
Abstract
Abstract
Background:
The purpose of this study was to explore the feasibility and safety of laparoscopic partial splenectomy (LPS) using a harmonic scalpel (HS) combined with bipolar coagulation.
Materials and Methods:
Using HS and bipolar coagulation technology, 18 patients suffering from splenic cystic neoplasm were treated with LPS between January 2010 and December 2014, and their clinical data were analyzed retrospectively.
Results:
LPS was performed successfully without conversion to open surgery in all cases. The mean intra-operative blood loss was 75.8 ± 33.5 mL, and the mean operation time was 54.3 ± 16.6 minutes (range, 48–82 minutes). No cases of postoperative bleeding, infection, or pancreatic fistula occurred. No patient required total splenectomy. The mean hospital stay was 6.6 ± 3.2 days, and the median postoperative follow-up was 19.8 months (range, 5–60 months). All patients recovered successfully, with normal complete blood counts and without any recurrence on follow-up.
Conclusions:
LPS is a safe and feasible operation for selected patients. Combined use of an HS and bipolar coagulation can shorten the operation time, reduce blood loss, and improve the safety of the operation.
Introduction
O
Because the spleen is rich in sinusoids, it is prone to bleeding during operation or delayed bleeding postoperatively from the cut surface of the residual spleen. Therefore, it is important to select appropriate surgical instruments. Usually, one of the following instruments can be used to transect the splenic parenchyma: scalpel, LigaSure, CUSA, waterjet, single-stage coagulation, argon knife, and others. However, in previous studies, combined use of an ultrasonic scalpel and bipolar coagulation in laparoscopic liver resection has been shown to significantly reduce intraoperative bleeding and shorten the operative time. 4 To maximize the preservation of splenic function, we combined use of an ultrasonic scalpel and bipolar coagulation in LPS.
Materials and Methods
Patients and methods
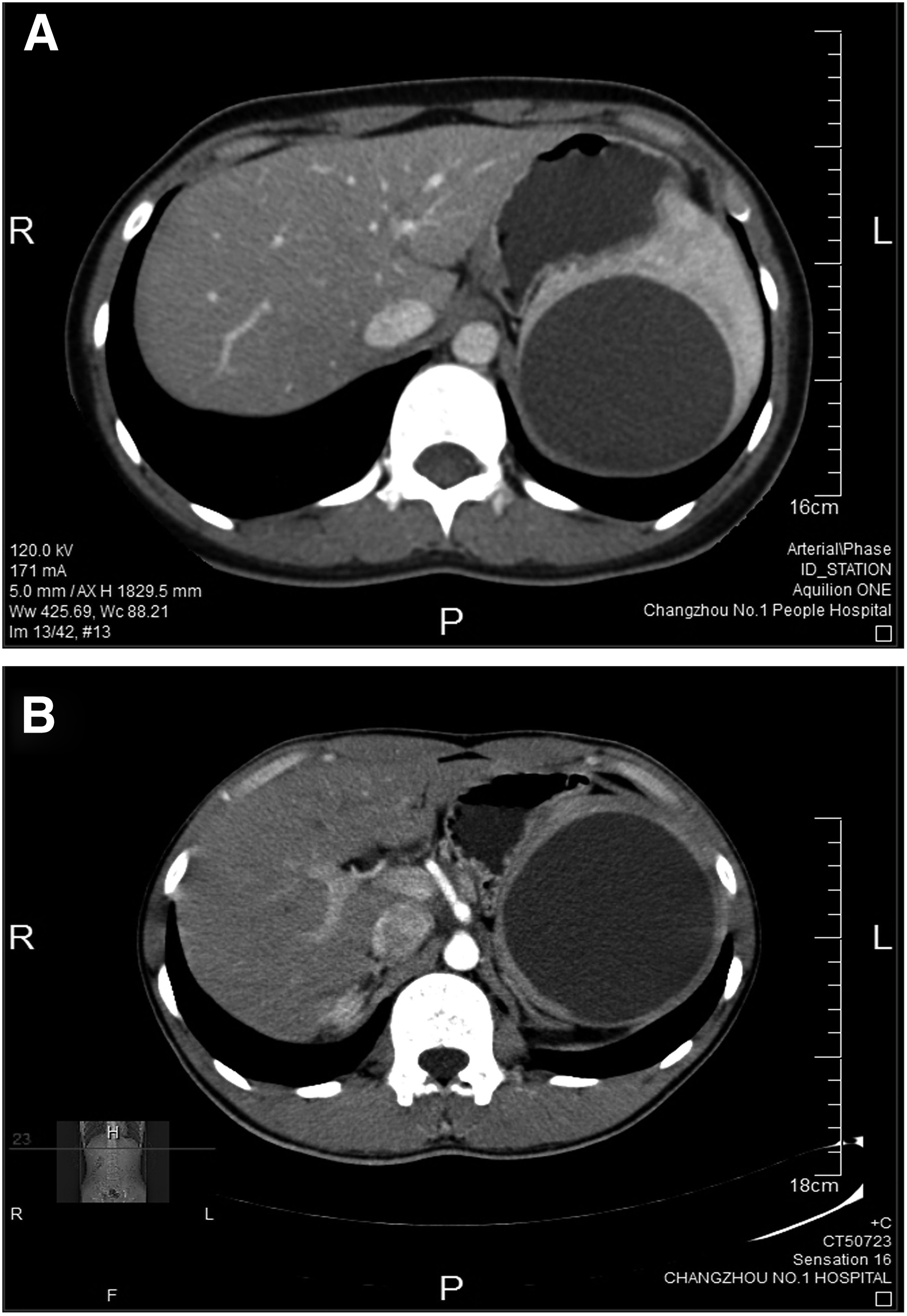
This study included 18 patients suffering from benign splenic diseases who were treated between January 2010 and December 2014. The indications for LPS were as follows: (1) preoperative computed tomography (CT) or magnetic resonance (MR) examinations showing a splenic cystic or solid tumor (diameter >5 cm) and (2) a tumor or cyst located at the pole of the spleen. Exclusion criteria were as follows: (1) the tumor was located in the middle of the spleen; (2) the tumor was close to the door; (3) preoperative CT/MRI indicated that malignant tumor clouds were not to be excluded; (4) there was a history of epigastric operation; and (5) there was a history of hepatitis, cirrhosis, and hypersplenism. Contraindications were as follows: (1) severe cardiopulmonary dysfunction and being unfit for general anesthesia or surgery; (2) extensive intra-abdominal adhesions; and (3) coagulation disorders.
Written informed consent was obtained from all of the adult patients. For children, written informed consent was obtained from their parents. The Institutional Review Board of The Third Affiliated Hospital of Soochow University approved this study protocol.
Operative technique
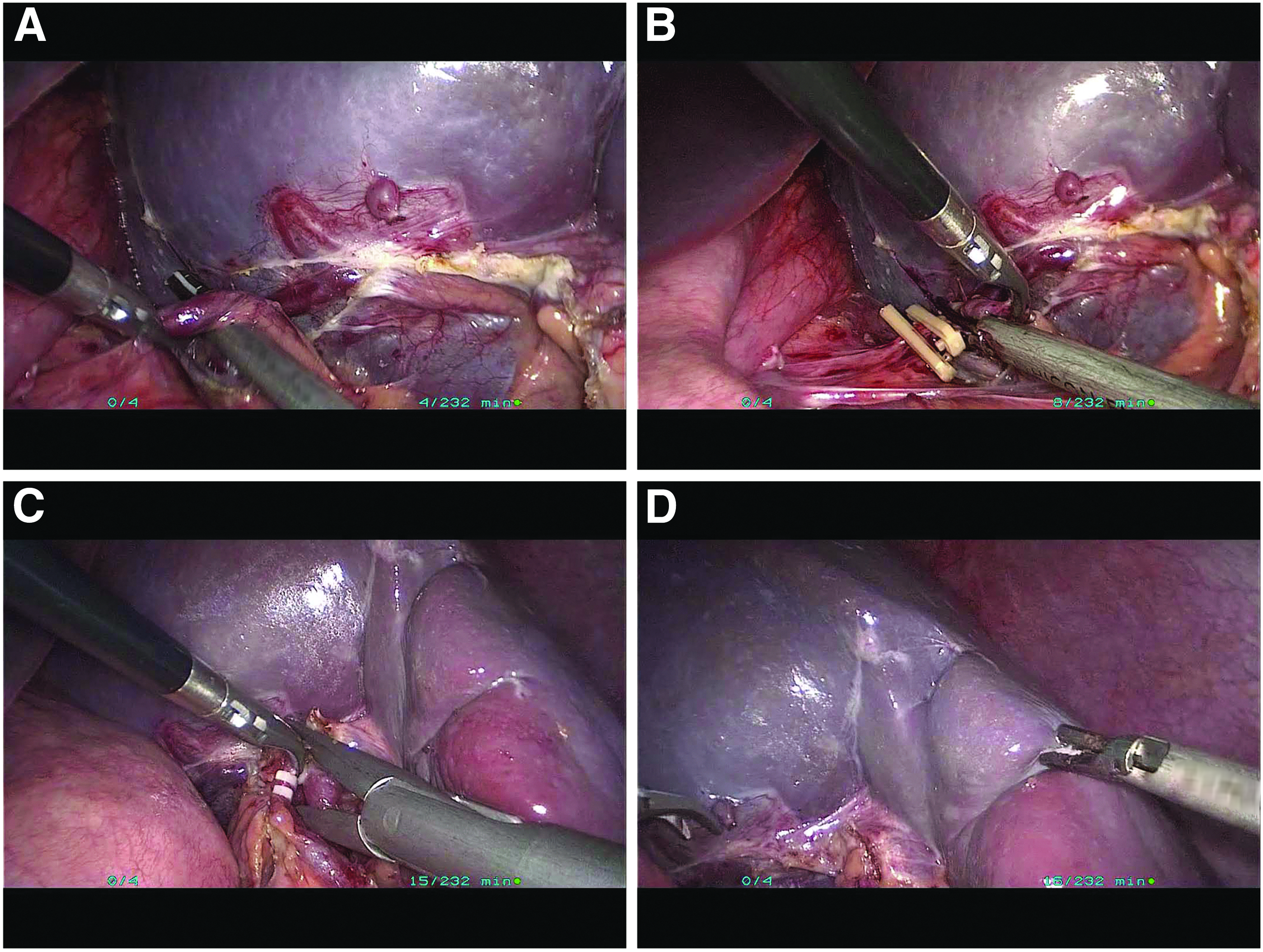
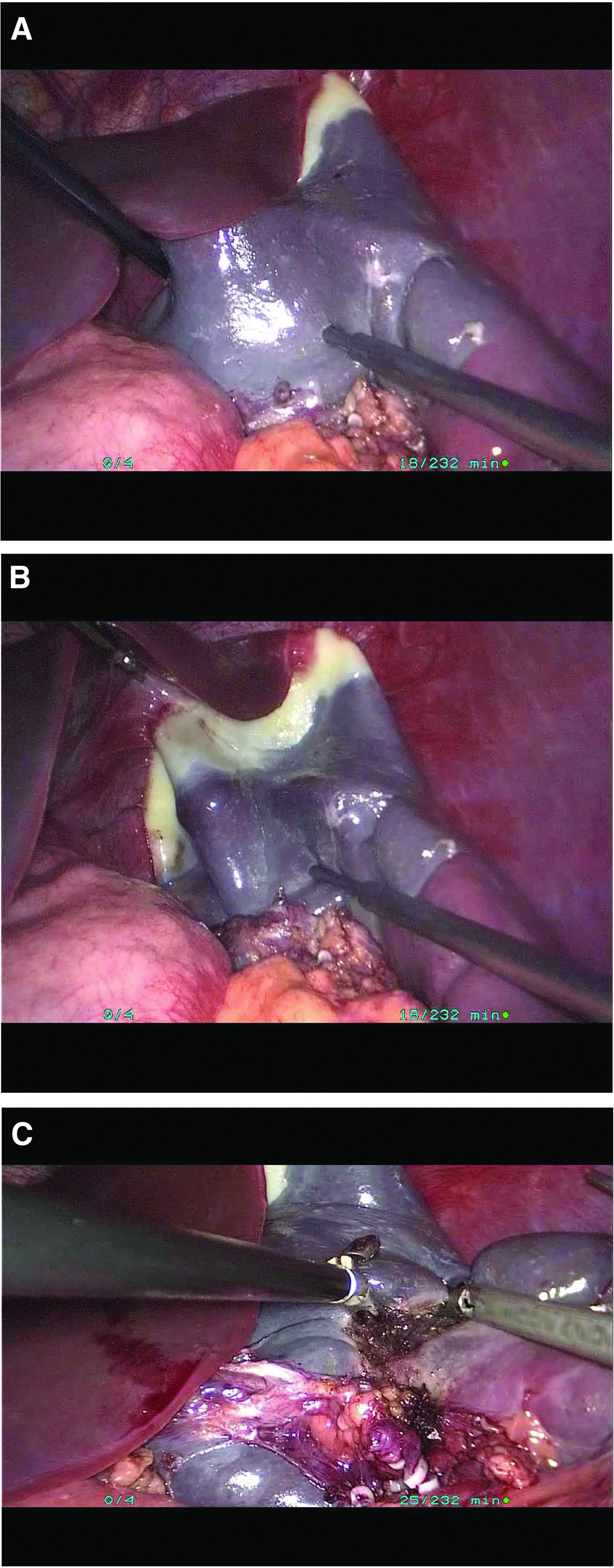
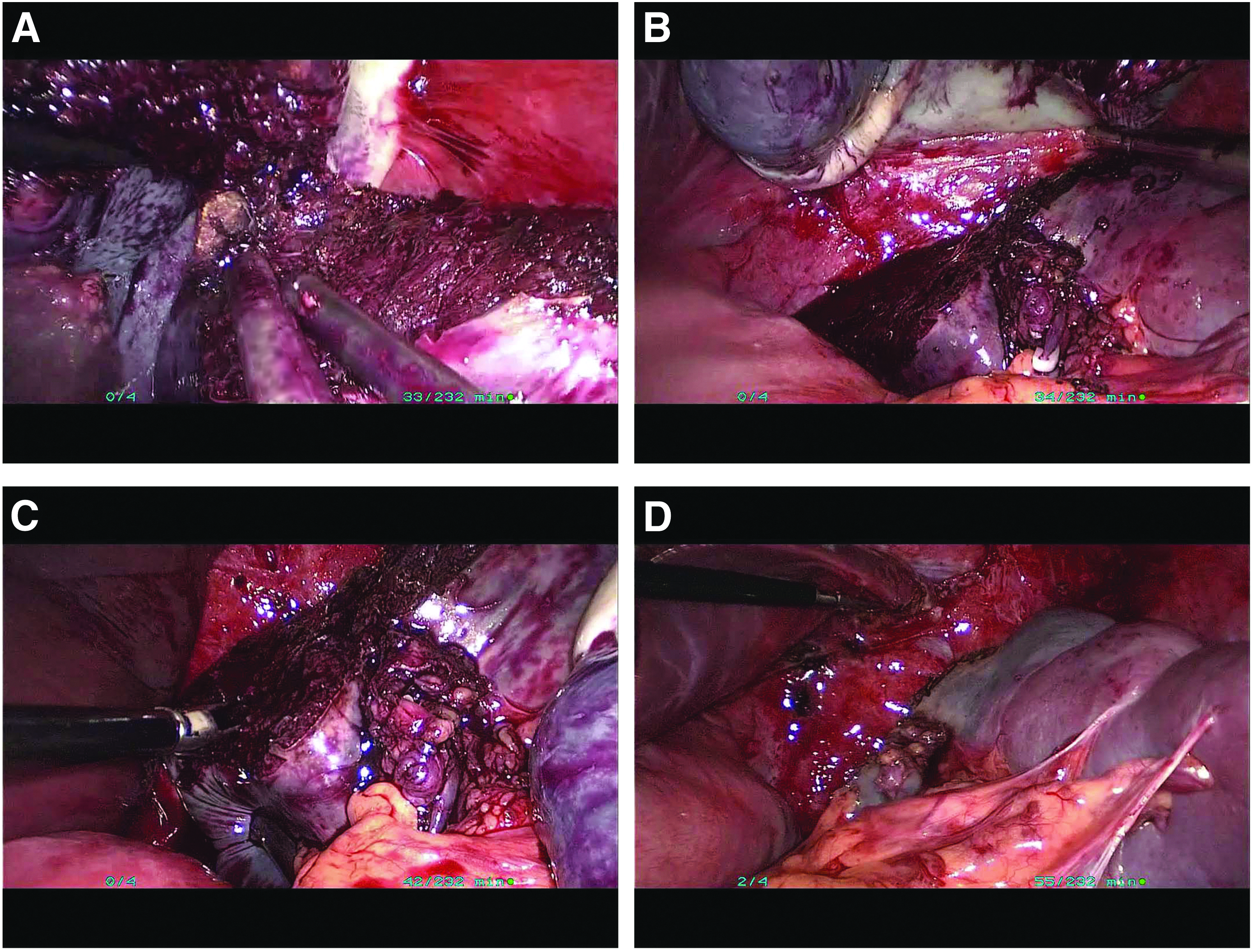
All operations were performed by the same surgeon. Under general anesthesia, the patient was placed in either a “low lithotomy” or a split-leg position, with the operating surgeon standing on the patient's right side, the camera assistant standing between the patient's legs, and the second assistant standing on the patient's left side. Pneumoperitoneum was achieved by Veress needle and was maintained at a pressure of 12 mmHg with a flow rate of 1.5 L/min. A 10-mm camera port was placed just below the umbilicus, and a 30-degree telescope was used. To gain better access, the patient was placed with the head elevated 30° and a slight elevation of the left side. Three additional ports were placed under vision: one 5-mm port just below and to the left of the xiphoid cartilage, one 5-mm port 5 cm below the xiphoid cartilage, and one 10-mm port parallel to the umbilicus in the left mid-clavicular line. The omentum over the spleen was pulled down, and the spleen was clearly exposed. The splenic hilar dissection was carefully performed, and the superior/inferior lobar vessels going toward the lesions were identified and dissected. All these vessels were clamped with a Hem-o-lok, which resulted in ischemia of the cyst/tumor-containing part of the spleen with a well-defined line of demarcation (Fig. 2). The lesion, if cystic, was punctured with the needle, and the fluid was aspirated. A harmonic scalpel (HS; Ethicon Endo-Surgery, Inc.) was used to cut the spleen along the lesion, keeping a 5–8-mm rim of devascularized splenic tissue (Fig. 3). Parenchymal transection was performed with the HS in the blunt mode at level 2 or 3. During the dissection of the parenchyma, the assistant maintained the exposure of the spleen with forceps or suction. The small venous tributaries encountered during the transection were coagulated by bipolar electrocautery before being cut with the HS. After the splenic parenchymal transection, the ligaments and adhesions around the spleen were dissected with blunt and sharp methods (Fig. 4). If the coagulated tissue adhered to the electrocautery blades, then saline was poured over the blades to facilitate smooth removal of the coagulated tissue and to prevent further bleeding from the frail vessels.
The specimen was placed in a bag and removed through the enlarged umbilical incision. A closed suction drain was placed lateral to the residual spleen.
Results
The patients in our study included 10 men and 8 women, and the mean age was 29.3 ± 6.5 years (range, 5–42 years). In 12 cases, the lesions were located in the upper pole of the spleen (Fig. 1), and in 6 cases, the lesions were located in the lower pole of the spleen (Table 1). In all cases, LPS was performed successfully without conversion to open surgery. The average intra-operative blood loss was 75.8 ± 33.5 mL, and the mean operation time was 54.3 ± 16.6 minutes (range, 48–82 minutes). No postoperative bleeding, residual infection, or pancreatic fistula occurred, and the mean hospital stay was 6.6 ± 3.2 days. No patient required a total splenectomy. Pathological examination indicated epidermoid cysts in 12 cases, cavernous lymphangioma in 4 cases, and splenic hemangioma in 2 cases. The median postoperative follow-up was 19.8 months (range, 5–60 months). All patients recovered, with normal complete blood counts and without any recurrence as assessed by postoperative B-ultrasonography.
Discussion
Splenic cysts are classified as primary cysts (true) or pseudocysts (secondary) on the basis of the presence or absence of lining epithelium, respectively. True cysts of the spleen are very rare and are typically classified as cystic hemangiomas, cystic lymphangiomas, and epidermoid and dermoid cysts. Splenic cysts with a diameter greater than 5 cm should be managed surgically to prevent the increased risk of complications, such as infection, rupture, or intracavitary bleeding, because conservative options, such as percutaneous aspiration or sclerosis, are associated with high rates of recurrence and infection.5,6
The conventional treatment of splenic cysts has been open or laparoscopic total splenectomy. In recent years, a spleen-preserving surgical approach has been recommended for treating benign splenic diseases, because the spleen is known to play an important role in normal homeostasis. The spleen has several functions, including the regulation of the circulating blood volume, hematopoiesis, immunity, and protection against infections and malignancies. Postsplenectomy overwhelming infection and sepsis are serious morbid complications associated with a high fatality rate. 7
Morgenstern and Shapiro reported the first resection of a cyst and a portion of the contiguous splenic parenchyma (partial splenectomy). 8 Subsequently, in the past decade, several authors have reported LPS for nonparasitic splenic cysts.9–11 The most difficult step in this surgery has been the control of bleeding laparoscopically during parenchymal transection, which limits its widespread use.
Our previous study showed that use of an HS combined with bipolar coagulation could reduce intra-operative bleeding in laparoscopic liver resection. 4 Therefore, we tested the application of this technique in LPS. The results showed that the mean intra-operative blood loss was 75.8 ± 33.5 mL, and the mean operation time was 54.3 ± 16.6 minutes (range, 48–82 minutes). No postoperative bleeding, residual infection, or pancreatic fistula occurred.
The HS is an instrument that cuts and coagulates tissue with ultrasound. The main drawback of the HS is its inability to control bleeding from the cut splenic surface, especially from the splenic blood sinuses. Bipolar coagulation can well compensate for the deficiencies of the HS. Bipolar coagulation applies local high-frequency power to the tissue so that the blood vessel is dehydrated and coagulated, achieving the purpose of hemostasis. Bipolar coagulation has some advantages compared with monopolar electrocoagulation, in that it results in less coagulation scale, more effectively achieves hemostasis, and is safer, especially for patients with a pacemaker. However, the use of bipolar cautery is not always satisfactory, because coagulated tissue often adheres to the electrocautery blades. With present technology, low-flow irrigation with saline droplets can prevent adhesion of debris to the blades, clear the cut splenic surface, reduce charring, and facilitate smooth removal from the coagulated vessels without tearing of fragile tissues.
Conclusion
The combined use of an HS with bipolar coagulation in LPS can offer the full advantages of both techniques to shorten the operation time, reduce blood loss, and significantly improve the safety of the operation. Even with the development of many new devices during the past few years, in our opinion, use of an HS and bipolar cautery can be considered an optimal method for laparoscopic splenic transection.
Footnotes
Acknowledgments
This work was supported by the Natural Science Fund of Jiangsu Province (Grant No. H201548) and the National Natural Science Foundation of China (Grant No. 81502002).
Disclosure Statement
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.