
Abstract
Abstract
Background:
Liver resection (LR) for hepatocellular carcinoma (HCC) is the best alternative option for increasing the survival of many patients with intermediate or advanced stages of the Barcelona Clinic Liver Cancer staging classification. Mini-invasive approach may play a positive role in treating a tumor rising almost exclusively in a diseased liver.
Methods:
A prospectively collected database was retrospectively reviewed for 167 consecutive patients who underwent LR between 1999 and 2015.
Results:
A total of 38 LRs were performed from 1999 to 2009 (Period I), and 129 between 2010 and 2015 (Period II). Laparoscopic procedures increased from 5.3% to 38.1%. Not undergoing laparoscopic LR increased length of stay, and Clavien Grade II or worse complications. Ninety-day mortality decreased from 5.2% to 0%, and morbidity did not differ significantly, despite the fact that the most complex patients were in Period II.
Conclusions:
Mini-invasive approaches allow to safely expand limits of LR for HCC; in particular, laparoscopic approach favors surgical option even in more complex patients without increase the risk of posthepatic liver failure or other postsurgical complications.
Introduction
L
Over the last two decades, Makuuchi criteria, Barcelona clinic liver cancer (BCLC) staging classification, Child-Pugh classification, Model for End-Stage Liver Disease (MELD) score, and many other tools have been implemented to propose a decision-making algorithm for HCC on liver disease. 3 Although many of these are simple and widely accepted, the BCLC has resulted historically as the most reliable prognostic system for predicting outcome in Western countries. 4
This system, which is endorsed by both the European Association for the Study of the Liver (EASL) and by the American Association of the Study of Liver Diseases (AASLD), recommends LR only for patients at the first stage, who are those in Child-Pugh class A without portal hypertension or major vascular invasion. 5 However, many centers perform LR for intermediate and advanced stages of the BCLC, claiming better results compared with alternative palliative options, such as transarterial chemoembolization (TACE).6,7
With resectability as the best, the effort in the surgical community is toward the expansion of LR limits, without increasing the incidence of posthepatectomy liver long-term outcome parameter failure (PHLF) or the risk of performing futile surgery due to very early recurrence.
For liver failure following hepatectomy in 2011, the International Study Group of Liver Surgery summarized the published nonstandardized definitions of PHLF and defined it as an impairment of liver function on or after postoperative day (POD) 5, which is graded according to its impact on clinical management. 8 PHLF has a variable clinical relevance in the oncologic setting because its incidence differs according to the underlying parenchyma and to the extension of the resection.9,10
As a result, 90-day mortality secondary to PHLF can reach 8%, and PHLF is responsible for more than 60% of deaths after extended LR.11,12
In light of these facts, we postulated that the possibility of performing mini-invasive liver surgery on chronic liver patients could potentially contribute to the development of LR for HCC.
To explore this hypothesis, we reviewed our approach to LR for HCC over a 16-year period, in a single center, considering all the changes and improvements in surgical techniques and perioperative management that have taken place in that period. In addition to the obvious improvements over time in the perioperative management, we focused our attention on new surgical trends in mini-invasive surgery and hepatic parenchymal-sparing surgery. The primary goals of this single-center retrospective study were to report the incidence and characteristics of PHLF in our population of patients resected for HCC and document the changing trends in our center regarding the treatment of HCC.
Materials and Methods
Study population
A total of 167 consecutive LRs for HCC were performed at IRCCS-ISMETT (Istituto Mediterraneo per i Trapianti e Terapie ad alta specializzazione) in Palermo, Italy, between July, 1999 and June, 2015. This study and analysis of our database were undertaken after approval from ISMETT's Joint Institutional Review Board. Informed consent was obtained from all living patients at the undertaking of the study.
The following demographic characteristics and surgical variables were retrospectively extracted and analyzed from a prospectively collected database, exploring the medical records of the patients included in the study: age, gender, BCLC (according to EASL/AASLD guidelines) and Child-Pugh scores, postoperative length of stay, onset of PHLF, occurrence of any complication or a Clavien–Dindo Grade II or worse complication, 13 packed red blood cell or red blood cell (PRBC/RBC) transfusion, using a water-cooled, high-density monopolar device (TissueLink Medical, Inc., Dover, NH) or Kellyclasia as the primary surgical technique, major or minor resection according to the Couinaud classification, site of primary tumor, comorbidities such as diabetes or glucose intolerance, heart disease, respiratory diseases, POD 1 through 5 laboratory values for alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transferase (GGT), alkaline phosphatase (ALP), international normalized ratio (INR), albumin (ALB), total bilirubin, and platelet count.
The Couinaud classification was used for defining LRs, so a major LR was defined as involving three or more liver segments, such as right or left hepatectomy, extended or not, and minor LRs, including left lobectomy, as bisegmentectomy, segmentectomy, and wedge resection. 14
Outcome parameters
The following outcome parameters were considered in this study: PHLF, postoperative length of stay, occurrence of any complications within 90 days of surgery, Clavien Grade II or worse complication, and need for intraoperative PRBC/RBC transfusion. The PHLF classification was defined as a grading-system classification, as recently described elsewhere by the IGSLS:
1. Grade A: the patient experiences a postoperative deterioration of liver function with no change in clinical management; 2. Grade B: the patient requires clinical management with noninvasive treatments, such as the administration of fresh-frozen plasma, ALB, and/or daily diuretics; 3. Grade C: the patient requires clinical management with invasive treatments, such as hemodialysis and/or intubation. We used this definition to divide the patients into two groups: those who had developed PHLF and those who had not.
Postoperative length of stay was measured as the time, in days, from the date of surgery to discharge. To standardize reporting, complications were graded using the Clavien–Dindo classification. In this classification system, Grade 0 describes a case that does not deviate from the normal postoperative course.
1. Grade I complications are those that do not require pharmacological treatment, or surgical, endoscopic, or radiologic interventions;
2. Grade II complications are those requiring pharmacological treatment other than antiemetics, antipyretics, analgesics, diuretics, or electrolytes;
3. Grade III complications are those requiring surgical, endoscopic, or radiologic intervention. This category is further divided into Grade IIIa complications, for which interventions do not require general anesthesia, and Grade IIIb complications, for which interventions require general anesthesia;
4. Grade IV complications are life threatening and can be divided into Grade IVa, single organ dysfunction, and Grade IVb, multiorgan dysfunction. Grade V describes the death of the patient. Patients with at least one Grade II, IIIa, IIIb, IVa, IVb, or V were classified as having experienced a Grade II or worse complication.
Statistical analysis
Categorical variables are presented as numbers and percentages, and groups were compared using the Pearson χ2 test or Fisher's exact test. Quantitative variables are expressed as mean ± standard deviation (SD), and groups were compared using the Mann–Whitney U-test or t-test.
Uni- and multivariate logistic regression analysis were used to identify independent risk factors among those variables that were identified as statistically significant in group comparison tests: odds ratios (OR) with the corresponding 95% confidence interval (95% CI) were calculated.
Statistical tests were considered significant when the corresponding P value was ≤5%. Data handling and analyses were done with STATA 13.1.
Results
Over the study periods, 38 LRs were performed from 1999 to 2009 (Period I), and 129 between 2010 and 2015 (Period II). Even after an increase in the number of procedures, no differences between the two groups were found in terms of length of hospital stay (12.7 ± 12 days versus 9.1 ± 10.9 days, two-sample t-test with equal variances, P = .21), intraoperative blood loss (23.6 ± 66 cc versus 34.5 ± 82 cc, 1-sided variance ratio test, P = .16), and patients who received blood transfusions (4/38, 10.5% versus 10/127, 7.7%, Fisher exact test, P = .56). Ninety-day mortality decreased from 5.2% to 0%, with an overall 1-year disease-free survival rate of 79.2%; 90-day morbidity did not differ significantly, despite the fact that the most complex patients were in Period II.
Postoperative complications of Clavien–Dindo Grade ≤2 were documented in 85.8% of patients, and complications with a score ≥2 in 14.2% of patients. No correlation in terms of postoperative morbidity was found between patients who underwent LR during Period I (84.2% of patients developed complications ≥2) and patients in Period II (86.4% of patients developed complications ≥2) (Fisher's exact test, P = .79). No significant discrepancies were found in terms of PHLF (Fisher's exact test, P = .45): in Period I, Grade A was documented in 23.7% of patients, Grade B in 7.9%, and Grade C in only one case (1.7%). During Period II, PHLF Grade A was documented in 24.8% of patients and grade B in 8.3%. No patients experienced Grade C PHLF in Period II (Table 1).
Related to the significant statistical tests, when the corresponding P value was inferior or equal to 5%.
BCLC, Barcelona clinic liver cancer; MELD, model for end-stage liver disease; PHLF, posthepatectomy liver failure; SD, standard deviation.
Patient-related factors
A total of 167 patients were included in this study; 145/167 (86.8%) were affected with cirrhosis, while 22/167 (13.2%) had normal liver parenchyma, with no significant differences between the two periods of time. The age of patients who underwent LT during Period II was significantly higher (mean ± SD: 67 ± 9.7 years) than those whose surgery was performed in Period I (mean ± SD: 59.3 ± 16 years, P = .01). The proportion of patients with American Society of Anesthesiologists (ASA) score 3 and 4, who underwent surgery during Period II (68.2%, 88/129 and 18.7%, 24/129, respectively), and was not significantly higher than those undergoing surgery in Period I (75%, 28/38 and 8.1%, 3/38, respectively, P = .82) (Table 1).
The most common comorbidities in our patient population were hypertension (117/167, 70.1%), respiratory diseases (74/167, 44.3%), diabetes or glucose intolerance (51/167, 30.5%), a history of smoking (48/167, 28.7%), heart valve disease (14/167, 8.3%), and atrial fibrillation (14/167, 8.3%). However, there were no significant correlations between these comorbities, and the severity of ASA score, and a worse short-term surgical outcome or the increased incidence of PHLF (data not shown). Significant differences were found in the incidence of respiratory and cardiac diseases in patients treated in the two different periods (Fisher's exact test, P = .045 and .041 for Period I and Period II, respectively). Patients with incomplete data (24/167, 14.3%) were excluded from analysis of the trends of ALT, AST, GGT, ALP, ALB, INR, platelet count, and total bilirubin levels from perioperative day 0 through 5. Using the two-sample t-test with unequal variances, associations between total bilirubin levels were found between the two study groups, Period I and II, according to the increasing severity of liver disease over time. Patients who underwent surgery in Period II had significantly higher preoperative values of total bilirubin (0.7 ± 0.4 mg/dL versus 0.5 ± 0.3 mg/dL, P = .03) than those in Period I (Table 2). There was no significant difference in postoperative trends in ALT, AST, GGT, ALP, ALB, INR, or platelet count; these laboratory values appeared to share similar downward trends from POD 1 through 5 in both time periods.
Related to the significant statistical tests, when the corresponding P value was inferior or equal to 5%.
ALB, albumin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; INR, international normalized ratio; POD, postoperative day; SD, standard deviation.
Liver-related factors
Roughly 70% of the patients were hepatitis C carriers. The MELD score remained constant over time (6.6 ± 0.9–6.8 ± 1.5, Mann–Whitney test, P = .73). Otherwise, the pattern of preoperative severity of underlying liver disease significantly changed over the study period: 15.3% of patients were preoperatively classified as Child-Pugh score B7 and the majority of those were treated with LR in Period II (21 cases, 95.5%) (Fisher's exact test, P = .03). With regard to the BCLC staging classification, patients were considered BCLC-B stage when multinodular asymptomatic tumors with no invasive pattern were detected. In detail, 88 (52.8%) and 25 (15.1%) patients were within early (A) and intermediate (B) stages of disease. Of those treated in Period II, 65.5% were stage A and 87.5% were stage B (Fisher's exact test, P = .004). The presence of intermediate stage disease was correlated with a greater chance of experiencing a Clavien–Dindo Grade II or worse complication (Fisher's exact test, P = .02). Conversely, it is important to note here that no correlation was found between the severities of liver disease in cirrhotic patients and the incidence of PHLF (Fisher's exact test, P = .99) (Table 1).
Focusing on Period II, a higher value of total bilirubin on POD 1 was associated with a higher incidence of PHLF (1.8 ± 1.2 mg/dL versus 1.0 ± 0.5 mg/dL, Mann–Whitney test, P < .001), with an almost five-fold increased risk of experiencing PHLF (OR, 4.5, 95% CI, 1.2–16.6, P = .002) (Table 3). Otherwise, this laboratory marker did not evidence any correlation with experiencing a Clavien Grade II or worse complication (Mann–Whitney test, P = .42). Intermediate-stage-disease patients undergoing LR was the only liver-related factor associated with an almost five-fold increased risk of experiencing a Clavien–Dindo Grade II or worse complication (OR, 4.5, 95% CI, 1.2–16.6, P = .002), (Table 4).
Related to the significant statistical tests, when the corresponding P value was inferior or equal to 5%.
BCLC, Barcelona clinic liver cancer; PHLF, posthepatectomy liver failure; POD, postoperative day; SD, standard deviation.
Related to the significant statistical tests, when the corresponding P value was inferior or equal to 5%.
BCLC, Barcelona clinic liver cancer; SD, standard deviation.
Surgery-related factors
The mean operating room time was 241.7 ± 121 minutes and decreased from 289.8 ± 138 to 226.4 ± 111 from Period I to Period II (Mann–Whitney test, P = .01). With regard to the type of LR, the percentage of major hepatectomies fell from 25% to 10.9% (Fisher's exact test, P = .05) from Period I to Period II. The most relevant decrease was in right extended hepatectomies, from 13.1% (5/38) to 0.7% (1/129) (Fisher's exact test, P = .004). Conversely, the percentage of minimally invasive procedures increased from 5.3% (2/38) in Period I to 38.1% (49/129) in Period II, (Fisher's exact test, P = .01).
In parallel with fewer major hepatectomies performed over time, the 90-day mortality rate for all cases decreased from 5.2% (2/38) in Period I to zero mortality in Period II, (Fisher's exact test, P = .01). The percentage of resections combined with ablation treatments increased: in Period I, 9 patients (25%) underwent a major LR, and in 1 case LR was associated with a radiofrequency thermal ablation (RFTA) for another HCC nodule. In Period II, 10.9% (14/129) of cases were treated with a major LR (Fisher's exact test, P = .05), and in 2 patients the LR was followed by microwave thermal ablation (MWTA) for intrahepatic distant nodules of HCC. No thermal ablation treatments were performed in association with minor LR during Period I, in contrast to minor LR associated with MWTA and RFTA in 5 and 2 cases, respectively, in Period II. Patients in our study had a wide array of primary tumor liver sites, with no significant difference in the two time periods.
In Period II, undergoing a major LR was correlated with a greater chance of suffering any PHLF (Fisher's exact test, P = .004). Minimally invasive surgery (Fisher's exact test, P = .02) and the length of surgical procedures (two-sample t-test with unequal variances, P = .01) were significantly associated with experiencing any PHLF after LR for HCC, but lacked significance on multivariate analysis (Table 3). Of the 8/14 patients (57.1%) who underwent a major resection, none suffered any complications or experienced a Clavien–Dindo Grade I complication, compared with 91.6% (105/115) of patients who underwent a minor resection (Fisher's exact test, P = .06). Of those patients who underwent minimally invasive procedures (40% versus 6.7%, Fisher's exact test, P = .02) or experienced reduced length of operative time (285.3 ± 113 minutes versus 217.1 ± 109 minutes, two-sample t-test with equal variances, P = .03), or minor hospital stay (18.4 ± 21.1 days versus 7.7 ± 7.5 days, Mann–Whitney test, P = .0001), there was a significant inverse association with Clavien–Dindo Grade II or worse complication. Otherwise, none of the surgical factors were associated on multivariate analysis with severe postoperative morbidity, except for patients undergoing a right hepatectomy (9/127, 7.3%), with an almost nine-fold increased risk of experiencing a Clavien–Dindo Grade II or worse complication (OR, 8.7, 95% CI, 1.6–46.7, P = .011) (Table 4).
Tumoral hepatic histology
Preoperative HCC diagnosis was made with dynamic contrast-enhanced magnetic resonance imaging and/or noninvasive 4-phase multidetector computed tomography scan (hypervascular in the arterial phase with washout in the delayed phases) on nodules larger than 1 cm in diameter. Biopsies were done for uncertain diagnosis with suspicion of high-grade dysplastic nodules. The mean number of resected segments decreased from 2.1 ± 1.2 in Period I to 1.5 ± 0.8 in Period II (two-sample t-test with unequal variances, P = .01). Although tumor grading was not correlated with an increased number of LR cases in the two periods (Fisher's exact test, P = .21), when stratified by tumor stage, relevant differences were found in those with T1 and T3-T4 tumors in Periods I and II, (Fisher exact test, P = .009) (Table 1).
In Period II, none of the histologic tumor characteristics on univariate and multivariate analyses evidenced increased risks of experiencing any PHLF (Table 3). In addition, patients with T1 tumors (82/129, 63.6%) experienced excellent outcomes, with a Clavien–Dindo Grade II or worse complication in only 6.9% (9/129) of cases, (Fisher's exact test, P = .03), although none of the histological factors were relevant on multivariate analysis (Table 4).
Discussion
Treatment of HCC must be multidisciplinary and patient oriented, and take into account the patient's clinical stage, liver function reserve, and performance status. Over the last 5 years at our institute, we have performed an increasing number of LRs, with an opposite trend in transarterial embolization and TACE and LT (Fig. 1).
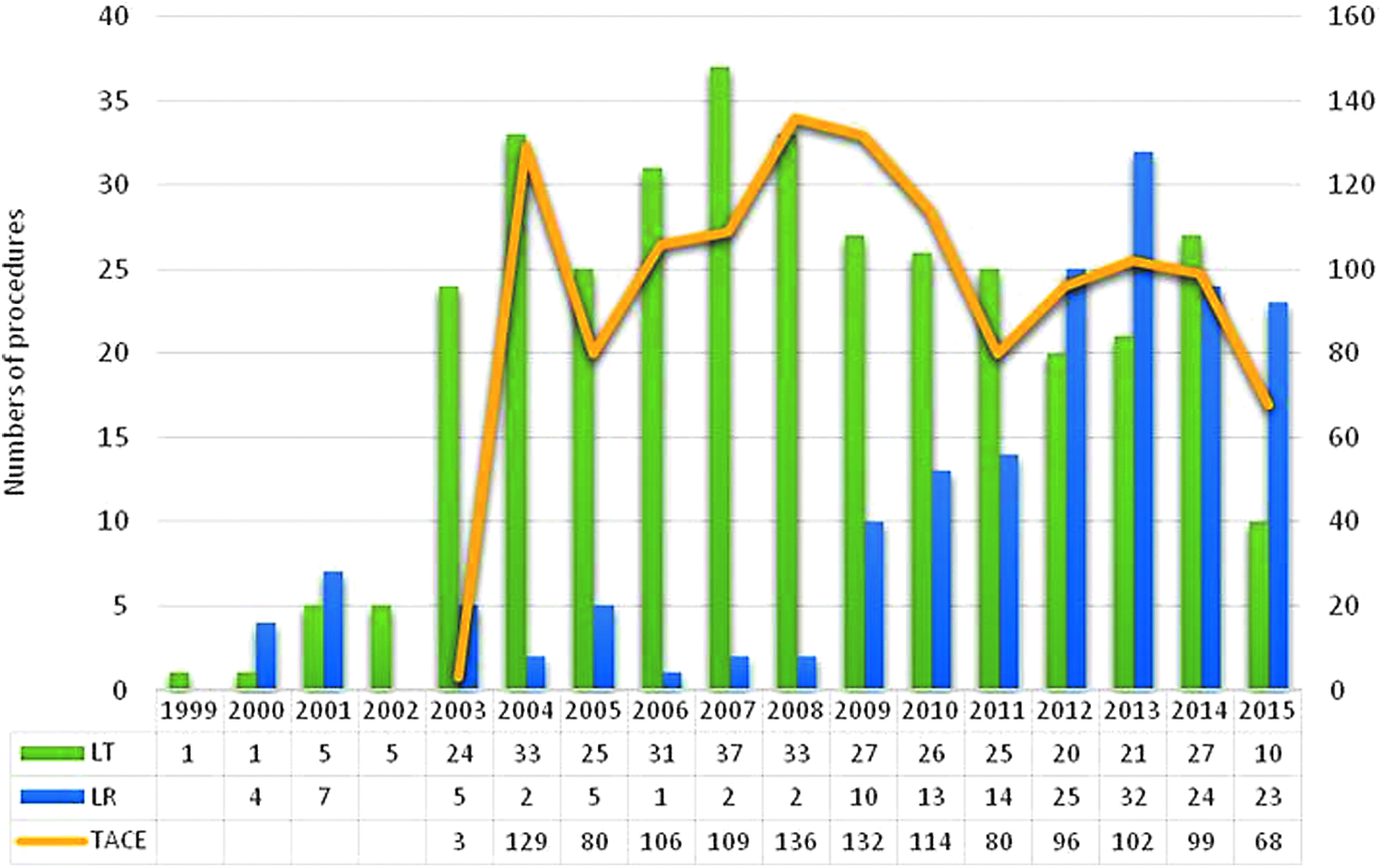
Single-center experience in hepatocellular carcinoma (HCC) treatments. From 1999 to 2015, we performed 169 liver resections (LR) and 350 consecutive liver transplantations (LT), of which 20 were split LT and 35 were living donor LT with right hemilivers (segments 5–8). During the same period of time, a total of 1254 transarterial embolization (TAE) and transarterial chemoembolization (TACE) procedures were performed in cirrhotic patients with HCC not suitable for surgical resection and percutaneous ablation therapy.
Our institute has a multidisciplinary program in which all the therapeutic options for HCC are present, and looking at our data, it appears clear that some strategies have changed over time. Due to chronic organ shortage, and to a better understanding of the donor/recipient match, in the setting of deceased liver allocation and LT benefit, in Italy we now perform much less LT for HCC. 15
Moreover, despite the fact that molecular genotyping seems to have great potential for individualizing the best recipients of LT, 16 this is far from actual clinical practice; so the role of LR is growing both as a downstaging bridging therapy for HCC, and an alternative to LT due to lack of grafts. On the other hand, living-related liver transplantation has some important potential in the setting of HCC therapy, but still faces a host of problems in the Western world, so the number of cases performed per year is very low. This might explain why more Western centers are moving away from strict BCLC indications for LR and are now performing more LR for intermediate-stage patients than in the past. 17
There is now enough scientific evidence that parenchymal-sparing surgery carries fewer postoperative complications and, furthermore, the possibility of performing mini-invasive liver surgery on chronic liver patients has contributed tremendously to the development of LR for HCC. 12 Restricting surgery to small or no incision results not only in better cosmetic effects but also, above all, in a much less-complex postoperative period, with less pain, and a greater chance of faster recovery for the patients. Minimally invasive surgery benefits patients with portal hypertension, who are more prone to bleeding and ascitic decompensation.
“Modern LR,” based on cautious attention to technical details, with less or no use of blood transfusions, and improvements in perioperative management have now reached an important level of success, with overall low morbidity and mortality in the published series. 18 Over time, our clinical experience prompted us to “arbitrarily” consider sicker patients for a laparoscopic approach or minimally invasive parenchymal-sparing resection, even in the presence of large nodules, accepting a tumor-free surgical resection margin of 1 mm.19,20
Our data reflect how surgical treatment of HCC has changed over time in the Western world. This study is subject to a number of limitations, the most important of which is its retrospective design, with all of the inherent limitations of retrospective studies. The relatively small group of patients also limited the number of variables that could be simultaneously investigated with multiple linear regression analysis. In addition, this was a single-center study and was done in a small, highly specialized, and dedicated transplant hospital, with experience in LR and LT, which means that the associations we found are likely not generalizable to larger, more heterogeneous settings. It is our hope that future, prospective, observational, and preferably multicenter studies will shed further light on the associations that we found in our group of patients. However, our experience is a successful example of how to expand indications for LR in HCC patients. The mean age of patients was higher in Period II, and patients in the Child-Pugh B class and intermediate BCLC stage underwent resection with no increase in PHLF or other postsurgical complications. As a result, more patients were offered LR in a time of persistent graft shortage, and benefited from an increased life span and quality of life.
Conclusions
Expanding the limits of LR for HCC, through mini-invasive approach, to include more complex patients, such as the elderly and those within the Child-Pugh B class and intermediate BCLC stage, does not increase the risk of posthepatic liver failure or other postsurgical complications.
Footnotes
Acknowledgment
The authors would like to thank Warren Blumberg for his help in editing this article.
Authorship
S.G.: Design of study, acquisition of data, interpretation of data, preparation of the article, and final approval of article. A.T.: Acquisition of data, interpretation of data, and preparation of the article. D.P.: Acquisition of data, interpretation of data, and preparation of the article. A.G.: Acquisition and interpretation of data. R.L.: Acquisition and interpretation of data. T.L.: Acquisition and interpretation of data. F.T.: Statistical analysis and interpretation of data. A.L. Design of study and interpretation of data. G.V.: Design of study and interpretation of data. B.G.: Design of study and interpretation of data.
Disclosure Statement
This article has not been published, and is not under consideration elsewhere. We declare that all authors are in agreement on the content of the article and have no potential conflicts of interest. We have nothing to disclose regarding sources of support in the form of grants, equipment, and/or pharmaceuticals. The authors of this article have no conflicts of interest, including employment, consultancies, stock ownership, honoraria, paid expert testimony, or patent applications/registrations, to disclose. The article has been “spell-checked” and “grammar-checked”. References are in the correct format for this journal. All references mentioned in the Reference list are cited in the text, and vice versa. Permission has been obtained for use of copyrighted material from other sources (including the Web). Color Figure is clearly marked as being intended for color reproduction.