
Abstract
Abstract
Aims:
To evaluate the technical and clinical outcomes of early laparoscopic radiofrequency (RF) ablation for spontaneously ruptured hepatocellular carcinoma (HCC).
Methods:
From April 2005 to July 2015, ten patients with spontaneously ruptured HCC treated by laparoscopic RF ablation in our hospital were included in the study. The post treatment outcomes were recorded and analyzed.
Results:
The mean size of the 10 HCCs was 6.6 ± 2.2 cm (4.0–10.1 cm) in the maximal dimension. Procedures of laparoscopic RF ablation were performed successfully for all patients. Complete ablation was achieved in 60.0% patients (6/10). Four patients with incompletely ablated tumors received repeated RF ablation to achieve complete ablation. During clinical follow-up, 3 (30.0%) patients developed minor complications and no patient had peritoneal recurrence. As of March 2016 (with a mean follow-up of 32.9 months), 3 patients (30.0%) were alive and 7 (70.0%) died. Of the 10 patients, the 1- and 3-year survival rates were 90.0% and 70.0%, respectively.
Conclusion:
Early laparoscopic RF ablation therapy is an effective treatment measure for spontaneously ruptured HCC in selected patients, which presents an advantage of achieving simultaneous hemostasis, tumor elimination, and rinsing of peritoneal cavity to minimize the risk of peritoneal metastasis.
Introduction
H
Surgeries by laparotomy, such as ligation of the hepatic artery, perihepatic packing, plication, and hepatectomy, used to be the first choices of treatments for managing spontaneously ruptured HCCs from the years of 1960s to 1980s.2–4 Recently, a consensus has been reached that transarterial embolization (TAE) can offer the survival benefit to the patients with HCC. 5 Some experts have recommended two-staged procedures, including TAE for hemostasis followed by a staged hepatectomy to remove HCC, instead of emergent hepatectomy.2–4 However, to the best of our knowledge, no definite recommendation has been reported regarding optimal treatment of spontaneously ruptured HCC.
Radiofrequency (RF) ablation as a safe and effective treatment modality has been widely used for managing HCC, which can be performed using a percutaneous, laparoscopical, or laparotomic approach. This minimally invasive treatment has become the first line of treatment for small HCC in patients with compromised hepatic function reserve or associated medical comorbidity.7,8 Recently, a few reports have described the treatment of ruptured HCC by percutaneous RF ablation to achieve hemostasis in the emergency setting.9–11 However, it is difficult to treat ruptured HCC by percutaneous RF ablation because tumors usually protrude beyond the liver surface. In such situations, a laparoscopic approach would appear to be an appealing alternative. 12 More importantly, percutaneous approach was not a curative method for spontaneously ruptured HCC due to the impossibility of removing tumor tissue and blood clots. Alongside with the blood flow, tumor cells may spread pervasively in the peritoneal cavity, leading to peritoneal metastasis.13,14
In the past decade, we gained extensive experience of using early laparotomic RF ablation to treat spontaneously ruptured HCC. 13 With the increasing use of laparoscopy in the emergency setting, we developed the technique of laparoscopy-aided RF ablation to treat spontaneously ruptured HCC at a tertiary hepatobiliary center between 2005 and 2015. The aim of this study was to evaluate the technical and clinical outcomes of laparoscopic RF ablation for treating spontaneously ruptured HCC.
Materials and Methods
Patients
From April 2005 to July 2015, a total of 435 patients were diagnosed with HCC in Capital Medical University affiliated Beijing Chao-Yang Hospital. The diagnosis of HCC was made according to the American Association for the Study of Liver Disease guidelines. 15 Abdominal contrast material-enhanced multiple phase computed tomography (CT) and/or magnetic resonance imaging (MRI) were used to assess the tumors. HCC rupture was diagnosed based on the manifestations of abrupt abdominal pain, CT imaging features of disrupted peritumoral liver capsule with enhanced fluid collection in the perihepatic area, or bloody ascites confirmed by an abdominal paracentesis.
Of these 435 patients, 16 patients were diagnosed with spontaneous rupture of HCC. Figure 1 illustrates the strategy for the management of spontaneously ruptured HCC. All 16 patients received emergent fluid resuscitation, followed by an extensive examination to evaluate the hemodynamic stability. Hemodynamic instability was defined as systolic blood pressure <90 mmHg despite adequate fluid resuscitation. After primary resuscitation, laparoscopic RF ablation, TAE, surgical intervention, or conservative treatment was selected for treating the patients. Laparoscopic RF ablation was performed in 6 patients with stable hemodynamic status after primary resuscitation. TAE followed by laparoscopic RF ablation was performed for 4 patients with unstable hemodynamic status. Hemostasis procedure using laparotomy was performed in 2 patients because the unstable blood pressure didn't allow for the TAE. Conservative treatment was used in 4 patients due to poor liver function, severe coagulopathy, hepatic encephalopathy, portal venous tumor thrombus (PVTT), and/or poor general conditions.
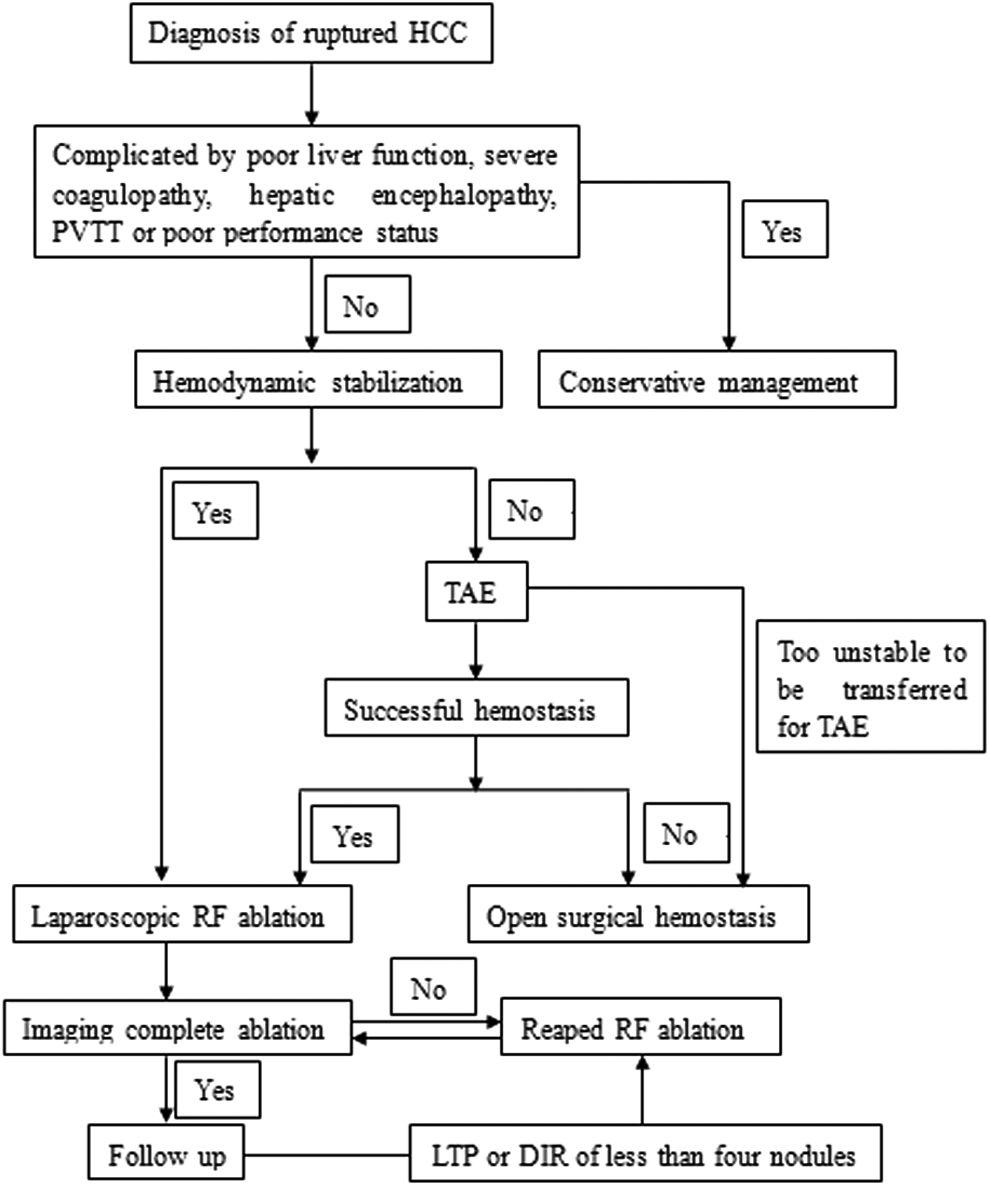
Treatment algorithm for spontaneous rupture of HCC. HCC, hepatocellular carcinoma; IDR, intrahepatic distant recurrence; LTP, local tumor progression; PVTT, portal venous tumor thrombus; RF, radiofrequency; TAE, transcatheter arterial embolization.
Ten patients with spontaneously ruptured HCC treated by laparoscopy-aided ablation were included in the study. This study was approved by the Ethics Committee of Beijing Chao-Yang Hospital affiliated with Capital Medical University, Beijing, China. Written informed consent was waived considering the retrospective nature of this study, and this study was performed in compliance with the Declaration of Helsinki.
TAE procedures
Premedications of analgesia and sedation were performed for all patients before the procedure. Seldinger technology was used to puncture the femoral artery. After celiac and superior mesenteric arteriography, a 5-French catheter (Cook, Bloomington, IN) was used to catheterize the hepatic artery. Tumor feeding arteries were superselectively cannulated using a 3-French microcatheter (Microferret; Cook). Embolizations of the tumor-feeding arteries were performed by infusing suitable amount of iodized oil (Lipiodol; Andre Guerbet, Aulnay-sous-Bois, France) until a complete arterial flow stasis was achieved. Further embolization of tumor feeding arteries with gelatin sponge particles (1–2 mm in diameter; Gelfoam; Upjohn, Kalamazoo, MI) was performed for the patients as well. After embolization, angiography was used to confirm the successful blockade of tumor feeding arteries. Success of hemostasis was defined as cessation of angiographic extravasation, hemodynamic stability, and stabilization of hematocrit without further need of transfusion.
Laparoscopic RF ablation procedure
An experienced hepatobiliary surgeon (W.S.) performed all the procedures. Liver tumor RF ablation was performed using internally cooled cluster electrodes, Cool-tip ACTC 2025 electrodes, and an RF generator (Covidien Healthcare, Dublin, Ireland). Briefly, under general anesthesia, two 10-mm trocars were placed in the abdomen, through which an initial laparoscopic exploration of the peritoneal cavity was performed to check the site of hepatic bleeding. Under ultrasound imaging (US) guidance, a RF probe was introduced into the peritoneal cavity and deployed into the tumor under laparoscopic visualization. After the removal of blood clots around the lesion, the protruded tumor and the bleeding spot were clearly visualized. To avoid worsening tumor bleeding, the RF probe was advanced to target tumor through liver parenchyma. Overlapped ablations were carried out to achieve a complete ablation of tumors. Under the direct visualization of laparoscopy, the ablated tumor was removed in a block-by-block superficial-to-deep manner. Following the tumor removal, RF ablation was used to achieve complete hemostasis and curative effects. Finally, the peritoneal cavity was repeatedly lavaged and rinsed with distilled water containing 1.0 g/L of 5-fluorouracil to prevent peritoneal metastasis. During the procedure, the Pringle maneuver was not used to decrease the heat-sink effect, because of increased risk of postoperative deterioration of hepatic function.
Postoperative evaluation and follow-up
The follow-up protocol includes routine outpatient visit, laboratory tests of a-fetoprotein levels every month, as well as contrast-enhanced CT studies every 2 or 3 months. All patients underwent imaging follow-up of contrast-enhanced multiple phase CT or MRI one month post RF ablation. Complete ablation was defined as absence of nodular or irregular enhancement adjacent to the ablation zone on contrast-enhanced CT or MRI. Incomplete ablation was defined as irregular peripheral-enhanced foci in the ablation zone on the enhanced CT or MRI. In case of incomplete ablation, repeated RF ablation procedures were performed to achieve complete tumor elimination. Local tumor progression (LTP) was defined as the presence of nodular enhancement at the peripheral zone of the ablated area on hepatic arterial phase CT images followed by a fast washout on the portal venous phase images. Intrahepatic distant recurrence (IDR) was defined as the lesion with similar imaging characteristics, but not in the domain of the original ablated zone. 16
In case of LTP or IDR, supplemental imaging examinations such as thoracic and/or abdominal CT or bone scintigraphy were performed to screen potential tumor metastasis. Once LTP or IDR with less than four nodules was confirmed, patients were hospitalized as soon as possible to undergo repeated RF ablation. Patients with five or more IDR nodules have the indications of being treated with transarterial chemoembolization. When extrahepatic metastasis was confirmed, the patient was referred to receive treatment of sorafenib administration.
Statistical analysis
All data were recorded as mean ± standard deviation.
Results
RF ablation procedure
Among 10 patients, 8 (80.0%) were male and 2 (20.0%) female, with a mean age of 55.8 ± 6.4 years (47–66 years). All patients were hepatitis B virus carriers with complication of liver cirrhosis. Hepatic function of 2 patients was evaluated as Child-Pugh class A and 8 as class B. The demographic features of patients are illustrated in Table 1.
HCC, hepatocellular carcinoma.
The tumor features were evaluated by imaging examinations. The mean size of the HCCs was 6.6 ± 2.2 cm (4.0–10.1 cm) in the maximal dimension. Eight patients had single HCC lesion and 2 patients had two and three HCC lesions.
Laparoscopic RF ablation was performed as the primary treatment for 6 patients immediately after primary resuscitation. Four patients received staged laparoscopic RF ablation 3–5 days after TAE. TAE treatments were performed in 4 patients successfully.
Complications
Laparoscopic RF ablation treatment was performed successfully for all patients without any technical difficulties. The mean ablation time was 1.8 ± 0.3 hours (1.4–2.4 hours) and the mean blood loss was 242.0 ± 122.3 mL (100–470 mL) without need of transfusion.
Complications were seen in 3 (30.0%) patients, including right shoulder pain, fever, pleural effusion, jaundice, and hemoglobinuria. All complications were evaluated as grade I according to Dindo–Clavien classification system. 17 No perioperative mortality occurred. No severe complications were seen in patients, including liver failure, thoracic hemorrhage, abdominal hemorrhage, destructive biliary damages, adjacent viscera perforation, or liver abscess.
Complete ablation
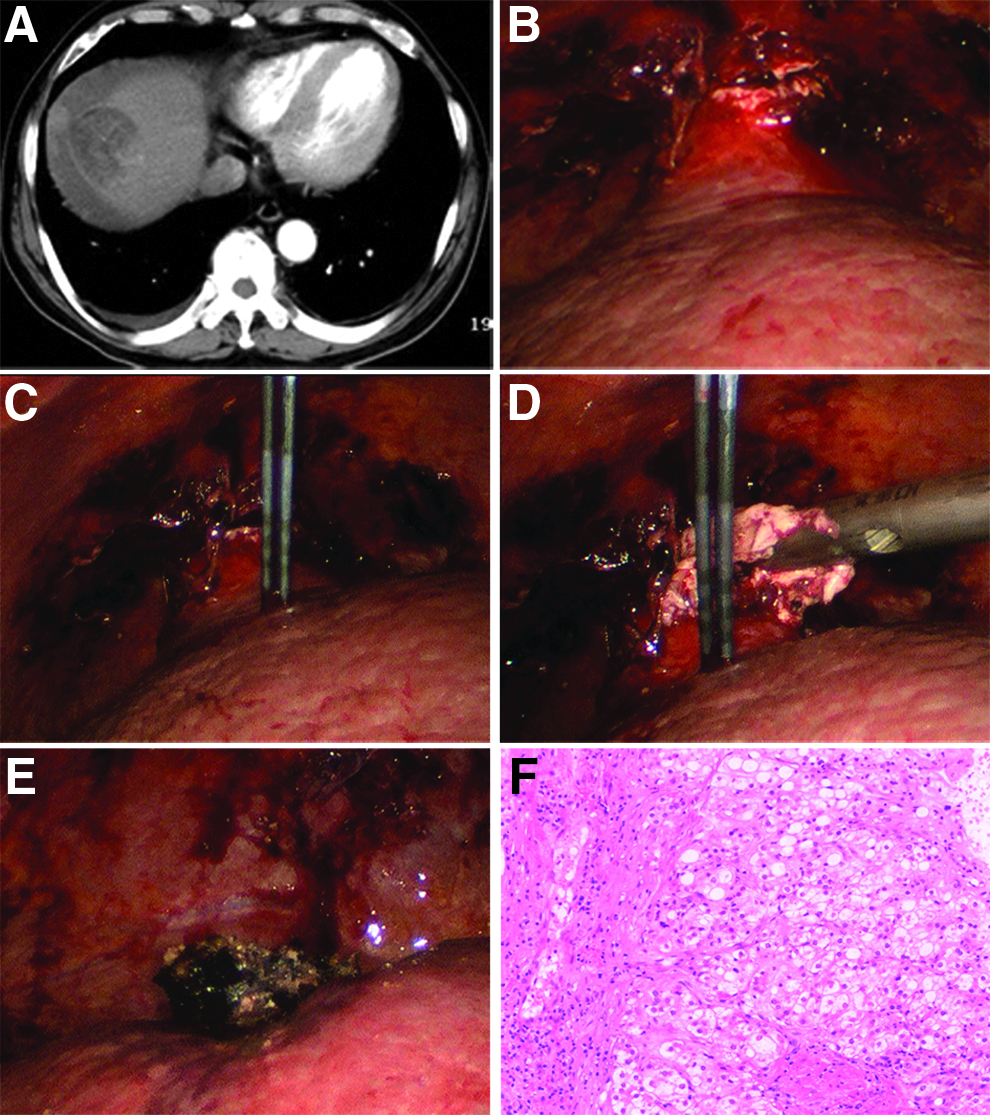
Complete ablation was achieved in 6 of 10 patients (60%) after one session of RF ablation (Fig. 2). Four patients who presented as incomplete ablation received repeated RF ablation 1 month post one session with successful complete ablation of tumors. The remnant tumor tissues of the four HCCs were situated in the deep locations of liver after laparoscopic RF ablation. Therefore, the repeated RF ablation was performed under CT-guided percutaneous approach (Fig. 3). The mean hospitalization time for patients with ruptured HCC was 14.5 ± 3.2 days (10–19 days).

Recurrence and survival
During follow-up, the LTP rate was 20.0% (2/10) and IDR was found in 3/10 patients (30.0%). Extrahepatic metastasis rate was 20.0% (2/10). No patient had peritoneal metastasis.
The patients with LTP or IDR received RF ablation. One patient who had extrahepatic metastasis received the treatment of sorafenib and the one refused conservative symptomatic treatment. The total number of RF ablation sessions of each patient is listed in Table 2.
HCC, hepatocellular carcinoma; RF, radiofrequency; TAE, transcatheter arterial embolization; LTP, local tumor progression; IDR, intrahepatic distant recurrence.
As of March 2016 (with a mean follow-up of 32.9 months), 3 patients (30.0%) were alive and 7 (70.0%) died. Patient deaths were caused by IDR in 2 patients, extrahepatic metastases in 2 patients, PVTT in 2 patients, and liver failure in one. Of the 10 patients, the 1- and 3-year overall survival rates were 90.0% and 70.0%, respectively. Three patients survived actually beyond 3 years (Table 2). Kaplan–Meier survival curve of 10 patients is listed in Figure 4.
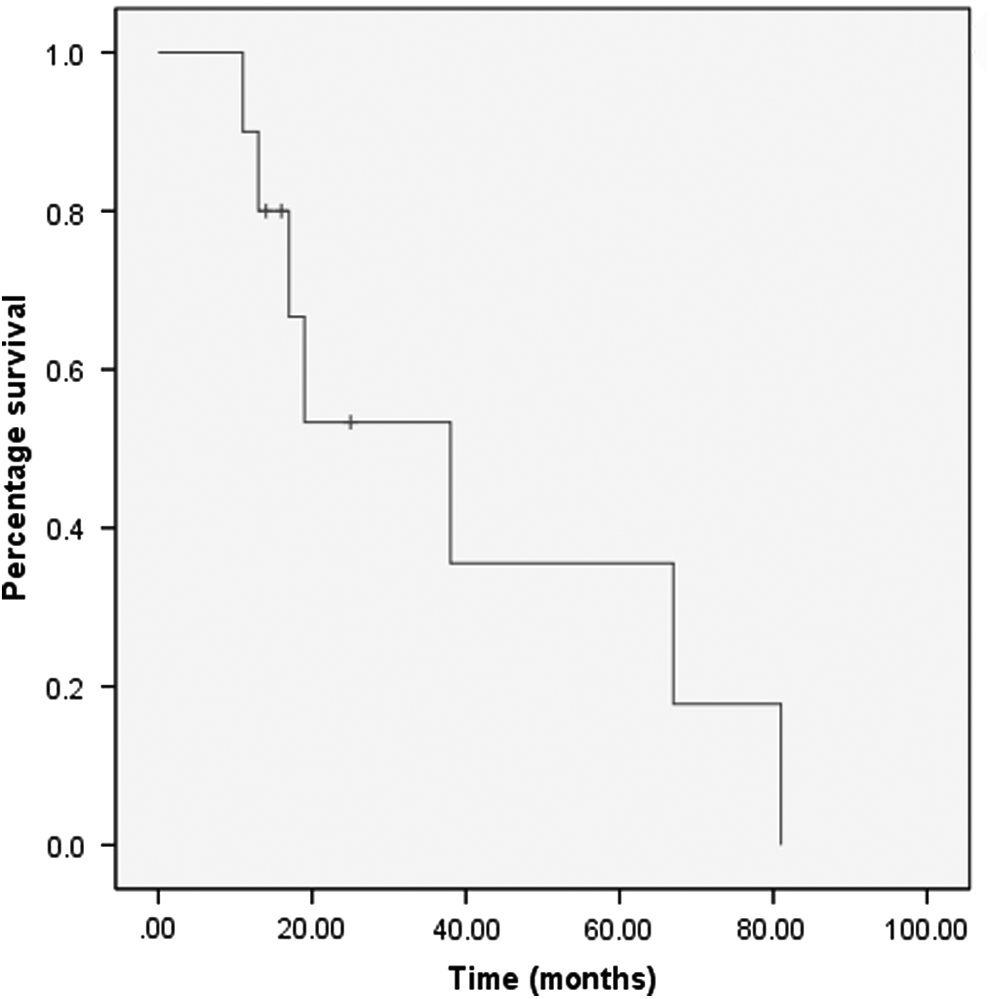
Kaplan–Meier survival curve of the patients with spontaneous rupture of HCC, starting on the day of the first radiofrequency procedure. HCC, hepatocellular carcinoma.
Discussion
This study evaluated the technical and clinical outcomes of patients with spontaneously ruptured HCC treated by laparoscopic RF ablation. Our data showed the relatively high safety and technical effectiveness, without severe complications, suggesting that acute laparoscopic RF ablation therapy may be considered as an alternative treatment of spontaneously ruptured HCC in the patients with stable hemodynamics (Fig. 2). However, for patients with spontaneously ruptured HCCs and unstable hemodynamics, due to massive amount of hemorrhage, RF ablation may not be an insufficient approach to effectively stop active bleeding. In this scenario, a combination treatment of TAE followed by laparoscopy-aided RF ablation may be more safe and effective (Fig. 3).
Spontaneous rupture of HCC is a life-threatening condition. It is necessary to take effective measures to stop the bleeding and simultaneously treat the tumor as early as possible.2–6 TAE has been recommended as the first choice for emergency treatment of ruptured HCC. Although TAE can be used to stop the bleeding from a ruptured HCC in a majority of patients, it is not effective to control the tumor itself in some cases.2–5 Recurrence of tumor rupture-induced bleeding and hepatic failure may appear in some TAE-treated patients. 2 Moreover, TAE cannot eliminate the risk of HCC rupture-induced intraperitoneal metastasis.2–4 For patients treated by TAE alone, the long-term survival rate remains low. 5 Hepatectomy seems to be an ideal treatment for achieving both hemostasis and curative effects.2–4 However, the majority of patients with ruptured HCC cannot withstand surgery even in a stable condition, because of hepatic insufficiency or portal hypertension.
RF ablation is a minimally invasive therapy for patients with early stage HCC, which can offer similar outcomes compared with surgical resection in selected patients. RFA can be performed percutaneously, laparoscopically, or during open surgery. In recent years, a few studies have reported that percutaneous RF ablation has been used as an emergency procedure for hemostasis of ruptured HCC.9–11 However, the effect of RFA using a percutaneous approach to treat spontaneously ruptured HCC is still unclear. Ruptured HCC usually protrudes beyond the liver surface, which was regarded as one of the contraindications of percutaneous approach, because of the great risk of bleeding, bile leakage, or visceral organ injury. Livraghi et al. 12 suggested that subcapsular tumors should be treated by the open or laparoscopic approach for direct visualization of the organs, ensuring a complete separation of tumor. An obvious disadvantage of percutaneous approach lies in the fact that the tumor tissue and hematocele in the peritoneal cavity cannot be removed, as the same with TAE.
Our study shows that acute laparoscopic RF ablation is an effective technique for achieving a complete hemostasis and offering a benefit of maximizing tumor elimination in selected patients with ruptured HCC. Hepatectomy is not appropriate for all of the 10 cases according to operability criteria. 18 With the aid of laparoscopy, RF ablation can not only control hemorrhaging effectively but also remove the tumor in a minimally invasive manner without massive blood loss. After tumor tissue removal, the margins can be involuted to confine the remaining lesion into depression, which facilitate the application of repeated RF ablation. Recently, laparoscopy had been increasingly applied to abdominal trauma as a diagnostic or therapeutic role, which could significantly reduce the risk of incidence of postoperative complications and perioperative mortality rate. 19 Despite the many advantages, the application of laparoscopy to abdominal trauma has strict indications and contraindications. The laparoscopy was mostly applied to hemodynamic stable patients who sustained suspected abdominal trauma. Contraindications to laparoscopy included hemodynamical instability or those who combined with shock or serious cardiopulmonary dysfunction. 19 Based on the literature and our experience, an algorithm for potential applications for laparoscopic RF ablation in spontaneously ruptured HCC has been proposed (Fig. 1). As was shown in our study, 6 patients with stable hemodynamic status were treated successfully by laparoscopic RF ablation alone. Moreover, 4 patients with unstable hemodynamic status received TAE therapy before laparoscopic RF ablation to block the tumor blood supply and maintain hemodynamic stability to reduce the risk of laparoscopy.
In addition, patients with previously ablated HCC seem to be at higher risk of developing new rapidly growing nodules in comparison with cirrhotic patients without history of HCC. 20 Close follow-up is consequently mandatory, because RF ablation can be performed repeatedly in steps to ultimately eradicate the tumors for the patients with subablated or recurrent tumors.13,21 Furthermore, in our study, none of the 10 patients had peritoneal recurrence during the period of clinical follow-up, which indicates that under the direct visualization of laparoscopy, we can lavage and rinse the peritoneal cavity to remove the blood clot, decreasing the likelihood of peritoneal metastasis and improve survival.13,14
The major limitations of our study include its retrospective nature, lack of control group, and the limited sample of patients. Our study indicates the advantage of using laparoscopic RF ablation to treat spontaneously ruptured HCC. A well-designed clinical trial enrolling a large cohort of patients with control groups may be warranted to further confirm the clinical significance of this technique to maximize the benefit of HCC patients.
In conclusion, early laparoscopic RF ablation therapy is an effective treatment measure for spontaneously ruptured HCC in selected patients, which presents an advantage of achieving simultaneous hemostasis, tumor elimination, and rinsing of peritoneal cavity to minimize the risk of peritoneal metastasis.
Footnotes
Acknowledgments
Supported by Clinical-Basic Medicine Cooperation Fund of Capital Medical University (1300171711) and the Program for Medical Key Discipline of Shijingshan District (20130001).
Author Contributions
Conceived and designed the experiments: J.G. and W.S. Performed the experiments: J.G., Y.Z., Q.Z., J.K., S.K., X.D., S.W., and J.Z. Contributed reagents/materials/analysis tools: J.G., Y.Z., Q.Z., J.K., S.K., X.D., S.W., and J.Z. Wrote the article: J.G. and W.S.
Disclosure Statement
No competing financial interests exist.