenges in laparoscopic hernia repair, new technologies, and the future role of data registries and prospective trials.
Ventral Hernia Factors
The surgical approach to repair a ventral hernia is dependent on multiple factors, some of which are related to the morphology of the defect. The significance of size, multiplicity and location of hernias, whether primary or recurrent, and presence of symptoms will be discussed separately below. During the preoperative workup, these characteristics must be considered congruently when formulating a surgical plan (Table 1).
IDDM, insulin-dependent diabetes mellitus.
Size
The ideal size of a hernia to be repaired laparoscopically ranges from 2 to 10 cm in width. Ventral hernia defects that are small in size (<2 cm) can be managed with a simple open approach, often with suture-only repair and do not require a laparoscopic or more elaborate procedure.27,36,38 In addition, if the defect is small enough, general anesthesia can be avoided and the repair performed with local anesthesia alone. Large-size defects, on the other hand, pose different challenges. There are various definitions in the literature of large or giant hernias, but for our purposes, these terms describe hernia defects with a width >10 cm. Large hernias result in abdominal wall dysfunction and might result in bulging when repaired laparoscopically with intraperitoneal onlay mesh (IPOM). 39 In addition, with such a large defect, there is likely deficient peripheral tissue to safely secure the intraperitoneal mesh with adequate overlap. 40
Although reports of successful laparoscopic repair of large hernias have been published, 41 a laparoscopic approach does not allow for primary myofascial closure of the anterior abdominal wall. Still controversial, performing a bridge-only repair in contrast to primary closure, as classically described by LeBlanc, results in an inadequate repair.2,42 That being said, there are many advocates for a laparoscopic repair of large-sized defects.41,43 A published review of 310 patients who underwent laparoscopic incisional hernia repair showed a significant difference in recurrence between patients with a defect <10 cm and patients with a defect >10 cm. The cohorts were organized into three groups <10, 10–12, and >15 cm with recurrence rates of 0.4%, 20%, and 41.2%, respectively. 44 Based on this study and others, it is our experience that LVHR should be restricted to defects that are between 2 and 10 cm in size.
Multiple and nonmidline defects
The majority of ventral hernias are midline along the linea alba. However, there are many patients who suffer from multiple and simultaneous defects, affectionately referred to as “Swiss cheese” defects. There are also hernias in locations other than midline such as in the lumbar suprapubic and subcostal areas, which can be challenging to repair. Swiss cheese defects may be known preoperatively or found intraoperatively. 45 A benefit of the laparoscopic approach is that all defects can be identified, reduced under direct vision, and repaired with proper mesh overlap. Swiss cheese defects have been reported to have an increased rate of recurrence, 46 however, many surgeons prefer a laparoscopic approach for these hernias for the reason described above. Nonmidline hernias, especially when primary, are uncommon and potentially challenging to repair. They can be treated laparoscopically with adequate results, but should be approached with caution and reserved for those comfortable with advanced laparoscopic techniques. 47
Recurrent hernias
Most cases of repair of recurrent hernias through a laparoscopic approach are intermixed with primary repair and not studied independently. Single-institution studies have shown moderate success with this approach in experienced hands.48,49 Theoretically, laparoscopy allows for access through a different and new incision site to avoid previously placed incisions and areas of scar/adhesion. It also allows for direct visualization of occult defects. 42 However, because of adhesions, there is an increased risk of bowel injury. 49 In a study evaluating the presence of adhesions during revision laparoscopic hernia repair, following an initial laparoscopic hernia repair, 47.05% had no adhesions, 42.3% had adhesions of the omentum, and 10.58% had adhesions of bowel serosa. 48 Another retrospective review, supporting the use of laparoscopy, looked at 69 patients with recurrent incisional hernias repaired laparoscopically demonstrating low repeat recurrence rate with an overall morbidity of 13% and bowel injury of 4.3%. 49 Repairing recurrent hernias through a laparoscopic approach is possible, but should be considered only in select patients and by surgeons with experience in advanced laparoscopic techniques. 36 Initial access should be completed with heightened awareness to avoid bowel injury.
Patient Factors
Every patient is different and should be treated as such. The patient's presentation, medical and social history, as well as compliance with care, all play a significant role in determining the best repair of their ventral hernia. Below we look at how patients' own characteristics influence the repair of their hernia (Table 1).
Obesity
Obesity is an ever increasing problem encountered in the United States with nearly one-third of the U.S. population classified as obese. 50 The occurrence of ventral hernias is increased in this patient population. 50 They are also prone to larger defects and increased complications overall.37,50 Many state that laparoscopic hernia repair is useful and indicated in obesity because it avoids a large incision and decreases complications, hospital stay, and recurrence rate compared to the open approach.32,51,52 This thought gained more support over time, and from 2008 to 2009 (in the era of obesity), the use of LVHR increased from 6.5% to 28%. 52
A retrospective review of the American College of Surgeons National Surgical Quality Improvement Program database demonstrated that open hernia repairs, compared to laparoscopic, in Obesity Classes I/II/III have increased odds of superficial surgical site infection, deep surgical site occurrences, and dehiscence. 50 It may be difficult to primarily close the defect; however, in the case of the obese patient, the importance of decreased wound infection may outweigh the risk of primary fascial closure. Patients who are candidates for bariatric surgery should undergo weight loss before repair of hernia. One study has shown that hernia repair can be performed at the time of bariatric surgery. 53 Eid et al., presented an algorithm for hernia repair when dealing with the morbidly obese. 4 The components of deciding to repair a hernia first versus pursuing bariatric surgery versus combined surgery depend on the anatomy of the hernia and symptomatology. 4
Diabetes and other medical conditions
Diabetes is known to increase surgical risk. A recent study looked at the risk of insulin-dependent diabetes mellitus (IDDM) versus noninsulin-dependent diabetes (NIDDM) and its relationship to complications in the repair of ventral hernias. In open repairs, IDDM increased rates of overall, surgical (such as superficial, deep, or organ- space infections, and wound disruption), and medical (such as deep venous thrombosis, pulmonary embolism, unplanned reintubation, ventilator dependence >48 hours, acute renal failure, coma, stroke, cardiac arrest, etc.) complications. In the laparoscopic cohort, insulin-dependent diabetes was related to an increased risk of overall and medical complications of the patient, but it was not directly related to complications of the surgery. NIDDM was not associated with an increased risk of morbidity in either laparoscopic or open procedures. 54 Insulin-dependent diabetes is therefore a risk to both patient populations, but the use of minimally invasive approaches in this cohort may lead to lower surgical complications compared to an open procedure. The authors state that the difference is subtle between open and laparoscopic surgery in this group. 54
Caution should be observed in patients with cardiopulmonary problems because insufflation and increased intraperitoneal pressure can compromise their pulmonary status. 55 Laparoscopy is not contraindicated in other disease states such as Cirrhosis Childs A-B. 37 In cirrhotic patients, great care should be taken to look for and avoid reconstituted umbilical veins and other collaterals when trocars are placed in the umbilical area.
Smoking
The reports on the effects of smoking in patients undergoing laparoscopic hernia repair are conflicting. A single-center retrospective study of 194 patients undergoing either LVHR or OVHR did not show an association between smoking and complications or recurrence after LVHR; however, in that study there was an association between hernia recurrence and smoking in patients who had an open repair. 56 In contrast, a different retrospective study from 2009 did find smoking to increase the rate of recurrence after LVHR. 57
Technical Challenges in Laparoscopic Hernia Repair
In the operating room and thereafter, the surgeon will confront many challenges when trying to properly repair a ventral hernia laparoscopically. Ongoing topics of discussion are primary fascial closure, type and location of mesh, and the different techniques for securing the mesh (Table 2).
ePTFE, expanded polytetrafluoroethylene.
Closing the defect
The original and classic description of laparoscopic hernia repair is simple reduction of the hernia and placement of IPOM. 2 This achieves all the goals of hernia repair except restoration of abdominal wall anatomy and function. Recent studies have discussed the use of “IPOM plus” in which the hernia defect is closed primarily. 42 The argument in favor of such an approach is that it anatomically reconstructs the abdominal wall, while decreasing the risk of bulging, and will provide a larger surface area for the mesh to be attached. 58 A retrospective study of 128 patients showed a recurrence rate of 19.18% when the defect was not closed and a recurrence of 6.25% when the defect was closed, although this did not reach statistical significance. 59 A meta-analysis of several studies found that primary fascial closure compared to nonclosure resulted in lower recurrence rates (0%–5.7% versus 4.8%–16.7%) and lower seroma rates (5.6%–11.4% versus 4.3%–27.8%). One of the studies included in this meta-analysis evaluated abdominal wall function and bulging and found better outcomes with primary closure, with also more satisfied patients (Nguyen). 60 There are multiple additional studies that show decreased recurrence when the defect is closed,1,42,61,62 and one that does not show a difference in recurrence between closure and nonclosure. 63
To perform an adequate closure, the linea alba or edges of the hernia defect need to be reapproximated. Multiple techniques have been described on total laparoscopic closure of the defect. 60 If primary myofascial closure cannot be achieved, then a hybrid procedure should be performed or the surgery should be completed with an open approach (except, perhaps, in the obese patient). We support the routine closure of the hernia defect, and if needed, a component separation (including external oblique release, posterior rectus fascia release, and/or transversus abdominis release).
Type of mesh and mesh location
The laparoscopic approach places a mesh in the peritoneal space against the anterior abdominal wall. There are numerous reports in the open repair literature as well as laparoscopic literature supporting the safety of this technique.2,64,65 The type of mesh used should allow for intraperitoneal placement without causing significant adhesions to the intra-abdominal contents, while integrating well into the anterior abdominal wall. 66 Meshes with elastic properties may be more comfortable for patients and may result in decreased recurrence rates. 67 There are many different meshes to choose from, including synthetic, biologic, or composite mesh. Synthetic meshes are made from different compounds that commonly include polypropylene, expanded polytetrafluoroethylene (ePTFE), or polyglycolic acid.
The current standard of practice in open hernia repair is to use large-pore, monofilament light-weight synthetic meshes when possible, however, due to risk of adhesions in the intraperitoneal space, this is not possible when performing a laparoscopic approach. 66 A commonly used mesh in the past was ePTFE, however, innovations with synthetic materials and their combination or coating are changing practice. 66 When possible, most surgeons prefer to use a synthetic mesh when repairing ventral hernias. Studies in the past have evaluated the recurrence rates of hernia determined by the different types of synthetic mesh used in the procedure, but there has not been a clear advantage of one synthetic mesh over the other. 68 In addition, the rapid change within this industry over time makes it exceptionally challenging to study different meshes in an expedient and proper scientific manner. Characteristics of mesh, which may lead to recurrence, include shrinkage and adhesions, although this has never been systematically proven.
The use of biologic mesh for laparoscopic ventral hernia has been studied. The LAPSIS trial compared open retromuscular (mesh augmentation) versus laparoscopic repair (mesh bridging technique) using either a noncross-linked biological mesh or a synthetic mesh for primary and incisional hernias with a diameter of 4–10 cm. This trial was stopped early due to a low rate of patient recruitment, incompleteness of the study data, and higher preliminary recurrence rate in the biologic mesh groups. The results from the acquired data showed early recurrence rates in the biologic group, 19% versus 5% after laparoscopic repair and 11% versus 3% after open repair. 69 Obviously, because a formal analysis of the study was not completed, the results need to be evaluated with caution.
As mentioned previously, a purely laparoscopic approach will usually result in intraperitoneal placement of mesh. However, if a hybrid procedure is performed, then there are more anatomical spaces to use for mesh placement. A large review of 62 studies with 5824 patients' status post ventral hernia repair found that the highest recurrence rates in open procedures were in onlay (17%) and inlay (17%) and the lowest recurrence rates were with retromuscular (5%) and intraperitoneal mesh (7.5%). 70 Patients from the same review who underwent laparoscopic repair and IPOM had a recurrence rate of 6%. 70 Regarding the type of mesh for each location, polypropelene meshes should be placed in the extraperitoneal space, ePTFE and other composite meshes can be placed in the intraperitoneal space, and as discussed earlier, the use of biologics in any location remains controversial. 71 The ideal location for mesh is in a sublay position (retromuscular, preperitoneal, or IPOM if purely laparoscopic); however, further research needs to be performed to determine if there is a difference in recurrence and complication between these variable sublay positions.
Mesh fixation
One of the advantages of IPOM is that mesh adherence is promoted by abdominal wall pressure. 13 During the laparoscopic approach, the mesh, however, needs to be secured in the correct position with appropriate overlap in all directions.42,72 A meta-analysis showed a decrease in hernia recurrence rate from 8.6% to 1.4% when there was an increase in mesh overlap from <3 to >5 cm, respectively. 72 Securing the mesh to the anterior abdominal wall is performed by multiple techniques. Suturing, stapling, tacking, glue application, and combinations of techniques have all been described in the literature. 73 The most commonly used method is by tacking the mesh circumferentially with four-corner transfascial sutures. 73 Every surgeon has a preference; however, the technique performed may play a role in intraoperative and postoperative care. Transfacial sutures inherently take longer time to place than tacks, and there is debate about the pain caused by nerve entrapment by the sutures. It has been shown that patients undergoing laparoscopic hernia repair have more reported early postoperative pain than any other minimally invasive operation, which sometimes requires inpatient status. 38 A common understanding is that postoperative pain is directly related to the mechanisms of mesh fixation to the anterior abdominal wall; therefore, it is an important consideration when using laparoscopic repair.
Recurrence rates between spiral tacks and suturing of the mesh do not appear to be different.73,74 Suturing of the mesh may create less mesh shrinkage and have a higher tensile strength compared to tacking the mesh; however, this has not been shown to produce a difference in recurrence. 75 The long-term outcome of pain does not appear to be dramatically different between the two techniques either, with conflicting reports regarding intensity of early postoperative pain.73,75,76 There are various types of tacks, including absorbable and permanent. A nationwide study showed an increased recurrence rate after the use of absorbable tack fixation with a hazard ratio of 1.53. In this study, patients were screened for recurrence by a questionnaire, and any response that prompted suspicion was followed by a physical exam and CAT scan if needed. 77 Previous studies have looked at the mechanics between different tackers suggesting that titanium tacks should be used if perpendicular deployment cannot be assured. 78 The major difference between fixation techniques is that the operative time is significantly longer when using transfascial sutures, including up to at least 1 additional minute of surgery for each suture placed. 73 Complication rates are similar between techniques. 73 Cost does not appear to be affected because the quicker tacking is offset by the cost of the tack applicator. 73
There are small studies reporting the use of fibrin glue for mesh fixation, but not enough data are available yet to support its use. 74
Complications
Most studies suggest that laparoscopic surgery compared to the open approach has decreased wound infection rates15,26,30,33,79; however, a comparable infection rate was noted in a meta-analysis of incisional hernias published in 2015. 80 There are no studies, which compare open and laparoscopic hernia repair, that clearly demonstrate an improved or worse outcome when it comes to recurrence rate. 28 Recurrence rates are similar to open repairs, and are generally sited as <10% in most studies.28,80 Reasons for recurrence include mesh overlap <5 cm, poor fixation of mesh, mesh integration into the defect, surgical site infection, obesity, size of defect, and recurrence.26,72,80 Hernia repairs need to be followed for >5 years and likely for a lifetime to know the long-term recurrence rates. 81
Bulging (Fig. 1) remains a major problem of laparoscopic repair, particularly if the primary defect is not closed, with a reported incidence of 21.5%.30,32 In accordance with LaPlace's Law, a large abdominal wall defect repaired with mesh will succumb to internal pressure acting as a “sail in the wind,” which will be prone to bulging. 55 Pseudorecurrence from eventrations (of mesh or tissue) and from seroma formation is clinically significant because they can mimic a hernia recurrence. 1 Clinically significant seromas occur 3%–20% of the time; insignificant hernias can occur up to 100% of the time.1,55,82 Seromas should only be aspirated if there are repeated complaints from patients because introduction of a needle increases the risk of surgical site infection. 1 The best form of treatment may be prevention of seroma by primarily closing the defect rather than bridging with a mesh. 1
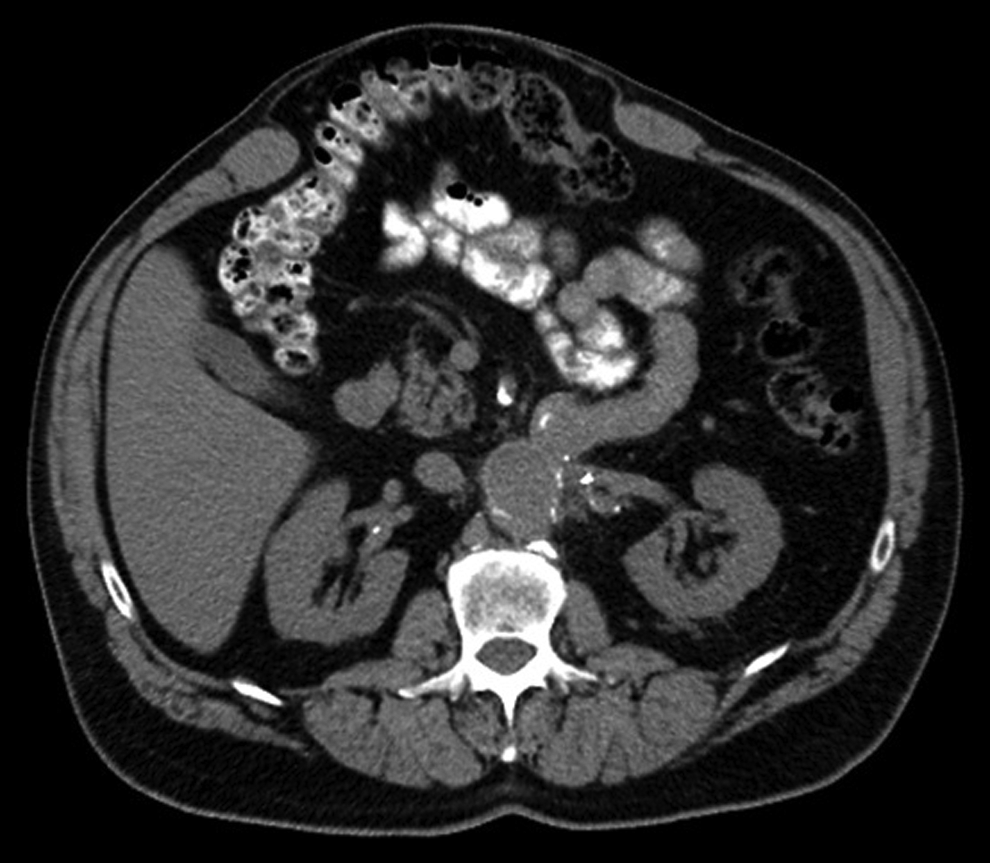
CT scan demonstrating significant bulge after intraperitoneal onlay mesh without repair of the fascia. Photo courtesy of Dr. Mike K. Liang.
Factors that contribute to hernia formation include open hernia repair, hernias that were never spontaneously reducible, patients with more abdominal incisions preoperatively, and those who did not have drains placed. 82 Eventration is directly correlated with size of hernia and failure to close the defect. 1 Eventration is not related to the amount of mesh overlap. 1 Port-site hernias are another complication and occur <1%–2.5% of the time.30,42
Bowel injury is more common in laparoscopic repairs with a rate of 1.7%–4.3%.15,83,84 Bowel injuries, particularly if not recognized, lead to severe complications, including death. 83 In experienced hands, enterotomy can be repaired laparoscopically, but fecal contamination requires abortion of the repair or conversion to an open approach. 27 Some studies suggest less pain with the laparoscopic approach, possibly due to smaller incisions and the use of tackers instead of transfacial sutures; however, this remains controversial as mentioned in the previous section. 80 Smaller, less notable incisions provide an advantageous cosmetic result in laparoscopic repair, but bulging can be noticeable and unsightly. Quality of life appears to be equal overall between open and laparoscopic approaches, with one study of 710 patients showing worse quality of life in the early postoperative period after undergoing laparoscopic repair.15,24,73,76 When evaluated alone, however, LVHR improves patient satisfaction from preoperative scores.15,85
Robotic Approach and Future Technology
Advances in technology will continue to heavily influence the forward progress of surgery. Robotic innovations in the operating room have played prominent roles over the last decade and have a stable role in intra-abdominal procedures. In 2012, Allison et al. published their experience of robotically repaired ventral hernias in 13 patients with acceptable results. 86 They reported several advantages to the robot over laparoscopy, including the following: six degrees of freedom with the endowrist, less abdominal wall trauma, the ability to perform circumferential suturing allowing for maximal mesh overlap, avoidance of transfacial sutures and tacks, and easier primary closure. 86 Another retrospective review compared primary closure of hernias with mesh placement by the robot versus traditional laparoscopic repair and IPOM. Complication profile and hernia recurrence favored the robotically repaired group with only an additional 19 minutes of operative time. 87 The current discussions surrounding robotic repair in the surgical community are exciting and it appears that the advantages of this technique lend themselves to a frontier that mandates further exploration to assess their true benefits.
Data Registries and Prospective Randomized Trials
As discussed above, the major problem facing surgeons today is the variability by which ventral hernias are repaired. There are many different tools, prosthesis, and techniques that can be used, with little evidence in each area. A review of the literature shows an abundance of short-term retrospective studies with small patient cohorts and subjective interpretations. 80 In 2013, recommendations for reporting outcomes in abdominal wall repair were published after a consensus meeting in Palermo, Italy, to combat these flaws in research. 88
Overall, there needs to be more prospective randomized trials worthy of class-1 evidence to improve the care of patients suffering from ventral hernia. At this time, there are reports of several prospective trials underway in Europe (Labor, TACS, INCH, AWARE, ProLOVE) and the United States (clinicaltrials.gov), which could help answer some pestering questions.89–93 In addition, not only is this an issue for patient care but also has significant implications on our healthcare system and overall costs. With the rapidly changing technology, the cost of conducting a well-designed, prospective randomized trial in each area is prohibitive. The creation and use of detailed national and international data registries are now essential. This will provide a platform to process as much information as possible, including long-term follow-up on the order of years to decades and to allow the conduct of pragmatic trials. The Danish Hernia Database and, more recently, the American Hernia Surgical Quality Collaborative (AHSQC) are models for what is more broadly needed in the international surgical community. 94
Conclusions
LVHR has evolved since its inception, has overcome many challenges, and continues to change rapidly. There are certain patients and ventral hernias that benefit the most from this approach, including the obese and those with multiple defects. There are still some challenges that remain and need to be resolved with proper scientific research. However, despite these challenges, the laparoscopic repair of ventral hernias is here to stay and will continue to develop along with advances in technology, prostheses, and fixation devices.
Footnotes
Disclosure Statement
No competing financial interests exist.