
Abstract
Abstract
Background:
Although laparoscopic distal pancreatectomy (LDP) is gradually recognized as a safe and effective alternative to open distal pancreatectomy (ODP), it is not yet widely accepted.
Objective:
We describe our experience, with emphasis on the learning curve of LDP.
Methods:
Patients who underwent distal pancreatectomy (DP) between January 2011 and August 2014 were included. Operative and postoperative parameters, as well as pathology reports were evaluated.
Results:
Thirty-nine and 41 patients underwent LDP and ODP, respectively. The mean age and gender distribution were comparable between groups. In six patients (15.4%), a conversion to open surgery was indicated. Operating time and intraoperative blood transfusion rates were comparable between groups. One patient of the LDP group died postoperatively. Postoperative complications were comparable with similar Dindo–Clavien (DC) score. Length of stay (LOS) was shorter following LDP (8.15 ± 4.68 versus 11.3 ± 6.3 days, P = .014). Patients selected to have LDP had larger lesions compared to those who underwent ODP (4.59 ± 4.23 versus 3 ± 2.52 cm, respectively, P = .048). R0 resection rates between the groups were comparable (92.3% in LDP versus 97.5% in ODP) as well as lymph node (LN) harvest (6.4 ± 6.4 LN in LDP versus 7.6 ± 6.6 LN in ODP). Following the 17th patient, LDP operative time decreased by more than 35 minutes, no conversions were done, no blood transfusion was needed, and the LOS was shortened by over 2 days.
Conclusions:
Short learning curve, shorter LOS, and satisfactory short-term oncological outcome place LDP as an attractive alternative for selected patients requiring DP.
Introduction
T
In this study, we examined the perioperative course and clinical outcomes of patients who underwent LDP in comparison to ODP, in a new service for MIS-HPB surgery. The feasibility, safety, and oncological integrity are evaluated with emphasis on the learning curve of the procedure.
Patients and Methods
Patients
Included are all patients who underwent DP for lesions of the pancreatic neck, body, and tail, between January 2011 and August 2014. Five surgeons performed ODP, while one performed ODP and LDP. Laparoscopy was elected based on preoperative imaging. Specifically, tumors involving the great vessels (splenic artery and vein) and those associated with left-sided portal hypertension were rejected from LDP.
Surgical and oncologic parameters and outcomes were analyzed. Patient demographics, type of resection, intraoperative blood loss, duration of surgery LOS, postoperative complications, and 60-day reoperation and mortality were evaluated. Pathological reports were reviewed to assess lesion histology, size, resection margin status, and lymph node (LN) involvement.
Postoperative complications were categorized according to D-C classification. 18 Resection margins were considered positive if the tumor was identified within 1 mm of the resection margins, including the retroperitoneal border. Patient's characteristics and perioperative data are presented in Table 1.
LDP, laparoscopic distal pancreatectomy; ODP, open distal pancreatectomy; pRBC, packed red blood cells; SD, standard deviation.
This study was approved by the Tel-Aviv Sourasky Medical Center institutional review board (IRB).
Surgical technique
Open distal pancreatectomy
The patient is placed in supine position, prepped, and draped. The abdominal cavity is entered through a midline or subcostal incision (per patient's body habitus and surgeon's preference). The lesser sac is entered by taking down the gastrocolic ligament immediately adjacent to the transverse colon, and by dissecting the gastrosplenic ligament, taking down the short gastric vessels.
The pancreas is exposed and the transection site is defined. Intraoperative ultrasound (IOUS) is performed as needed. The spleen is completely mobilized by taking down the phrenosplenic, splenorenal, and splenocolic ligaments, and the spleen and pancreas are rotated medially together.
The peritoneum is incised on the upper and lower borders of the pancreas, and the plane between the pancreas and Gerota's fascia is dissected, facilitating the rotation. If the tumor or desmoplastic reaction is adherent to Gerota's fascia, the dissection is carried out inside the perinephric fat, at the plane of the left renal vein. The IMV is tied and transected at the lower border of the pancreas, if needed. The splenic artery is tied and transected, and a tunnel is dissected between the pancreas and splenic vein. The pancreas and splenic vein are transected. The resection of the pancreas is done using a coated stapler, or sharply, after which the stump is oversewn. A drain is routinely left, and the abdomen is closed
Laparoscopic distal pancreatectomy
The patient is put in partial right-lateral decubitus position, at 45° for distal body and tail lesions and 30° for proximal body and neck lesions. Pneumoperitoneum is achieved by insertion of Veress needle, and four or five ports (two or three 12 mm and two 5 mm) are placed.
The lesser sac is entered by taking down the greater omentum and continuing the dissection to takedown the gastrosplenic ligament. The stomach is retracted. Due to the lateral position of the patient, no retractor is needed. The pancreas is exposed and the transection site is defined. IOUS is performed. The peritoneum at the upper border of the pancreas, where the resection is planned, is incised and the splenic artery is encircled and stapled with a vascular endo-GIA.
The lower border of the pancreas is exposed, the IMV is taken down if needed, and the splenic vein is exposed behind the pancreas. A tunnel is created between the pancreas and the splenic vein, and the organ is transected with a coated stapler. Next, the splenic vein is transected with a vascular endo-GIA. The pancreas is retracted from medial to lateral, at the plane of Gerota's fascia (or deeper, at the plane of the left renal vein, as indicated by tumor invasion), and the splenocolic ligament and the rest of the splenic ligaments are taken down and the specimen is freed. A 4–5 cm extraction incision is created (midline or Pfannenstiel), and the specimen is retrieved in a bag. A drain is left adjacent to the pancreatic stump as a routine
Statistical analysis
Continuous data are expressed as mean and standard deviation. Continuous variables were analyzed using student's t-test. Categorical variables were analyzed using the Fisher's exact test. Kaplan–Meier plots were applied for survival. P-value of .05 was considered significant.
Results
Eighty patients who underwent distal pancreatectomy (DP) between January 2011 and August 2014 were retrospectively analyzed. Forty-one underwent ODP (24 females, mean age 56.9 years, range 10–77), and 39 underwent LDP (27 females, mean age 57.6 years, range 17–79). No significant differences in mean age or gender distribution between groups were noticed.
Mean operative time was comparable between groups with 221.8 ± 77.5 minutes and 242.9 ± 81.2 minutes in the ODP and LDP, respectively (P = .24) (Table 1). Blood transfusion rate was similar between the groups with 0.6 ± 1.49 pRBC units and 0.51 ± 1.25 pRBC units in the ODP and LDP, respectively (P = .73) (Table 1). Eleven and eight patients from the ODP and LDP group required intraoperative blood transfusion. The maximum number of pRBC units given to a single patient was eight and six to patients in the ODP and LDP groups, respectively. Laparoscopy was converted to open surgery in six patients (Table 1). Indications for conversion were bleeding in three patients and poor progression of dissection in the remaining three patients.
One patient in the LDP group died within 30 days of surgery due to severe sepsis attributed to pancreatic leak. There was no significant difference in minor (Dindo–Clavien [DC] score I/II) or major (Clavien score III/IV) postoperative complications between groups (Table 1). Three patients in the ODP group had severe complications (DC 4), indicating intervention: explorative laparotomy in two and transgastric drainage of pancreatic leak in one. Thirteen patients developed pancreatic fistula overall (16.25% total, six and seven patients in the ODP and LDP groups, respectively) with no difference in fistula grade 19 between groups (Table 1).
Mean LOS was 10.8 ± 5.6 days after ODP versus 8.28 ± 4.5 after LDP (P = .03) (Table 1). Eight (19.5%) and 11 (28%; P = .54) patients in the ODP and LDP groups, respectively, were rehospitalized within 60 days from surgery due to various reasons (Table 1). No additional surgical procedures were required during these admissions.
The most frequent lesion in both groups was adenocarcinoma −13 (31.7%) in the ODP group and 14 (36%) in the LDP. Others included solid-pseudopapillary neoplasm, neuroendocrine tumor (NET), mucinous cystic neoplasm, intraductal papillary mucinous neoplasia, and others. There was no significant difference in lesion type distribution between groups (Table 2). Lesion size on pathologic examination was larger in the LDP group (4.6 ± 4.2 versus 3 ± 2.5; P = .04) (Table 2). Mean number of harvested LNs was comparable between groups (ODP 7.6 ± 6.6 versus LDP 6.4 ± 6.4; P = .38) (Table 2). Forty (97.5%) and 36 (92.3%; P = .67) patients in the ODP and LDP groups, respectively, had R0 resection (Table 3). Among patients diagnosed with adenocarcinoma, eight and six in the LDP and ODP groups died during follow-up. There was no significant difference in overall survival between adenocarcinoma patients who underwent LDP versus ODP (Fig. 1).
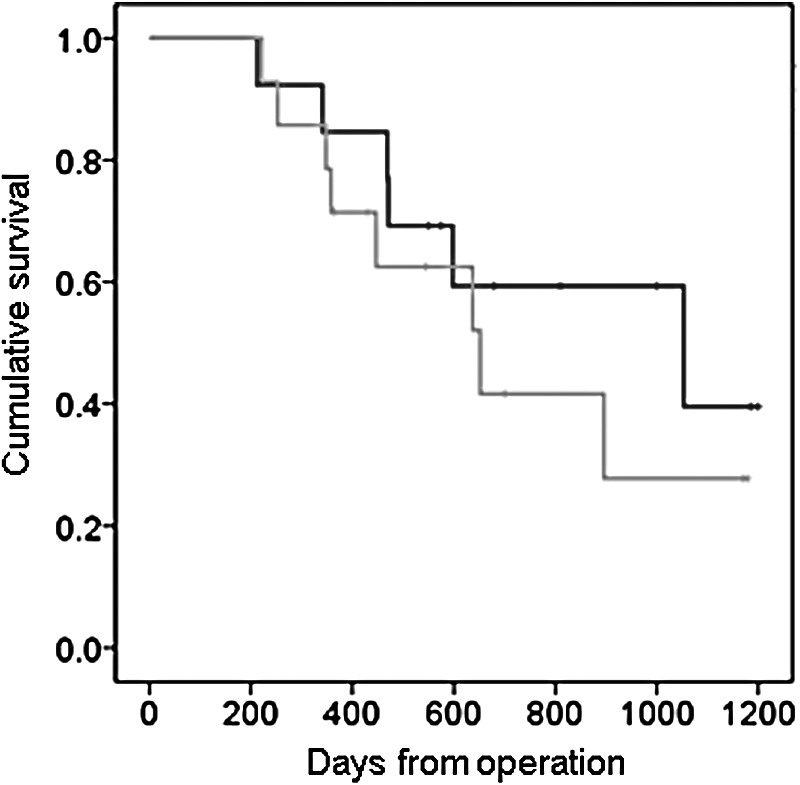
Kaplan–Meier curve of pancreatic adenocarcinoma patients following ODP and LDP. No significant difference in survival rates in patients who were diagnosed with adenocarcinoma following ODP (black) or LDP (gray) was demonstrated. LDP, laparoscopic distal pancreatectomy; ODP, open distal pancreatectomy.
IMPN, intraductal papillary mucinous neoplasia; LDP, laparoscopic distal pancreatectomy; MCN, mucinous cystic neoplasm; NET, neuroendocrine tumor; ODP, open distal pancreatectomy; SPN, solid-pseudopapillary neoplasm.
LDP, laparoscopic distal pancreatectomy; LOS, length of stay; ODP, open distal pancreatectomy; pRBC, packed red blood cells; SD, standard deviation.
Learning curve
The 44-month study period was divided into four periods of 11 months each (periods 1–4). LDP was performed throughout the entire study period. During months 1–11 (period 1), 9 out of 20 pancreatectomies were performed laparoscopically (45%). During periods 2–4, LDP consisted of 47%, 45%, and 54.5% of surgeries, respectively (Table 3). In six patients (three in period 1 and 3 in period 2), a conversion to ODP was indicated. No conversions were performed during periods 3 and 4 (Table 3). The operative time continually decreased, with the most dramatic reduction achieved following the first 22 months. In addition, the LOS gradually decreased from a median of 10 days in study period 1 to 7 days in period 4 (Table 3).
Discussion
Although LDP was shown to be cost-effective, associated with decreased intraoperative blood loss, fewer postoperative complications, early discharge, and comparable oncological outcome,1–7, 9–14 many centers still offer only open approach for DP. 8
We evaluated the safety and effectiveness of LDP compared to ODP in a newly established MIS pancreatic surgery service. Our data suggest that operative time, intraoperative blood loss, as well as postoperative complications, are overall comparable between approaches. One patient in the LDP group died within 30 days, with no perioperative mortalities in the ODP group. Nevertheless, three patients of the ODP group experienced a life-threatening complication (grade IV DC-score; Table 3).
LOS was significantly shorter after LDP. The rate of R0 resection was similarly high in both groups. No conversions to open surgery or pRBC transfusions were necessary following the 17th patient. The operative time and LOS continuously decreased in correlation with the accumulating surgical experience.
Mehrabi et al. 11 performed a systematic review and meta-analysis of LDP versus ODP for benign and malignant lesions, including the results of 29 observational studies, overall analyzing 3701 patients. Five other systematic reviews on this issue were recently published, overall analyzing data from 6961 patients.9,10,20–22 Together these studies reviewed thousands of patients who underwent LDP compared to ODP and provide a solid reference for the current LDP practice. The operative time in these studies ranged from 156 to 383 minutes in LDP with no significant difference from ODP. 11
In accordance with these results, in our series, the mean operative time of LDP was 242.9 ± 81.2 minutes, representing a nonsignificant extension of 21 minutes compared to ODP. In the last study period, the mean operative time of LDP went down by ∼12 minutes below the overall mean operative time of ODP. Previous studies demonstrated that LDP was associated with decreased intraoperative blood loss and requirement of blood transfusions compared to ODP.9–11,22 We were unable to recapitulate these results and demonstrated similar overall pRBC transfusions in both groups. Nevertheless, all patients who required intraoperative pRBC were operated within the first and second study periods, that is, among the 22 patients who underwent LDP during the third and fourth periods of the study, no pRBC were given. This suggests that our overall trend was influenced by the transient effects of early learning curve obstacles.
Although several studies suggested that LDP was associated with decreased postoperative complications, others showed comparable results to ODP, specifically in rates of pancreatic fistula formation.1–7,9–14 Our results stand in good agreement with these data, showing comparable rates of postoperative complications between groups, including the development of pancreatic fistula. LOS is commonly used as an indicator for postoperative patient's recovery. Previous reports demonstrated a markedly variable hospital stay after LDP, ranging from 4 to over 17 days.10,11 This variance can be attributed to cultural differences, healthcare economics, etc. Nonetheless, reduced length of stay was reported in all studies evaluating the benefits of LDP over ODP. Our data demonstrate over 2-day reduction of length of stay over all, with continuous shortening of this period as the study progressed and learning curve was overcome. The change over time is an important indicator that patients were truly recuperating faster, since there was no influence of cultural aspects or surgeon's attitude.
LDP was proved to provide solid oncological results with comparable rates of R0 resection and degree of LN harvest.7,23 We show a very high rate of R0 resections (over 92%) without a significant difference between groups. This was achieved despite greater lesion diameter (over 1.5 cm) in patients who underwent LDP compared to those who underwent ODP. The number of harvested LNs was comparable between groups. This strongly implies that LDP can be widely utilized even for resection of large and bulky tumors. Pancreatic adenocarcinoma was the most common diagnosis in both groups, followed by NET. As was previously shown,7,23 an overall noninferiority in survival of adenocarcinoma patients who underwent LDP was demonstrated.
To our knowledge, two studies evaluated the aspects of learning curve in LDP.15,16 These studies, including 3015 and 3216 patients, demonstrated variable results. Braga et al. 15 reported a significant drop in conversion rate and operative time following the first 10 patients, with no significant difference in operative blood loss, postoperative morbidity rate, and length of stay. On the other hand, Ricci et al. 16 showed decreased operative time after the 17th patient with no differences in conversion rates. No differences in the other parameters mentioned above were demonstrated. Our data show that following the 17th patient, the operative time decreased by more than 35 minutes, no conversions were indicated, no blood transfusion was needed, and the length of stay was shortened by over 2 days. All LDP cases were performed by a single surgeon with established background in other MIS procedures, as well as pancreatic surgery. This indicates that 17 surgeries, as was shown by Ricci et al., 16 are needed for a trained minimally invasive surgeon to complete the learning curve of LDP. Overcoming the learning curve is manifested by decreased operative time, conversion, pRBC transfusions, and length of stay.
Finally, a note about attitude toward laparoscopic surgery needs to be mentioned. Laparoscopic surgery in general has a significant psychological impact on surgeons and the public alike. So called “laparoscopic surgeons” tend to have a strong belief in its benefit, many times with no solid evidence. “Open surgeons” on the other hand, who are not practicing MIS, tend to reject it altogether, even though it is clear that there are some established benefits. Patients nearly always seek for it, as it is mistakenly considered an “operation without operation.” It is clear that the truth can be found only in randomized studies, but these are lacking. One advantage of a versatile service with MIS capabilities is the ability to offer tailored solutions for different clinical scenarios. Also, the very existence of LDP as an option is a strong recruiting force for patients. This, by itself, increases volume and expertise. Last, but not the least, patients satisfaction is becoming more important nowadays. When patients seek MIS and can be offered their desired solution, satisfaction is easier to achieve.
To conclude, LDP is safe and efficient, associated with comparable operative time and rate of postoperative complications, and offers decreased length of postoperative hospital stay. Noninferior short-term oncological outcome is demonstrated. The learning curve of an experienced surgeon consists of ∼17 cases.
Footnotes
Disclosure Statement
No competing financial interests exist.