
Abstract
Abstract
Objective:
Laparoscopic surgery is the current accepted approach in most pediatric surgical centers. In an attempt to further minimize the surgical trauma and improve cosmetic outcome, new techniques with a single incision through the umbilicus have been proposed and we believe they will become the standard choices for pediatric surgery. This report describes our initial experience with transumbilical single-incision laparoscopic surgery (TSILS) in children with conventional instruments.
Materials and Methods:
A retrospective review of 82 pediatric patients who underwent TSILS in children with conventional instruments from January 2011 to June 2015 was performed. The operations included 56 appendectomies, 9 cholecystectomies, and 17 spermatic vein ligations.
Results:
The average age by procedure was 6.2 years for appendectomy (range of 3–14 years); 12.4 years for cholecystectomy (range of 10–14 years); and 12.8 years for spermatic vein ligation (range of 11–14 years). The average operative time was 32 minutes for appendectomy (range of 25–56 minutes); 54 minutes for cholecystectomy (range of 35–95 minutes); and 23 minutes for spermatic vein ligation (range of 17–41 minutes). The average length of staying in hospital was 3 days (range of 2–5 days). All of the operations in 82 cases were successful. None required conversion to open or conventional laparoscopic surgery. There was no obvious wound pain. In addition, there were no wound infections on umbilicus and any other intraoperative complications. There was no obvious scar at patients’ umbilicus after postoperative follow-up for 2–4 weeks.
Conclusions:
TSILS is a safe and viable technique that may be used successfully in pediatric surgery. Additionally, excellent cosmetic results are obtained as evidenced by imperceptible umbilical scarring.
Introduction
L
Materials and Methods
A retrospective review of 82 pediatric patients who underwent transumbilical single-incision laparoscopic surgery (TSILS) in children using conventional instruments from January 2011 to June 2015 was performed. The operations included 56 appendectomies for simple and suppurative appendicitis, 9 cholecystectomies for gall stones, and 17 spermatic vein ligations for left varicocele. Data were collected on patient demographics, type of procedure, operative time, early or late complications, rate of conversion to traditional laparoscopic surgery or open procedure, hospital stay, and cosmetic outcome. We considered complications in appendectomies—wound infection, acute bleeding, incision hernia, and injury to any intra-abdominal viscera; in cholecystectomies—common bile duct injury and bile leak; and in spermatic vein ligations—vas deferens damage.
Technique
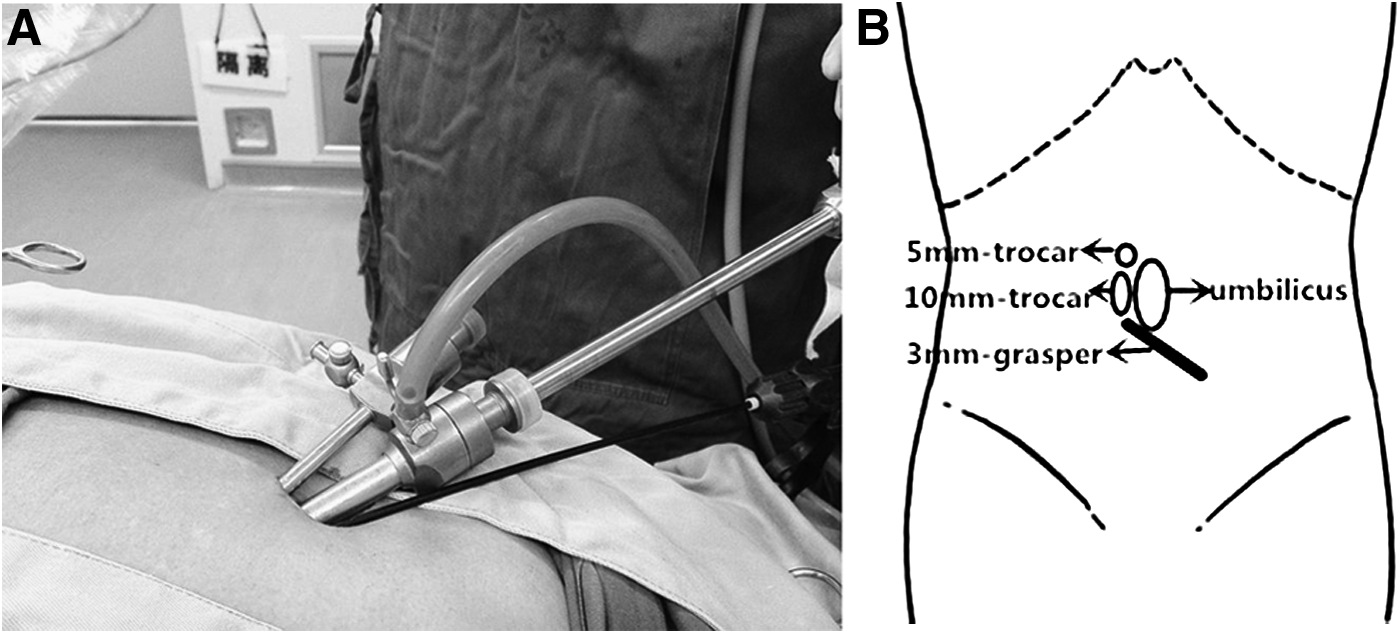
All 82 pediatric patients were treated under general anesthesia and orotracheal intubation. The technique for our TSILS involved making a 1.5–2.0-cm infraumbilical incision and dividing the umbilical stalk. Using an open Hasson technique, a 10-mm trocar was inserted through the incision at the median umbilical site. Establishment of pneumoperitoneum using carbon dioxide to an abdominal pressure of 10–12 mmHg was achieved. A 10-mm 30° optic was used in all operations. A 5-mm trocar was placed through the fascia ∼3 mm apart from 10-mm trocar at the upper umbilical incision. Then, in the inferior aspect of the umbilical incision, also ∼3 mm apart from 10-mm trocar, a 3-mm trocar was placed for establishing a channel in which 3-mm grasper can be inserted directly. Two trocars and grasper were not directly connected (Fig. 1A, B). All the instruments used were conventional laparoscopic instruments, including a 10-mm camera, a 3-mm grasper, and a 5-mm ultracision harmonic scalpel.
Appendectomy
The operation was similar to conventional laparoscopic appendectomy. The patient was placed in the supine position, with Trendelenburg position and the left side tilted up. The first operator stood on the patient's left side and the camera holder on the operator's right side. The 3-mm grasper was used to grasp the appendix. The 5-mm ultracision harmonic scalpel was used to divide adhesive bands and take down the mesentery for dissection of the appendix. Once the appendix was completely released, it was ligated by Johnson 2–0 endoloops and dissected by ultracision harmonic scalpel. Then, it was loaded into the specimen bag. After intraoperative inspection, the peritoneal cavity was desufflated and the instruments were withdrawn. We connected the incisions at the end of the case, and retrieved the specimen bag without any difficulty. The umbilical fascia was then closed with three 2–0 Vicryl sutures. The patient was given routine postoperative analgesia with 0.75% ropivacaine and 0.5% lidocaine on umbilicus. The patient was extubated and taken to recovery.
Cholecystectomy
The operation was similar to the conventional laparoscopic cholecystectomy. The patient was placed in the supine position, with reverse Trendelenburg position and the left side tilted up. The first operator stood on the patient's left side, and the camera holder stood on the operator's right side. Once the infundibulum had been cleared of its investing peritoneum, the cystic artery and cystic duct were identified entering the gallbladder. The cystic artery was cut by an ultracision harmonic scalpel. After the gallbladder was freed off the cystic plate, the cystic duct was ligated by Johnson 2–0 endoloops and dissected by ultracision harmonic scalpel. Then, it was loaded into the specimen bag. After intraoperative inspection, the peritoneal cavity was desufflated and the instruments were withdrawn. We connected the incisions at the end of the case, and retrieved the specimen bag without any difficulty. The umbilical fascia was then closed with three 2–0 Vicryl sutures. The patient was given routine postoperative analgesia with 0.75% ropivacaine and 0.5% lidocaine on umbilicus. The patient was extubated and taken to recovery.
Spermatic Vein Ligation
The operation was similar to the conventional laparoscopic spermatic vein ligation. The patient was placed in the supine position, with Trendelenburg position and the right side tilted up. The first operator stood on the patient's right side, and the camera holder stood on the operator's right side. The 3-mm grasper was used to grasp the peritoneum 2–3 cm over the internal inguinal ring. The 5-mm ultracision harmonic scalpel was used to incise the peritoneum and isolate the vessel plexus. The spermatic vein and artery and the vas deferens were identified. When the spermatic vein was completely separate from the vessel plexus, the spermatic vein was ligated by ultracision harmonic scalpel. After intraoperative inspection, the peritoneal cavity was desufflated and the instruments were withdrawn. We connected the incisions at the end of the case. The umbilical fascia was then closed with three 2–0 Vicryl sutures. The patient was given routine postoperative analgesia with 0.75% ropivacaine and 0.5% lidocaine on umbilicus. The patient was extubated and taken to recovery.
Results
The average age by procedure was 6.2 years for appendectomy (range of 3–14 years); 12.4 years for cholecystectomy (range of 10–14 years); and 12.8 years for spermatic vein ligation (range of 11–14 years). The average operative time was 32 minutes for appendectomy (range of 25–56 minutes); 54 minutes for cholecystectomy (range of 35–95 minutes); and 24 minutes for spermatic vein ligation (range of 17–41 minutes). The average length of stay in hospital was 3 days (range of 2–5 days). All of the operations in 82 cases were successful. None required conversion to open or conventional laparoscopic surgery (CLS). There was no obvious wound pain. In addition, there were no wound infections on umbilicus and any other intraoperative complications. There was no obvious scar at patients’ umbilicus after postoperative follow-up for 2–4 weeks.
Discussion
With increased experience and improved instrumentation, there is a trend in minimally invasive surgery toward new less invasive approaches to reduce pain and decrease recovery time and improve cosmetics. 8 New techniques such as natural orifice translumenal endoscopic surgery (NOTES) and SILS have been developed in surgery.
The NOTES technique is performed through a solitary natural orifice such as the mouth, vagina, or rectum. 9 Potential advantages purported to occur with NOTES include improved cosmesis, reduced systemic inflammatory response, reduced pain, or reduced incision-related complications. 10 However, NOTES is still in the early stages of development and has not yet gained widespread acceptance. There are various barriers to the development of NOTES, including unfamiliar visual approach, limitations of existing instruments, lack of a stable surgical platform, and ethical principles. These limitations have resulted in an increasing trend toward the application of SILS, in which complex operations could be performed through a single incision through the umbilicus.
However, performing SILS is more difficult than performing CLS because of problems related to the instrument and hand collision, reduced intracorporeal work space, triangulation difficulties, and a steep learning curve. So, most SILSs need specialized multichannel ports and specialized laparoscopic instruments (curve, bent tip, rotating mechanism, etc.) to facilitate performing. These devices are expensive and add additional costs in comparison with CLS. These issues may explain the limited application of SILS in practice, especially in developing countries.
To minimize material cost of the procedure, TSILS, which we called transumbilical single-incision bicannular triapparatus laparoscopic surgery, was performed using conventional laparoscopic instruments. Our experience showed that TSILS with conventional straight laparoscopic instruments and without a specialized port was feasible and safe in pediatric surgery. In our series, there was no conversion to open or CLS. Although the lengths of incision on umbilicus were increased 0.5–1 cm than standard multiport laparoscopic surgery, the patients did not complain about obvious wound pain. In addition, there were no wound infections on umbilicus and any other intraoperative complications, such as bleeding, incision hernia, injury to any intra-abdominal viscera, common bile duct injury, bile leak, and vas deferens damage.
We primarily used three ports in the early stages of exploration. We found that hand collision between the three-port pose was the biggest challenge. In our practice and understanding, the inferior trocar used for retraction with grasper could be removed considering its infrequent in–out operation, and we placed working trocar and grasper 30–45° laterally to the optic trocar to achieve adequate triangulation and also to avoid air leak. Keeping all ports 0.3–0.5 cm apart could reduce the clashing of the extra-abdominal parts of the ports and leaking of CO2. In addition, pneumoperitoneum was well maintained throughout the procedure. Movement of one instrument or the camera often resulted in inadvertent movement of an adjacent instrument. So, avoiding frequent conversion, once found, the best location to operate was partly essential. Conversion to conventional laparoscopic surgery should be performed if unstoppable intraoperative blood or difficult operation happened.
The primary advantage of our procedure in children is improved cosmesis with an anatomically concealed incision. The entire procedure can be performed through an umbilicus incision as small as 15 mm, none of which needed extension of the initial incision. Our early experience provides evidence that TSILS can be applied for routine appendectomies, cholecystectomies, and spermatic vein ligation in the pediatric population. We believe that TSILS will be widely used in most pediatric surgeries in the future, especially in developing countries.
Conclusion
Our initial data showed that TSILS was a safe and viable technique in pediatric surgery. This procedure will be further applied in a large group of patients in abdominal and urological surgery. We are unable to comment on the superiority of TSILS over conventional laparoscopy at this time. We hope to compare outcomes from our TSILS population with our conventional laparoscopy patients in the future.
Footnotes
Acknowledgment
The authors would like to thank their colleagues from the Department of Pediatric Surgery for their assistance with data collection.
Compliance with Ethical Requirements
This research has fully complied with research ethics.
Disclosure Statement
No competing financial interests exist.