
Abstract
Abstract
Background:
This study aimed to evaluate the feasibility and efficacy of solo-surgeon retroauricular thyroidectomy.
Materials and Methods:
For solo-surgery, we used an Endoeye Flex Laparo-Thoraco Videoscope (Olympus America, Inc.). A Vitom Karl Storz holding system (Karl Storz GmbH & Co.) composed of several bars connected by a ball-joint system was used for fixation of endoscope. A snake retractor and a brain-spoon retractor were used on the sternocleidomastoid.
Results:
Endoscopic thyroidectomy using the solo-surgeon technique was performed in 10 patients having papillary thyroid carcinoma. The mean patient age was 36.0 ± 11.1 years, and all patients were female. There were no postoperative complications such as vocal cord paralysis and hematoma. When compared with the operating times and volume of drainage of a control group of 100 patients who underwent surgery through the conventional retroauricular approach between May 2013 and December 2015, the operating times and volume of drainage were not significantly different (P = .781 and .541, respectively).
Conclusion:
Solo-surgeon retroauricular thyroidectomy is safe and feasible when performed by a surgeon competent in endoscopic thyroidectomy.
Introduction
T
Surgery performed by one surgeon operating with one scrub nurse is called “solo-surgery.” 4 Several reports have been published that evaluated the feasibility and efficacy of solo-surgery in abdominal and pelvic surgery.5–7 However, there have been no published reports of solo-surgery for thyroidectomy. Using current endoscopic and robotic surgical techniques, at least one assistant is needed to hold the endoscope or to retract the thyroid, sternocleidomastoid (SCM) muscle, or trachea. 1 To provide a large enough work space for the main operator, and to prevent interference from the assistant's body or the endoscope, the assistant should stand away from the main operator, and the endoscope and retractor should be kept attached to the elevated flap. These restrictions tire the assistant quickly; therefore, the current endoscopic retroauricular approach to thyroidectomy is limited by the narrow working space created by the presence of the assistant and the potential interference between the endoscope and instruments. Solo-surgery may be a good alternative to traditional endoscopic thyroidectomy in terms of widening the work space of the main operator by regulating the positions of instruments, retractors, and the endoscope, thereby reducing possible interferences during the operation. In this study, we aimed to evaluate the feasibility and efficacy of solo-surgeon retroauricular thyroidectomy using self-holding endoscopes and retractors.
Materials and Methods
Instrument and equipment
To prevent the endoscope from limiting the movement of instruments, we used an Endoeye Flex Laparo-Thoraco Videoscope (Olympus America, Inc.) (Fig. 1). This endoscope has a rigid body with a flexible end that can bend in four directions. Using this feature, the endoscope can be kept attached to the medial side of the elevated flap, widening the surgical field of view for the main operator. A Vitom Karl Storz holding system (Karl Storz GmbH & Co.) composed of several bars connected by a ball-joint system was used. Its base was anchored to the operating table rail, and its tip grasped the camera with a clamp. A snake retractor and a brain-spoon retractor were used on the SCM. Its base was also anchored to the operating table rail.

Positioning instruments for solo-surgeon retroauricular endoscopic thyroidectomy. Arrowheads: snake retractor. Arrows: endoscope-holding system.
Surgical procedure
The technique for retroauricular thyroidectomy has been described. 1 After elevation of the flap and application of the self-retraining retractor, the brain-spoon retractor, connected to the snake retractor, was applied to retract the SCM, and the endoscope was fixed in position by the holding system. The rigid body of the endoscope was inserted and attached to the anterior side of the elevated flap (Fig. 1). The flexible end was bent to be parallel to the recurrent laryngeal nerve (Fig. 2 and Supplementary Videos S1 and S2; Supplementary Data are available online at www.liebertpub.com/lap). When required, endoscope repositioning was performed using a knob-controlled manual unlock with one hand releasing the brake and the other hand repositioning the endoscope holder. All procedures, except the flap elevation, were performed by a single surgeon assisted by a scrub nurse.
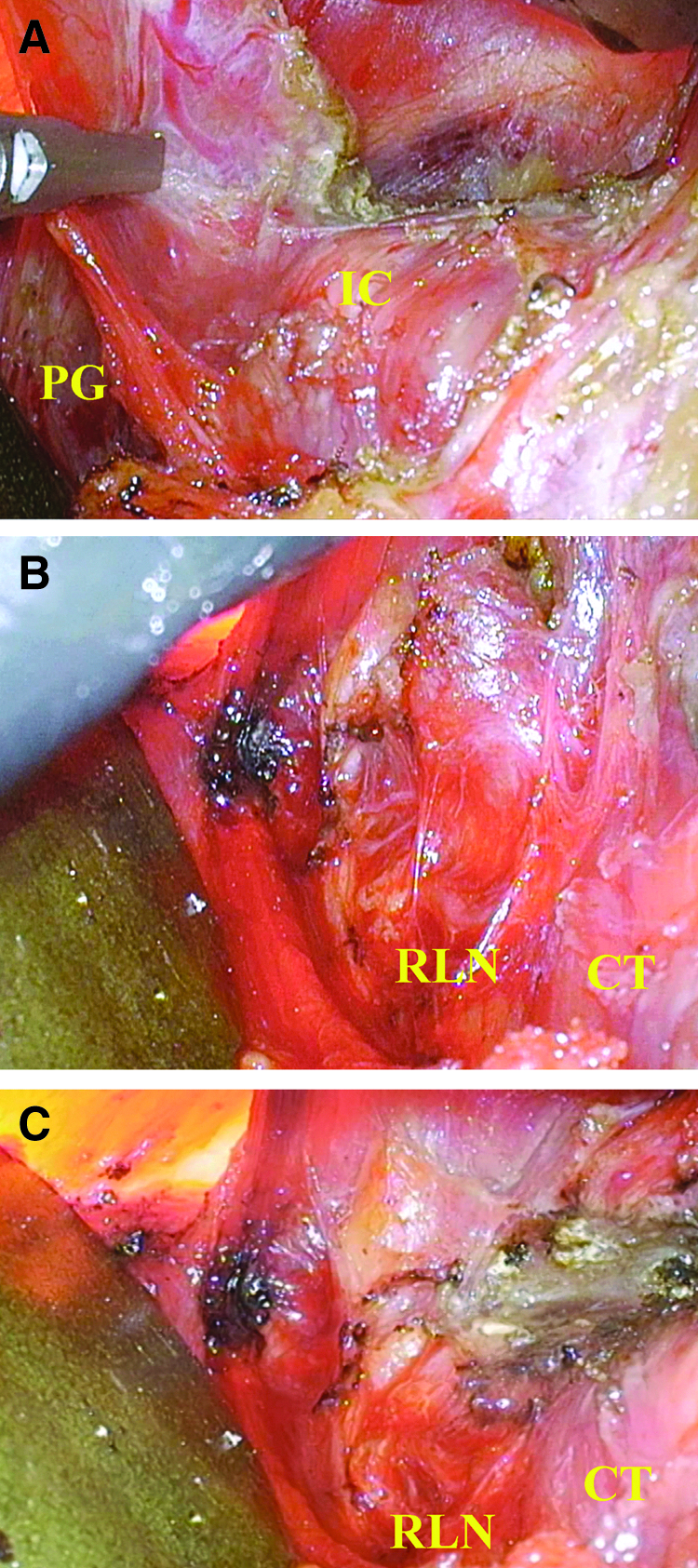
Operating procedure. Endoscopic dissection can be performed easily in the wide working space, (the direction of surgical view), that is kept in a fixed direction.
Results
Endoscopic thyroidectomy using the solo-surgeon technique was performed in 10 patients with papillary thyroid carcinoma. The mean patient age was 36.0 ± 11.1 years, and all patients were female. There was no conversion to conventional open thyroidectomy, nor was there any vocal cord paralysis, inadvertently excised parathyroid glands, or hematoma formation. In addition, there were no injuries to the great vessels, esophagus, trachea, or marginal mandibular nerve. When compared with a control group of 100 patients who underwent surgery through the conventional retroauricular approach between May 2013 and December 2015, the operating times were not significantly different between solo-surgery and conventional endoscopic surgery (127.5 ± 8.7 minutes versus 128.3 ± 36.2 minutes; P = .781). The volume of drainage was also not significantly different between conventional retroauricular thyroidectomy and solo-surgery (143.3 ± 53.8 mL versus 149.6 ± 65.1 mL) (P = .541).
Discussion
The retroauricular approach to endoscopic thyroidectomy offers substantial benefits to patients, such as improved cosmesis, reduced pain, and improved postoperative voice outcomes.1,8 The approach is also beneficial to those patients who cannot afford robotic thyroidectomy. Endoscopic thyroidectomy, however, inevitably results in the disassociation of the operator's hand and eye because the endoscope is directed by an assistant, causing the inconvenience of indirect observation and indirect manipulation. 9 Moreover, the endoscope and the assistant's arm frequently hinder the movement of the main operator's instruments. Ultimately, failure to achieve optimal coordination can lead to disturbances in the surgeon's concentration and poor surgical outcomes.
The authors believe that solo-surgery endoscopic thyroidectomy may help to overcome the disadvantages of the endoscopic approach. To the best of the authors' knowledge, this study is the first to evaluate the feasibility of solo-surgeon endoscopic retroauricular thyroidectomy. Solo-surgeon endoscopic thyroidectomy is a simple operation, and, in the authors' opinion, solo-surgery can make it even easier for endoscope-competent surgeons. While performing a solo-surgery thyroidectomy, it is important to create a wide space and maintain a steady view to avoid interruption by the endoscope or retractor, which can be annoying and time consuming, especially because the operators change the position of the endoscope or retractor on their own. In this study, the endoscope was attached to the anterior side of the elevated flap to create a wide workspace. A 30° rigid endoscope, which is usually used in endoscopic thyroidectomy, makes it difficult to obtain an adequate view and frequently cross the mid-portion of working space. However, the rigid endoscope with a flexible end used in this study makes it possible to obtain a wide surgical field for instrument manipulation.
Solo-surgery can be divided into total and partial procedures. 10 Total solo-surgery involves a single surgeon completing the entire procedure, whereas partial solo-surgery involves using solo-surgery as one part of the total operation. Although solo-surgery endoscopic retroauricular thyroidectomy is limited by the need for an assistant during flap elevation, eliminating the need for an assistant during the main procedure is helpful, especially when there are few assistants.
The interference of the endoscope and the assistant's arm is a disadvantage to surgeons performing endoscopic surgery, but it can be mitigated (Fig. 3). A previous study found that the operating proficiency and duration of laparoscopic surgery were similar between surgeons using camera holders versus surgeons using human assistants. 11 Because a retroauricular approach inevitably narrows the field of view, solo-surgery can reduce operation time by reducing the interference of instruments, and by maintaining the appropriate position of the endoscope by the main operator.
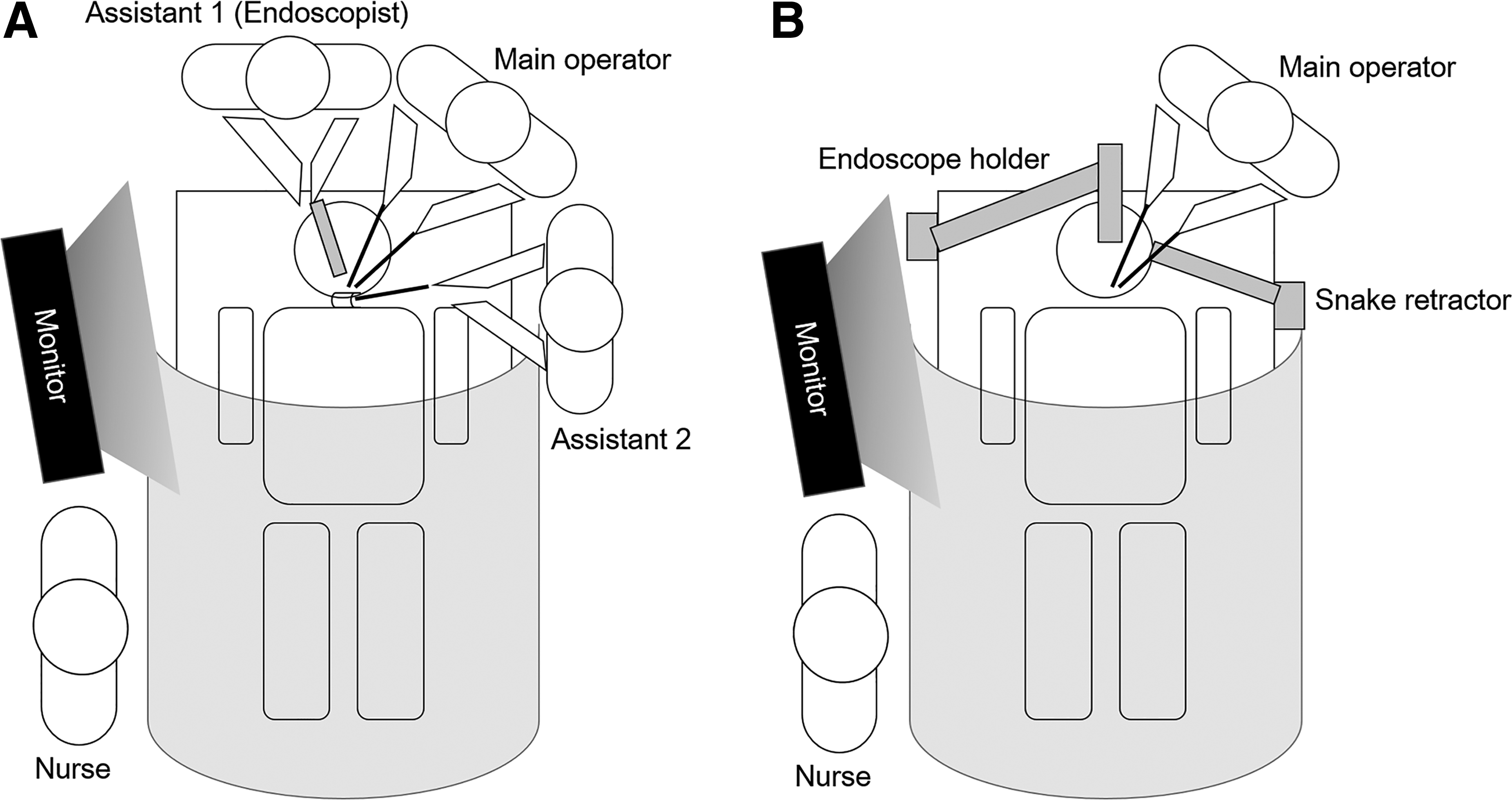
Schematic comparison between conventional
The camera holders used during solo-surgery are either passive or active; the former are manually controlled and the latter are driven by electrical motors. 10 In our study, a passive endoscope holder was used that required two hands for repositioning, and the endoscope was fixed in one position as much as possible with intermittent repositioning of the flexible tip with one hand. An active or passive endoscopic holder that can be repositioned with one hand could shorten operation time further. Additional studies of more easily repositioned endoscope holders for retroauricular thyroidectomy are necessary; there have been few studies on the most appropriate instruments and holders for solo-surgery. 12
In summary, solo-surgeon endoscopic retroauricular thyroidectomy has the following advantages: (1) eliminating the need for an assistant during the major part of the surgery, which can be helpful in situations in which there are few assistants, (2) coordinating the endoscope and instruments, and widening the work space to keep instruments in their ideal positions, and (3) allowing the main operator to concentrate more intensely on the procedure by providing stable observation of the endoscope and regulation of the surgical view. Despite the small number of patients included in this study, solo-surgery appears to be feasible in retroauricular endoscopic thyroidectomy, and may be a substitute for robotic instruments when they cannot be used. We postulate that solo-surgeon retroauricular thyroidectomy is safe and feasible when performed by a surgeon competent in endoscopic thyroidectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.