
Abstract
Abstract
Background:
Various methods of reconstruction after laparoscopic distal gastrectomy (LDG) have been developed and reported. In open gastrectomy, gastroduodenostomy or gastroenterostomy is often performed with the hand-sewn technique. Therefore, hand-sewn anastomosis was performed through a small incision in LDG. The aim of this study was to evaluate the feasibility and safety of LDG with hand-sewn anastomosis.
Methods:
Between June 2009 and December 2015, we assessed 263 consecutive patients who underwent LDG in our institution. In all patients, the reconstruction procedures were performed extracorporeally with the hand-sewn technique. The clinical characteristics, surgical outcomes, and operation cost related to anastomosis were evaluated and compared with the other methods.
Results:
The average operation time was 157.5 minutes, and average blood loss was 38.8 mL. The types of reconstruction were Billroth I, 95 cases (36.1%); Billroth II, 165 cases (62.7%); and Roux-en-Y, 3 cases (1.1%). The overall incidence of postoperative complications (Clavien–Dindo classification≧Grade II) was 8.0%. Anastomotic leakage was observed in 1 patient (0.4%) and anastomotic bleeding and anastomotic stenosis in 2 patients each (0.8%). There was no postoperative mortality. The cost of the absorbable threads used in anastomosis is less than the cost of a linear or circular stapler, which is often used in intracorporeal anastomosis.
Conclusion:
This procedure is similar to conventional open surgery, and it is feasible, safe, and cost-effective. In addition, in an institution that plans to introduce LDG, the use of our method during the introductory phase of LDG has many advantages.
Introduction
S
Various techniques have been developed, and their outcomes have been reported.4–8 The methods can be classified into two main types: extracorporeal hand-sewn anastomosis and intracorporeal stapled anastomosis using a linear or circular stapler. The determination of the method and technique for reconstruction after LDG depends on the surgeon and institution because both procedures have both advantages and disadvantages.
In conventional open gastrectomy, gastroduodenostomy or gastroenterostomy is often performed with the hand-sewn technique. In June 2009, we introduced LDG with extracorporeal hand-sewn anastomosis through a minilaparotomy incision in the same manner as conventional open surgery. Although some authors have reported that extracorporeal anastomosis is performed in a limited working space with restricted vision, and it is difficult to perform, especially in patients with obesity, a large body, or a small remnant stomach,9,10 we make all types of attempts to create adequate operative fields and easily and safely perform reconstruction.
The aim of the present study is to introduce our surgical technique and evaluate the short-term outcomes. In addition, we compared the cost required for anastomosis of our method and the other methods.
Materials and Methods
This study was a single-center, retrospective study that was approved by the Ethics Review Board of Ogaki Municipal Hospital. The subject provided informed consent, and patient anonymity was preserved.
Between June 2009 and December 2015, we performed LDG with extracorporeal hand-sewn anastomosis in 263 consecutive patients (173 men and 90 women) at Ogaki Municipal Hospital. The inclusion criteria were patients younger than 80 years old who had an Eastern Cooperative Oncology Group performance status of 0 or 1, histologically proven gastric adenocarcinoma located at the lower or middle third of the stomach, and a clinical depth of tumor invasion confined to the submucosal layer with no lymph node metastasis (or recently, owing to the improved skill, clinical depth of tumor invasion confined to the subserosal layer, and lymph node metastasis confined to the perigastric nodes) as determined by endoscopy and abdominal computed tomography (CT) according to the Japanese classification of gastric carcinoma, 2nd English edition. 11 The exclusion criteria were patients with unstable angina or myocardial infarction, severe respiratory disease, and a history of upper abdominal surgery. We retrospectively reviewed the prospectively collected data by electronic medical records from 263 consecutive patients. Data obtained for each patient included the following: sex, age, body mass index, comorbidities, surgical procedure, operation time, blood loss, number of harvested lymph nodes, postoperative complications, postoperative hospital stay, postoperative oncologic outcome, depth of tumor invasion, lymph node metastasis, and clinical stage according to the UICC staging and the WHO classification of tumors. Data for each patient are recorded from day of surgery up to now. The postoperative complications, including all major and minor complications, were graded according to the Clavien–Dindo classification. 12
All patients were monitored postoperatively by physical examination, blood tests every 3–6 months for the first 5 years, and thereafter by abdominal ultrasonography, CT, chest radiography, and gastroscopy at least twice each year.
Surgical techniques
The initial trocar port was introduced below the umbilical incision. After the establishment of pneumoperitoneum at 10 mmHg, a flexible laparoscope (OLYMPUS MEDICAL SYSTEMS CORP. Tokyo, Japan) was introduced through the initial port. The other five ports and a Nathanson liver retractor for liver-lift with fixation by OCTOPUS® (Yufu, Tokyo, Japan) were inserted under laparoscopic vision. The surgeon stood on the patient's right side, and the assistant stood on the patient's left side. The scopist was placed between the patient's legs. An aspirating tube was introduced through the 5-mm port on the left side of the umbilicus, which was manipulated by the right hand of the scopist to generate an auxiliary expanded field of view as well as lavage and aspiration to control bleeding (Fig. 1).
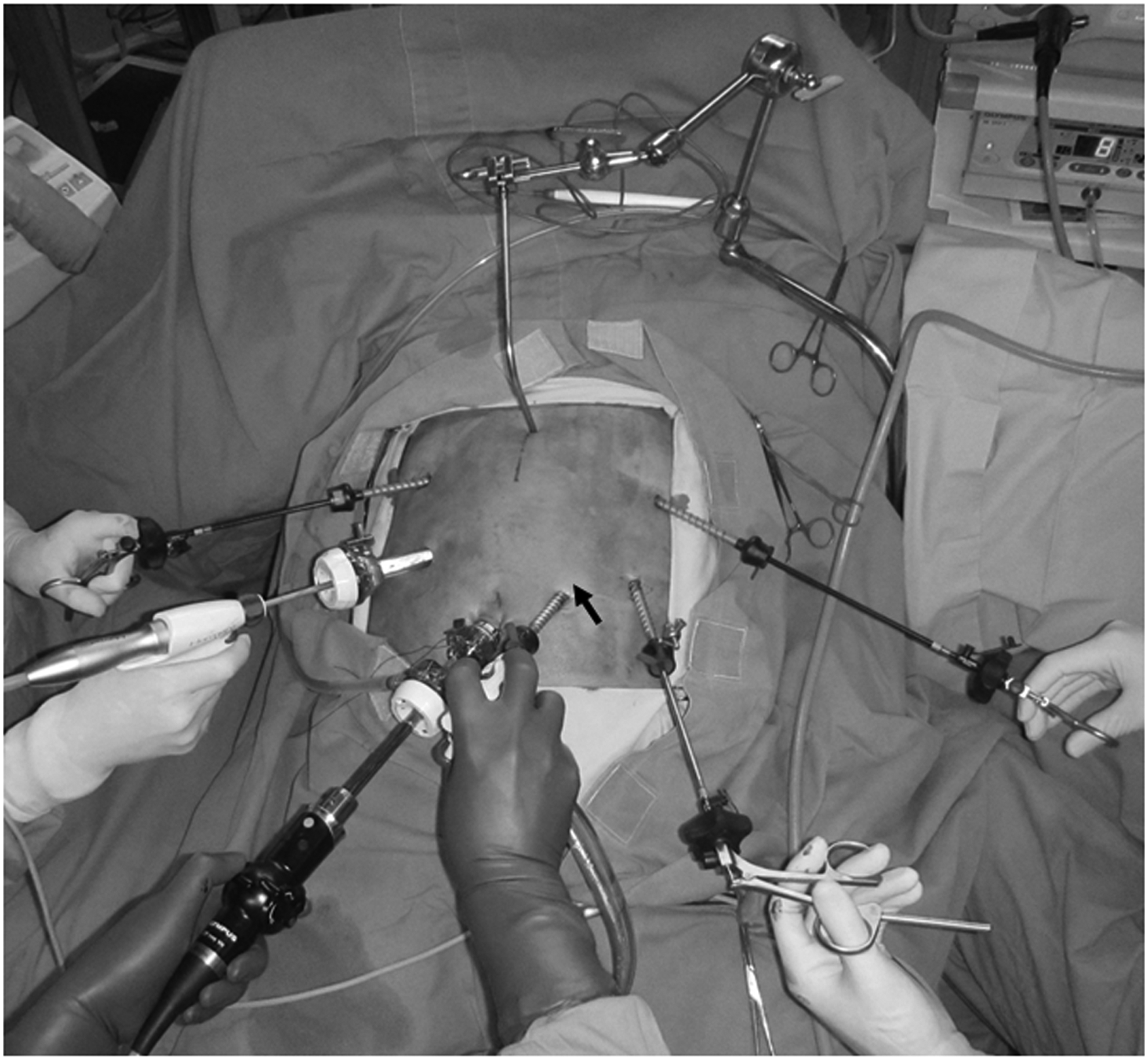
Trocar placement. Infraumbilical incision sites (12 mm), for the scope; right upper port (5 mm), for the instruments in the left hand of the operator; left upper port (5 mm), for the instruments in the right hand of the assistant; right lower port (12 mm), for the instruments in the right hand of the operator; and left lower port (5 mm), for the instruments in the left hand of the assistant. An aspirating tube was introduced through the 5-mm port on the right side of umbilicus port (5 mm) (arrow) for the aspirating tube in the right hand of the scopist.
In principle, we performed laparoscopic lymph node dissection in almost the same manner as conventional open gastrectomy. To mobilize the stomach and dissect the lymph nodes, laparoscopic coagulation shears (Ethicon Endo-Surgery, Inc., Cincinnati, OH) were used. Duodenal resection below the pyloric ring was performed using a linear stapler (60 mm) (Ethicon Endo-Surgery, Inc., Cincinnati, OH). All reconstruction procedures were performed extracorporeally with the hand-sewn technique. The Billroth I (B-I) reconstruction was the first choice, if possible; however, the Billroth II (B-II) and the Roux-en-Y (R-Y) reconstructions were performed when the B-I reconstruction could not be used, especially in patients with obesity or a small remnant stomach. When the reconstruction was performed with the B-II or R-Y, a Nelaton catheter was placed into the jejunum ∼20 cm distal to the Treitz ligament for delivery in an antecolic manner via minilaparotomy.
After removing the Nathanson liver retractor, a 5–7 cm midline incision was made in the upper abdomen (Fig. 2a) and opened to allow for the insertion of a wound protector. The stomach was extracted through this minilaparotomy incision and the tumor location was detected by palpation. The resection line was determined with the identification of the cancer lesion. The proximal resection margin was determined, and two clamps were applied to the greater curvature of the stomach at a length of ∼4 cm. After the gastric wall was incised between the two clamps using scissors, a linear stapler (100 mm) (Covidien, Mansfield, MA) was used to divide the distal stomach and close the lesser curvature (Fig. 2b). A reinforcement suture was added to the linear stapler line. In the B-I reconstruction, we grasped the gastric stump and duodenal stump with angle clamps. In B-II or R-Y reconstruction, we grasped the gastric stump and jejunum with angle clamps. An adequate and stable operative field around the stumps of the intestinal tracts was provided with the fixation of these angle clamps by OCTOPUS® (Yufu, Tokyo, Japan) (Fig. 2c). Gambee anastomosis was performed using 3-0 VICRYL (Ethicon; Johnson & Johnson, New Brunswick, NJ) with an interrupted suture in the same manner as for open surgery (Fig. 2d). In all operations, we routinely inserted one intra-abdominal drain during surgery, and each wound was closed.

Reconstruction procedures.
Results
In this study, 263 patients were enrolled. Three patients were lost to follow-up within 1 year after surgery at the discretion of the patient. The follow-up period was 6–77 months (average, 33 months). The clinical characteristics and operative data of the patients who underwent LDG are summarized in Tables 1 and 2, respectively. The 3 patients more than 81 years old were included. Although the inclusion criteria in our institution were patients less than 80 years old, these patients hoped strongly that they could undergo laparoscopic surgery. The mean operation time was 157.5 min (range, 93–368), and the mean estimated blood loss was 38.8 mL (range, 1–690). The mean number of harvested lymph nodes was 26.6 (range, 3–77). The B-I reconstruction was performed in 95 (36.1%) patients. The B-II and R-Y methods were performed in the remaining 165 (62.7%) and 3 (1.2%) patients. In one case with a right inguinal hernia, transabdominal preperitoneal repair was simultaneously performed.
Data are shown as number of patients (%).
BMI, body mass index; COPD, chronic obstructive pulmonary disease.
Data are shown as number of patients (%).
The postoperative outcomes are shown in Table 3. The overall incidence of postoperative complications (≧Grade II) was 8.0%. Reoperations were required in 5 patients (1.9%). The causes of reoperation were pancreatic fistula and secondary pseudoaneurysm of the gastroduodenal artery, intra-abdominal bleeding, port-site herniation, afferent loop obstruction, and anastomotic stenosis. Anastomotic stenosis was observed in 2 patients. A patient was treated by decompression with a gastric tube without endoscopic balloon dilatation. However, the other patient was not treated conservatively, and total gastrectomy included gastrojejunostomy after B-II reconstruction was required. The patient had improvement of symptoms and was discharged 15 days after surgery. A patient with anastomotic bleeding was treated by endoscopic hemostatic therapy on one occasion. A patient with anastomotic leakage was treated by percutaneous drainage. There was no postoperative mortality. The mean postoperative hospital stay was 14.8 days.
Data are shown as number of patients (%). Grade is according to the Clavien–Dindo classification.
The histological findings are shown in Table 4. Early gastric cancer (T1) was confirmed pathologically in 76.8% of the patients. 17.8% (47 out of 263 patients) of the patients had nodal involvement. 83.3% (219 out of 263 patients) of the patients had Stage I disease. One patient had abdominal dissemination during LDG and received chemotherapy after the operation. The patient was alive for ∼3 years after surgery.
Data are shown as number of patients.
UICC, UICC TNM classification, 7th edition.
With respect to the operation-related costs, the cost of the absorbable threads used in anastomosis was ∼3000 JRY, which was cheaper than the linear or circular stapler that is often used in intracorporeal anastomosis (Table 5).
JLSSG, Japanese Laparoscopic Surgery Study Group; JCOG, Japan Clinical Oncology Group; LS, linear stapler; CS, circular stapler; HS, hand-sewn; LDG, laparoscopic distal gastrectomy.
Discussion
We described here a method of extracorporeal hand-sewn anastomosis through a minilaparotomy in LDG. This study demonstrated that anastomotic leakage was observed in 1 patient (0.4%), and anastomotic bleeding and anastomotic stenosis in 2 patients each (0.8%). Our method is similar to conventional open surgery and was feasible, safe, and cost-effective.
In general, laparoscopic gastrectomy can be divided into laparoscopy-assisted and totally laparoscopic techniques. With laparoscopy-assisted gastrectomy, lymph node dissection is performed laparoscopically, but transection of the stomach and anastomosis are performed extracorporeally through a minilaparotomy. Compared with the laparoscopy-assisted surgery, with the totally laparoscopic procedure, the anastomosis is also performed intracorporeally using staples and appears to have several advantages, including a shorter incision, less pain, and earlier recovery.9,13 Extracorporeal anastomosis is conducted in a limited working space with restricted vision, making it a difficult procedure, especially for obese patients with thick abdominal walls or patients with a small remnant stomach.9,10 This might have resulted in complications from anastomosis, such as minor leakage due to excessive traction of the organs toward the abdominal wall. 4
We designed a procedure to perform the reconstruction easily and safely, even in obese patients. If the assistant holds the forceps by grasping the gastric and duodenal stumps or jejunum during anastomosis, the operative field sometimes becomes unstable because of the fatigue of the assistant. The fixation of the forceps grasping the gastric and duodenal stumps or jejunum by OCTOPUS® provided good and stable operative fields for anastomosis. Both assistants’ hands were free, and the assistants could help the operator to anastomose delicately. In this environment, we performed extracorporeal hand-sewn anastomosis.
Herein, we summarized the surgical outcomes of various methods of anastomosis in LDG (Table 5). Kanaya et al.5,14 first reported on delta-shaped anastomosis (Delta), an intracorporeal procedure completed with a linear stapler alone. They demonstrated that Delta offered the advantages of being virtually unaffected by the patient's physical constitution in securing the visual field and was less subject to variation in the surgeon's suturing skill level. In addition, it was a simple, easy, and safe method. Kim et al. 8 described the method of an intracorporeal procedure using a circular stapler. None of the patients experienced complications, such as leakage or stenosis. In extracorporeal anastomosis, we summarized four reports, including our study. The length of minilaparotomy incision is almost the same. Kitano et al. 15 reported the data obtained from 16 surgical departments that are members of the Japanese Laparoscopic Surgery Study Group. Katai et al. 16 described a multi-institutional phase II trial conducted by the Gastric Cancer Surgical Study Group of the Japan Clinical Oncology Group (JCOG 0703). Although the reconstruction approach and surgical method following resection were not specified in their reports, the rates of anastomotic leakage and stenosis were, respectively, 2.1% and 3.0% in Kitano et al., 15 and 1.1% and 0.6% in Katai et al. 16 Hand-sewn anastomosis was also reported by Lee et al. 13 They performed the procedure with a two-layer anastomosis technique that was unlike our Gambee method. The rates of anastomotic leakage and stenosis were 6.8% and 2.7%, respectively, for the initial experience with LAG. Subsequently, they introduced the intracorporeal stapler technique. Seung Jong Oh et al. 17 reported that the median time for performing the anastomosis with the stapling technique was shorter than with the hand-sewn technique. However, our present study indicates that our method resulted in the shortest operation time and lower blood loss. In addition, although 1 patient had anastomotic bleeding, the rate of 0.4% for anastomotic leakage had the lowest incidence. The rate of 0.8% for anastomotic stenosis had the acceptable incidence in the extracorporeal methods listed above and was almost same as those of the intracorporeal methods. One possible reason for the low proportion of anastomosis-related complications might be our procedures, which are conducted in the same manner as conventional open surgery and are performed under adequate, stable operative fields.
In the recent study,10,18 there were no differences in the intracorporeal or extracorporeal anastomosis for the operation time, estimated blood loss, incidence of conversions to open surgery, and operative complications. In addition, the patient symptoms during the postoperative follow-up, including BMI, were similar between the groups. The meta-analysis also revealed no significant differences between the two methods, indicating that extracorporeal anastomoses following LDG were feasible and safe.
With respect to the reconstruction after distal gastrectomy, many surgeons in Japan have typically performed either the B-I or B-II reconstructions.
Recently, R-Y reconstruction has been increasingly used. The B-I reconstruction is advantageous in that it only requires a single anastomosis and retains physiologic food passage. However, the disadvantages of the B-I reconstruction after LDG include a higher risk of anastomotic leakage and difficulty securing a satisfactory visual field under a minilaparotomy due to the limited mobility of the duodenal stump.13,15 In contrast, the R-Y reconstruction offers the advantages of being virtually unaffected by the patient's physical constitution when securing the visual field. The R-Y reconstruction is reported to be associated with a lower incidence of anastomotic leakage and a favorable postoperative QOL. 6 The current study showed that the rate of the B-II reconstruction was higher (62.7%) than the other reconstructions. Zhao et al. 19 also reported that the rate of the B-II reconstruction after laparoscopic assisted distal gastrectomy was higher (77.5%) than B-I (22.5%). They performed reconstruction through the 4–6 cm median superior incision as in our procedure. With our method, we can perform the R-Y reconstruction. However, this procedure is laborious, requiring two anastomoses. The B-II reconstruction, on the contrary, is advantageous in that it only requires a single anastomosis. Therefore, we selected the B-II reconstruction. We did not experience any serious complications, including bile reflux, reflux esophagitis or gastritis, or residual stomach cancer. In the future, if patients with the B-II reconstruction suffer from these symptoms, we could use the R-Y reconstruction instead of B-II reconstruction.
In laparoscopic surgery, the higher cost of the operation, including the equipment cost, remains a major challenge that needs to be solved. 9 A benefit of our method is its cost-effectiveness. We used 3-0 VICRYL sutures and did not require a stapler for the anastomosis. However, the Delta-shaped anastomosis reported by Kanaya et al.5,14 requires three linear staplers, and anastomosis with a circular stapler by Kim et al. 8 requires one circular stapler and one linear stapler. As a result, the cost of our method is much lower than the intracorporeal anastomosis with a stapler method (Table 4). Some researchers have insisted that the increased intraoperative costs associated with equipment costs are compensated for by a better perioperative hospital course of patients, who often have shorter hospital stays, fewer complications, less need for narcotics, and less need for ward nursing. 20 Unfortunately, we could not compare the other methods in relation to total hospital charges associated with the hospital stays and other complications.
The current study has several limitations. First, the analysis was based on retrospective data collection at a single institution and there was a bias in the selection of the patients. Therefore, it is unclear whether the present results are applicable to all patients. Another limitation is that in comparison with the other anastomosis method, we compared only equipment costs without total hospital costs. However, we believe that our method contributes to the decrease in the hospital costs.
An additional advantage of our procedure is its optimization for laparoscopic surgery with incorporation of the concepts of a conventional open gastroduodenostomy. Surgeons who have previously performed the open version of this anastomosis can adopt our method without difficulty.
Conclusions
Although intracorporeal anastomosis using staples after LDG is gradually increased, our procedure is similar to conventional open surgery, and it is feasible, safe, and cost-effective. In addition, in an institution that plans to introduce LDG, the use of our method during the introductory phase of LDG has many advantages.
Footnotes
Disclosure Statement
No competing financial interests exist.