
Abstract
Abstract
Different connective tissue diseases (CTDs), such as dermatomyositis, mixed CTD, rheumatoid arthritis, polymyositis, lupus, and Behçet's, may affect the esophagus, impairing its motor function. The muscular atrophy and fibrosis caused by the autoimmune vasculitis and neuronal dysfunction affect the esophageal body and the lower esophageal sphincter, leading to a clinical presentation of dysphagia and gastroesophageal reflux disease (GERD). The belief that the impaired esophageal motility may negatively affect surgical outcome has led to the common recommendation of avoiding laparoscopic antireflux surgery (LARS) for fear of creating or worsening dysphagia. This review focuses on the evaluation of the outcome of LARS in patients with CTD. Specifically, this review shows that the literature on LARS and CTDs is scarce and most studies have a small number of patients and a short follow-up. Furthermore, a subanalysis of the outcome based on the type of CTD or the manometric profile is still elusive. In the setting of these limitations, it appears that results are good and comparable to those of patients with GERD and without a CTD. Morbidity and mortality are insignificant even considering the systemic manifestations of the CTD. LARS should not be denied to patients with CTD and GERD.
Introduction
C
The muscular atrophy and fibrosis caused by the autoimmune vasculitis and neuronal dysfunction affect the esophageal body and the lower esophageal sphincter (LES). 2 Thus, the esophageal motility disorder secondary to CDT is classically characterized by an absence of peristalsis and a severely incompetent LES. 4 This scenario leads to a paradoxical impairment of emptying of the esophagus and to gastroesophageal reflux, leading to a clinical presentation characterized by dysphagia and gastroesophageal reflux disease (GERD).2,3 Dysphagia is present in 36% of the patients 5 and may compromise nutrition. Malnutrition is present in 15%–30% rate of patients and may ultimately lead to death. 6 There is no effective pharmacological therapy to improve esophageal motility. 3
GERD is also a common problem in CTD, and GERD symptoms may be present in up to 90% of the cases. 7 Moreover, the incidence of esophageal strictures, Barrett's esophagus, and esophageal adenocarcinoma is increased in patients with CTD. 8 GERD in these patients may also determine worsening of the lung disease.2,9 Pharmacological treatment for GERD is effective in most patients with CTD3,8; however, some patients do not do well, particularly those with advanced rheumatologic disease.3,8 Furthermore, pharmacological therapy with proton pump inhibitors may lead to osteoporosis, 10 a serious concern in patients under chronic steroid therapy, and may not improve pulmonary function since aspiration of gastric contents through an incompetent LES is not stopped by medical therapy, with consequent damage as pepsin and biliary salts aspiration is also harmful to the lungs. 11 Thus, laparoscopic antireflux surgery (LARS) may be an option in some patients with CTD. However, the belief that the impaired esophageal motility may determine poor outcomes has led to the common recommendation of avoiding LARS for fear of creating or worsening dysphagia. 12
This review focuses on the evaluation of the outcomes of LARS in patients with CTD.
Laparoscopic fundoplication
A complete work-up, including barium swallow, endoscopy, esophageal manometry, and dual probe pH monitoring, is mandatory in these patients.
Although esophageal manometry is abnormal in most patients, 13 the classical picture of aperistalsis and atonic LES is not always present. Patti et al. 12 showed that in 20 patients with different CTDs and gastrointestinal symptoms, LES and esophageal peristalsis were not different when compared to those of a control group of patients without CTD who underwent LARS. Esophageal peristalsis was severely affected, and most often absent, in patients with end-stage lung disease secondary to CTD. Other described risk factors for greater esophageal dysmotility in patients with CTD are esophagitis, 13 Raynaud's phenomenon, 14 and diffuse skin involvement. 15 High-resolution manometry (HRM) has made easier and more intuitive the evaluation of esophageal peristalsis. Some cases probably classified before as absence of peristalsis on classic manometry actually show residual peristalsis on HRM, now classified as ineffective motility (Fig. 1).
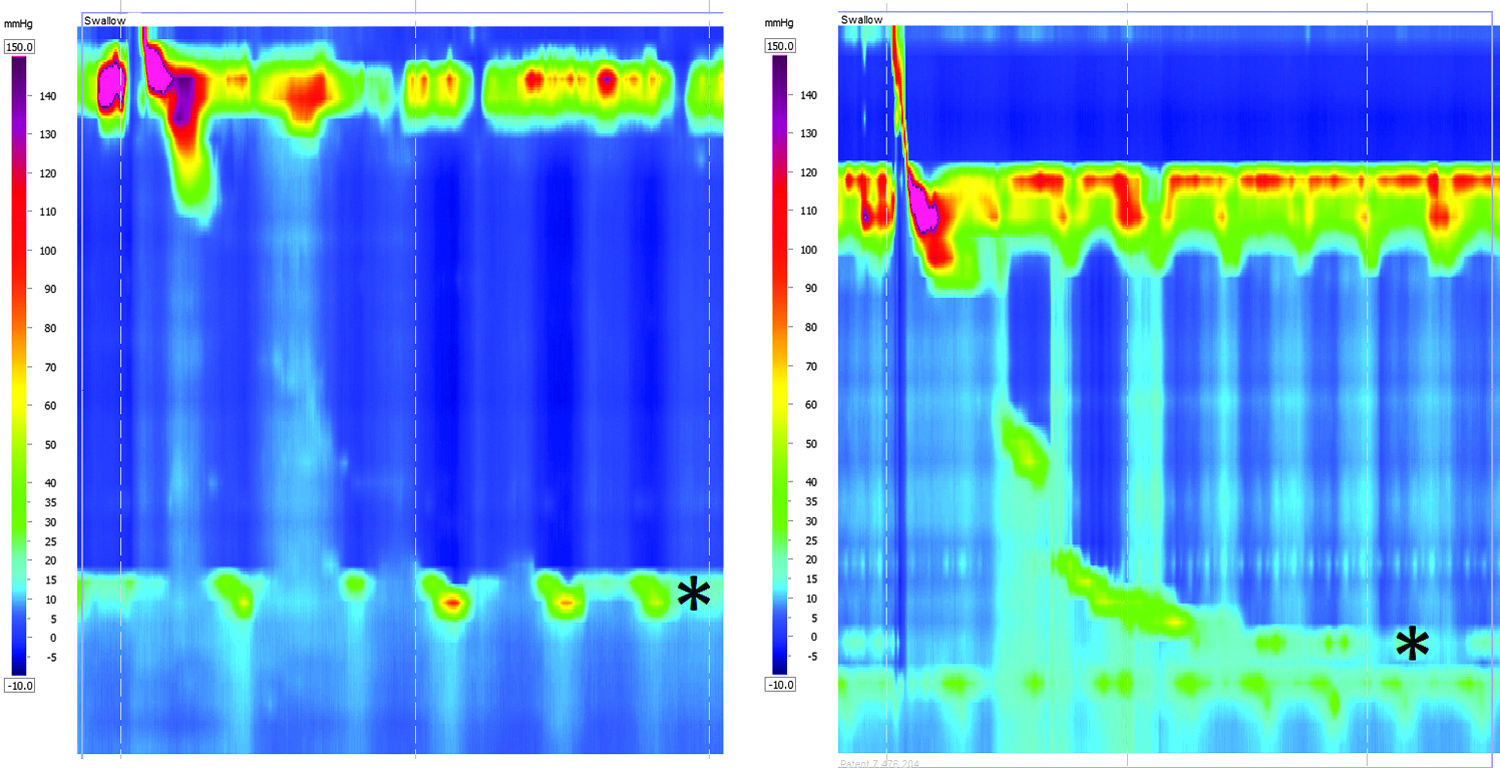
High-resolution manometry findings in patients with connective tissue disorders showing a range from absence of peristalsis (left) to residual peristalsis but ineffective esophageal motility (right). The lower esophageal sphincter (*) is always hypotonic.
Few studies have analyzed the outcome of LARS in CTD patients. Most cases are limited to aperistaltic esophagus 16 or end-stage lung diseases9,17 that may represent a distinct subset of patients.
A partial fundoplication was the procedure of choice in most patients, although a Nissen fundoplication was also used occasionally (Table 1). There was no reported mortality.
Laparoscopic Roux-en-Y gastric bypass
Roux-en-Y gastric bypass (RYGB) is an alternative to recurrent GERD after a fundoplication. 20 A laparoscopic RYGB can be easily accomplished in a nonobese individual and could, theoretically, control GERD and deal well with the motility impairment in patients with CTD. The morbidity associated with the procedure, however, may limit its usage. The only series of RYGB in patients with CTD 18 showed better results for dysphagia, bloating, diarrhea, and GERD score than fundoplication in patients with CTD. The authors considered it an alternative to fundoplication and a better option than an esophagectomy for complicated cases.
Laparoscopic esophagectomy
Although an esophagectomy was more liberally used to treat esophageal complications of CTD in the past, 21 today it is rarely used as it is associated with a high morbidity and mortality. 18
Discussion and Conclusions
In most patients with CTD, LARS is not considered for fear of severe dysphagia. Interestingly, patients with achalasia in whom the esophagus has no peristalsis have a partial fundoplication performed in association with the myotomy to prevent GERD. In patients with CTD and normal esophageal body motility, a Nissen fundoplication is probably an adequate surgical option, but when the manometry shows ineffective esophageal motility or absent peristalsis, a partial fundoplication is chosen.
This review shows that the literature on LARS and CTDs is scarce and all series have a small number of patients and a short follow-up. Furthermore, a subanalysis of the outcomes based on the type of CTD or the manometric profile is still elusive. In the setting of these limitations, results are good and comparable to those of patients with GERD without a CTD. Morbidity and mortality are insignificant even considering the systemic manifestations of the CTD. LARS should not be denied to patients with CTD, particularly when regurgitation and aspiration are present.
Footnotes
Disclosure Statement
No competing financial interests exist.