
Abstract
Abstract
Introduction:
Laparoscopic liver resection (LLR) has several problems, such as technical complexity and patient and tumor factors. A difficulty scoring system to preoperatively evaluate the difficulty of LLR was established at the second International Consensus Conference on Laparoscopic Liver Resection. The aim of this study was to explore the clinical usefulness of the difficulty scoring system for LLR.
Patients and Methods:
From January 2010 to June 2015, the records of 78 patients who had undergone LLR were retrospectively reviewed. The patients' data were used to assign a difficulty score, and the correlations between scores and surgical outcomes were investigated.
Results:
The mean surgical time was 256 minutes, and the mean blood loss was 168 mL. The difficulty score significantly correlated with surgical time and blood loss, but not with morbidity and postoperative hospital stay. Multivariate analysis showed that the difficulty score was an independent predictor of prolonged surgical time.
Conclusions:
The difficulty score was found to be an effective predictor of surgical time for LLR.
Introduction
M
LLR has gradually been accepted as a treatment option for hepatic malignancies. The Louisville statement in 2008 described LLR as a safe and effective approach for the management of liver disease in the hands of trained surgeons with experience in hepatobiliary and laparoscopic surgery. 17 However, there has been no index to define the degree of surgical difficulty of LLR. Therefore, a detailed difficulty index is required to introduce LLR to surgeons and to help them progress to more advanced LLR. A novel difficulty scoring system to preoperatively evaluate the difficulty of LLR was established at the second International Consensus Conference on Laparoscopic Liver Resection in 2014 at Iwate. Ban et al. reported a tool for guidance on the difficulty of LLR called the difficulty scoring system. 18 This system was developed to assess the difficulty of various laparoscopic hepatectomy procedures performed in a daily clinical setting. The system assesses tumor location, extent of liver resection, tumor size, proximity to major vessels, and liver function.
The aim of this study was to validate the difficulty scoring system for LLR by assessing the correlations between difficulty scores and surgical outcomes in a single institution.
Patients and Methods
Study design
From January 2010 to June 2015, 78 patients underwent LLR at the Department of Gastroenterological and Pediatric Surgery, Oita University Faculty of Medicine, Oita, Japan. The patients' data were retrospectively assigned a score according to the difficulty scoring system parameters, and a total score was obtained for each case.
We investigated the correlation between the difficulty score and surgical outcomes. Surgical time was defined as the time from skin incision to skin closure. Furthermore, we analyzed independent indicators of surgical outcomes using univariate and multivariate analyses. All complications were classified according to the Clavien–Dindo classification 19 and postoperative morbidity index. 20 Anatomical resection of the liver was defined as the procedure in which the Glissonian pedicle was divided at the root bifurcation and all of the parenchyma related to the pedicle was resected. The nomenclature from the Brisbane 2000 guideline for liver anatomy and resection was used to describe the extent of the hepatic resection. 21
Difficulty scoring system
In 2014, Ban et al. reported a novel scoring system for LLR. 18 This scoring system was defined as the extent of liver resection, tumor location, tumor size, liver function, and tumor proximity to major vessels. Surgical difficulty was assessed using an index of 1–10 with the following divisions: 1–3 low difficulty, 4–6 intermediate difficulty, and 7–10 high difficulty. This scoring system was proposed to predict difficulty of various LLRs preoperatively.
Statistical analyses
All variables were expressed as mean ± standard deviation for continuous data and as a number with percentages for categorical data. Statistical analysis was performed using Student's t-test for continuous variables and chi-squared test for categorical variables. The correlations between continuous variables and scores were investigated using Spearman's rank correlation. Multivariate logistic regression analyses were performed to identify predictors associated with prolonged surgical time. In these analyses, the cutoff points for surgical time and blood loss were determined using receiver operating characteristic (ROC) curve analysis. Statistical significance was set at P < .05. All statistical analyses were performed using SPSS for Windows software (IBM-SPSS, Inc., Chicago, IL).
Results
Patient characteristics and surgical outcomes
The mean age was 70 ± 10 years (range 40–86). Of 78 patients, 47 were males (60.3%) and 31 were females (39.7%). The majority of patients (74 patients, 94.9%) underwent LLR for hepatic malignancy, and 4 (5.1%) patients underwent LLR for a benign indication. Laparoscopic repeat liver resection was performed in 11 (14.1%) patients and anatomical liver resection was performed in 18 (23.1%) patients. The mean surgical time was 256 ± 124 minutes, and the mean blood loss was 168 ± 260 mL. The patients' characteristics and surgical outcomes are shown in Table 1. Postoperative complications occurred in 13 (16.7%) patients and the mean postoperative hospital stay was 13.7 days.
Alb, albumin; ALT, alanine transaminase; AST, aspartate transaminase; BMI, body–mass index; ICG, indocyanine green; PT, prothrombin time; T-bil, total bilirubin.
The difficulty score did not correlate with morbidity and the length of postoperative hospital stay (data not shown).
Correlation between difficulty score and surgical outcomes
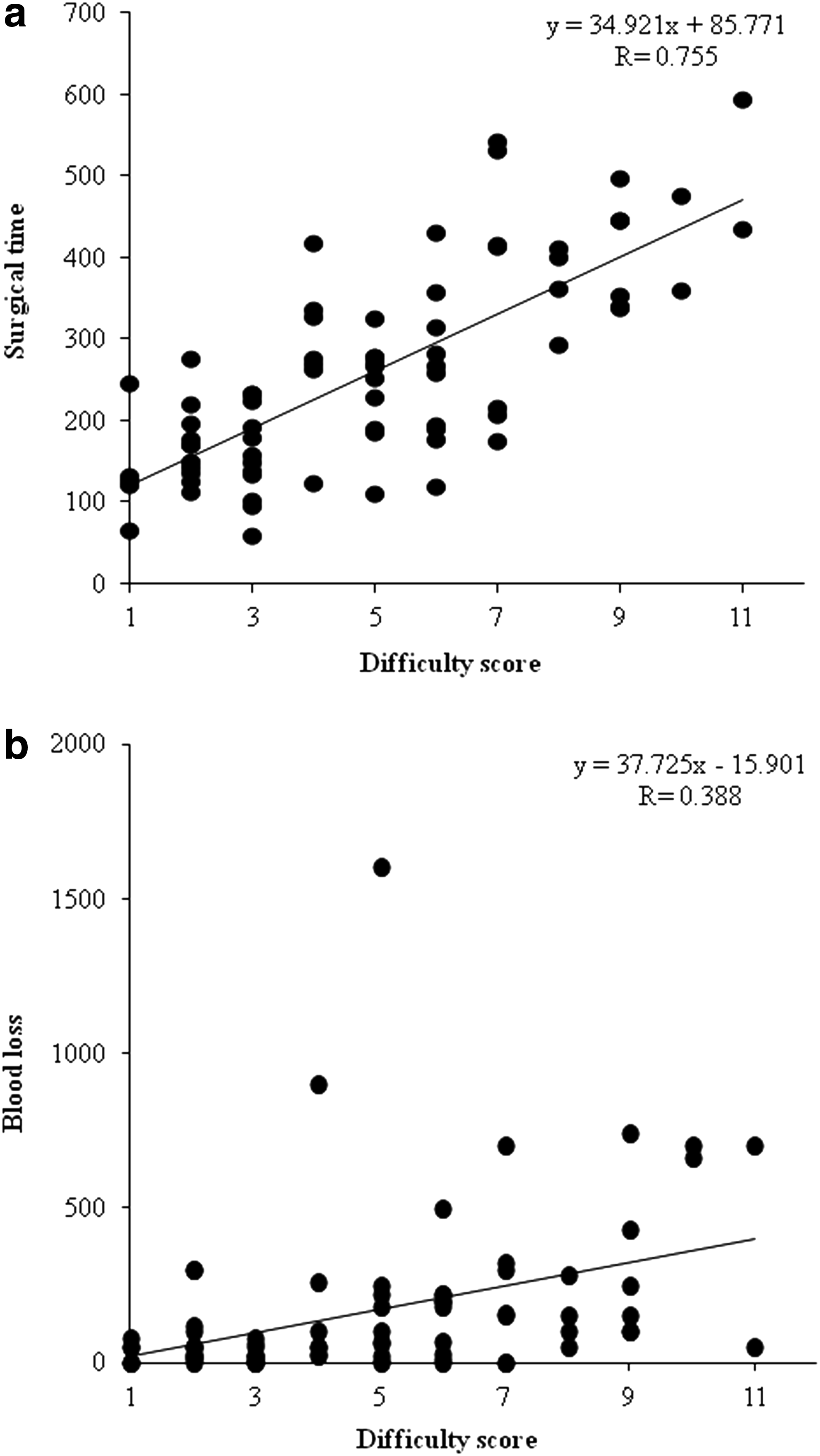
The correlation between difficulty score and surgical outcomes determined using Spearman's rank correlation test is shown in Figure 1. Significant correlations were found between the difficulty score and surgical time (R = 0.755, P < .001, Fig. 1a). The correlation between the difficulty score and blood loss was also significant (R = 0.388, P < .001, Fig. 1b).
Independent predictive factors for prolonged operation time and increased blood loss
The cutoff point of surgical time of 280 minutes was determined using ROC curve analysis. Univariate analysis showed that the indocyanine green test, platelet count, difficulty score, anatomical resection, and pure laparoscopic surgery were predictors of prolonged surgical time. Multivariate analysis demonstrated that the difficulty score was an independent predictive factor for prolonged surgical time in all patients (P < .001; odds ratio [OR] = 2.730; 95% confidence interval [CI] = 1.717–4.341, Table 2).
Alb, albumin; ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate transaminase; BMI, body–mass index; CI, confidence interval; γGTP, γ-glutamy transpeptidase; ICG, indocyanine green; Hb, hemoglobin; Ht, hematocrit; Plt, platelet count; PT, prothrombin time; T-bil, total bilirubin; WBC; white blood cell.
The cutoff point for increased blood loss was determined to be 65 mL using ROC curve analysis. Univariate analysis revealed significant differences among age, difficulty score, anatomical resection, pure laparoscopic surgery, and repeat liver resection for increased blood loss. Multivariate analysis showed that anatomical resection was an independent predictive factor for increased blood loss (P = .001, OR = 8.892, 95% CI = 2.509–31.515, Table 3).
Alb, albumin; ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate transaminase; BMI, body–mass index; CI, confidence interval; γGTP, γ-glutamy transpeptidase; ICG, indocyanine green; Hb, hemoglobin; Ht, hematocrit; Plt, platelet count; PT, prothrombin time; T-bil, total bilirubin; WBC; white blood cell.
Discussion
Many studies have demonstrated that LLR generally yields better short-term outcomes (decreased blood loss, complication rate, and postoperative hospital stay) without compromising long-term oncological outcomes, at least in selected patients and within the technical capabilities of each experienced center.7,16,22–24 It is expected that increasing numbers of surgeons will adopt laparoscopic approaches in the future, as evidenced by the exponential growth of LLR. 7 According to the second International Consensus Conference on Laparoscopic Liver Resection, LLR seems to be applied to a limited percentage of patients requiring liver resection (<40%), although some groups have reported a percentage >80%. 25
LLR is technically challenging in difficult cases. The difficulty of LLR depends on the technical complexity and various factors, such as the background of patients, size and location of the tumor, and degree of liver fibrosis. 26 Therefore, a difficulty scoring system using these factors is required to guide surgeons to progress from simple to highly technical laparoscopic resection. At the consensus conference held at Morioka in 2014, a novel difficulty scoring system was created to easily estimate the difficulty of LLR before surgery. 18 This scoring system was designed to select surgeons according to the score based on the following ranks: low (1–3 points), intermediate (4–6 points), or high (7–10 points). The difficulty score is a useful criterion for appropriate selection of surgeons. In some cases, the use of hand-assisted and/or the hybrid method would decrease difficulties associated with pure LLR.
Some reports have shown that surgical time was significantly longer in LLR than in OLR.27,28 Other reports have stated that a surgeon can master the skills required for LLR after performing 22–60 procedures,29–31 and surgical time reached a plateau after the surgeon had gone through the learning period. Prolonged surgical time correlated with an increased blood loss and morbidity rate.32,33 Therefore, it is useful to be able to predict the surgical time. Multivariate analysis in our study clearly demonstrated that the difficulty score had a strong correlation with surgical time. This finding indicates that surgical time can be predicted using a mathematical expression derived from the correlation coefficient, which will help avoid prolonged operation times. In our study, the morbidity and length of postoperative hospital stay did not correlate with difficulty score, although there was significant correlation between the morbidity and length of hospital stay (data not shown).
Ban et al. looked at cases in which the operator's difficulty index widely differed from the difficulty score of the procedure and found that mismatch mainly resulted from certain exceptional factors, such as repeated and/or multiple liver resections. In the present study, 14% of the surgeons had performed a repeat liver resection, and 5.1% had performed multiple liver resections, and we included these cases in this study because the numbers of LLRs performed in these cases have been increasing. Repeat liver resection was not a risk factor for prolonged surgical time and increased blood loss. Therefore, we believed that this scoring system might be adapted for repeat liver resection.
In conclusion, the difficulty scoring system reflected surgical outcomes, particularly the surgical time. Although this study was small and retrospective, it is the first study to validate the difficulty scoring system for LLR. Nevertheless, it is important that the scoring system be tested in a study involving a larger number of patients to provide further validation in a broader context.
Footnotes
Disclosure Statement
No competing financial interests exist.