
Abstract
Abstract
Objectives:
The purpose of this study is to identify the safety and feasibility of laparoscopic caudate lobectomy.
Background:
Caudate lobectomy has been considered as technically difficult because of the deep location of the caudate lobe and its proximity to great vessels. Due to the technical difficulty, laparoscopic caudate lobectomy was not feasible in patients with malignancy in the caudate lobe.
Methods:
Six consecutive patients with caudate hepatic malignancy received laparoscopic caudate lobectomy at Samsung Medical Center from September 2007 to May 2014. Demographic data, intraoperative parameters, and postoperative outcomes were assessed.
Results:
All procedures for these 6 patients with caudate malignancy were completed with totally laparoscopic technique. Only 1 patient who had hepatocellular carcinoma in the Spiegel lobe underwent partial caudate lobectomy, and others underwent complete caudate lobectomy. The mean tumor size was 2.65 cm (range 0.9–5.1 cm). The mean operative time was 382 minutes (range 168–615 minutes) and none required transfusion. The mean duration of hospital stay was 8 days (range 6–13 days). There was no perioperative complication and patient mortality in this series. The resected margins of the specimens were tumor free (R0 resections, range 0.1–1.2 cm). The mean follow-up period was 56 months (range 12.9–93.7 months). No patient died during the follow-up period.
Conclusions:
Our experience demonstrated that laparoscopic caudate lobectomy is safe and feasible in selected patients with malignancy in the caudate lobe.
Introduction
T
Laparoscopically isolated caudate lobectomy (Couinaud's segments I and IX) is considered a particularly risky and difficult procedure due to the relationship between vascular and biliary anatomy. 2 The caudate lobe of the liver is located behind the two major lobes and is surrounded by the inferior vena cava (IVC), the three main hepatic veins, and the hepatic hilum. 3 According to Kumon's nomenclature, 4 the caudate lobe consists of three sections: the Spiegel lobe (Couinaud's segment I), the paracaval portion (Couinaud's segment IX), and the caudate process. The Spiegel lobe is located behind the lesser omentum, to the left of the Arantius ligament. The paracaval portion, which is attached to the anterior surface of the IVC by the retrohepatic ligament and the short hepatic veins, lies to the right of the Spiegel lobe. The caudate process, which is the smallest of the three sections, is a thin tongue-like projection between the IVC and the portal vein to the right of the paracaval section. The upper border of the caudate lobe extends behind the major hepatic veins.
The portal blood flow for the caudate lobe comes from both the left and the right portal systems. The hepatic arterial flow is variable, but usually comes mainly through a branch from the main left hepatic artery. Venous drainage occurs along the posterior aspect of the caudate lobe directly into the IVC through multiple short hepatic veins. Biliary drainage is also variable, but predominantly occurs through the left hepatic duct.
Only case reports or a few case series have been described regarding laparoscopic caudate lobectomy.5–7 We herein describe our procedure for isolated laparoscopic caudate lobectomy in patients with malignancies and evaluated its safety and feasibility.
Patients and Methods
Between September 2007 and May 2014, 6 consecutive patients, including 4 cases of hepatocellular carcinoma (HCC), 1 case of cholangiocarcinoma, and 1 case of metastatic ovarian cancer, underwent laparoscopic caudate lobectomy. According to the Balliol classification scheme of IDEAL recommendation, the procedure was categorized as stage II. 8 Patients were informed of the innovative nature of the procedure, and consent was obtained before surgery. All operations were performed by consultant surgeons with experience in both advanced laparoscopic techniques and open liver surgery. Clinical characteristics and postoperative parameters of the patients including complications, length of hospital stay, and outcomes were assessed retrospectively until May 2015.
Operative procedure
The patient was placed in a modified lithotomy position after general anesthesia. The chief surgeon stood between the patient's legs, while an assistant surgeon stood on the left side of the patient. The port insertion sites are shown in Figure 1. Intraabdominal pressure (IAP) was maintained at 11 mmHg. After dissecting the round and falciform ligament of the liver, intraoperative ultrasonography was performed to confirm the locations of the tumor and the main vasculatures. The left liver portion was retracted upward and the lesser omentum was excised to expose the caudate lobe. The dissection was carried out from the caudal to the cranial side and from the left to the right side. Initially, the left caudal branches of the portal vein were divided followed by the division of short hepatic veins lying on the dorsal side to free Spiegel lobe from IVC (Fig. 2). Left caval ligament was divided to better expose the upper area of the IVC. The left boundary of the caudate lobe was the Arantius ligament. Transection along the Arantius ligament was performed to the cranial side and to the right direction. When approaching the right side, the anterior border of the resection plane was the posterior Glissonean pedicle. All portal branches from the posterior pedicle to the caudate process were exposed and ligated. The transection was carried out up to the cranial border, which was the confluence of the right hepatic vein (RHV) into the IVC. The transection of the liver parenchyma was performed with energy devices and an ultrasonic surgical aspirator as well as clipping of small vasculatures larger than 2 mm. During transection, all portal branches and short hepatic veins were carefully divided using clips; however, automated suturing devices were used during transection of the Glissonean pedicle and the hepatic vein root when necessary (Fig. 3). Liver transection proceeded cranially along the dorsal surface of the RHV and middle hepatic vein (MHV). When the dorsal plane of the liver between the RHV and MHV was transected, the laparoscopic caudate lobectomy was considered to be complete (Fig. 4). The resection surface was meticulously checked for biliary leakage and bleeding. The specimen was retrieved through the infraumbilical port site (Fig. 1).
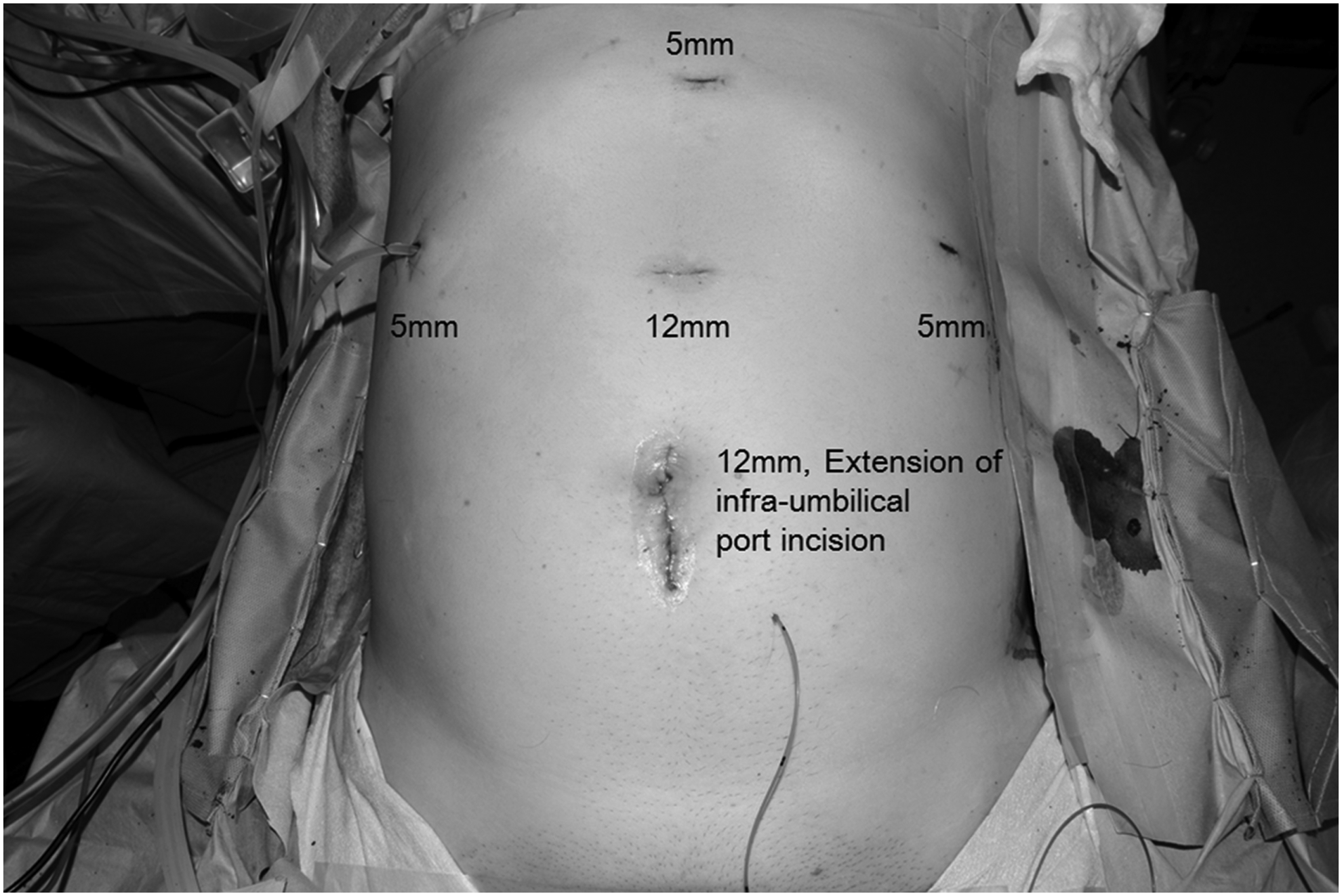
Port position for laparoscopic caudate lobectomy.

Transection of the caudal branches from the portal vein by an automated suture device.

Transection of the short hepatic vein.
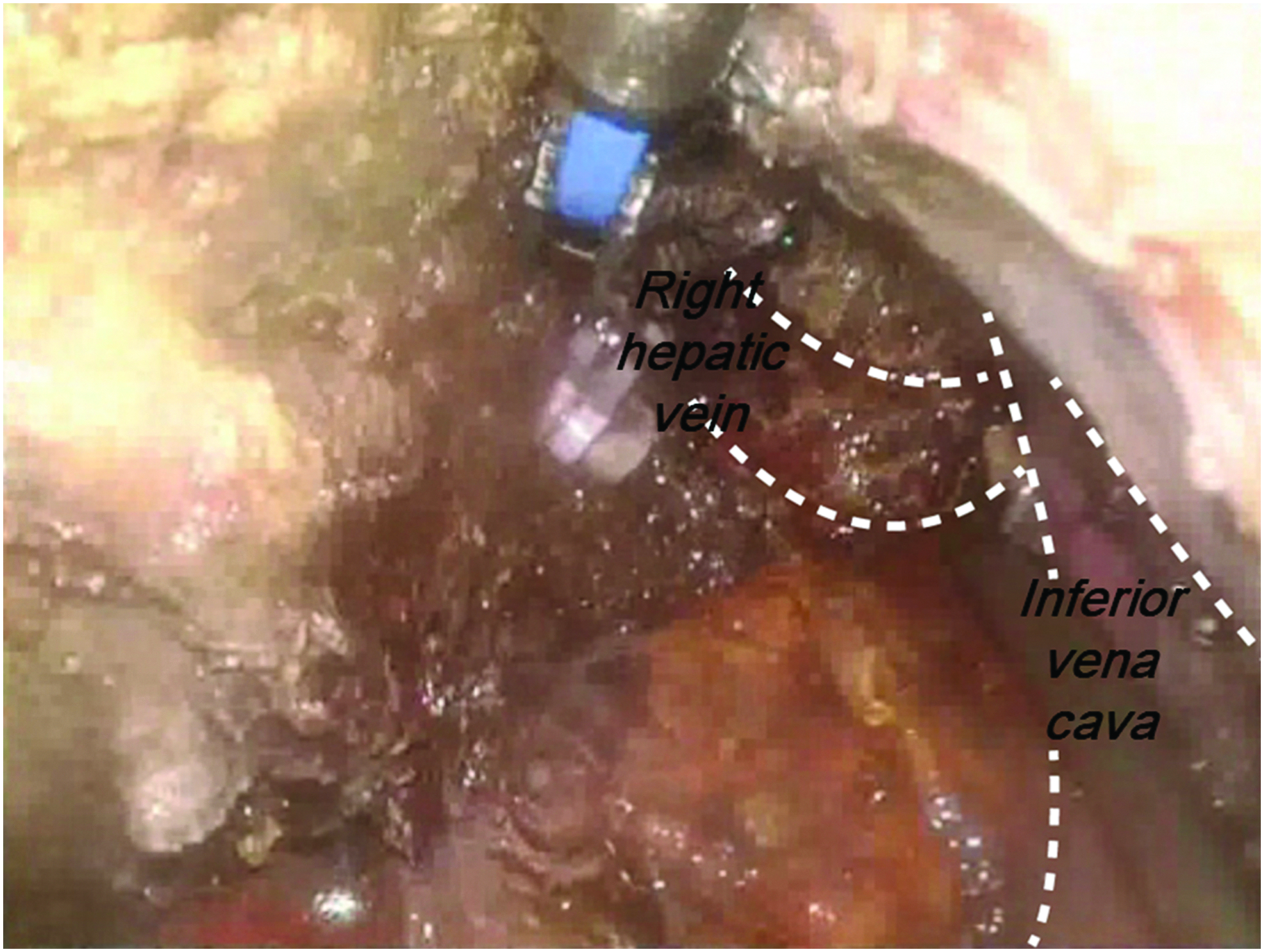
Liver transection along the dorsal surface of the right and middle hepatic veins.
Results
All patients had preserved liver function and were Child A. All patients underwent complete caudate lobectomy except for 1 patient who underwent partial caudate lobectomy for a HCC in the Spiegel lobe. Clinical and pathological characteristics of the patients are summarized in Table 1. The perioperative data and follow-up outcomes are summarized in Table 2. The total operation time ranged from 168 to 615 minutes, with a median time of 382 minutes. Patient 1 needed simultaneous laparoscopic radical subtotal gastrectomy due to an advanced gastric cancer that took 458 minutes to complete the operation. Patient 5 had undergone laparoscopic total abdominal hysterectomy with bilateral salpingo-oophorectomy 2 years earlier for ovarian cancer. She had metastatic ovarian cancer at the caudate lobe and intraperitoneal metastasis. She underwent simultaneous intraperitoneal debulking surgery, which took 615 minutes to perform. The estimated blood loss ranged from 120 to 360 mL, and no blood transfusions were required. No signs of hemodynamic instability during operation were observed. There was no case of open conversion.
AFP, alpha-fetoprotein; Alb, albumin; CCC, cholangiocarcinoma; HCC, hepatocellular carcinoma; ICG R15, retention rate of indocyanine green 15 minutes after administration; INR, international normalized ratio; T.bil, total bilirubin.
C, caudate process; co-op, combined operation; EBL, estimated blood loss; P, paracaval portion; RSTG, radical subtotal gastrectomy; S, Spiegel lobe.
Postoperative courses were uneventful for all patients. All patients were able to tolerate liquids on the second postoperative day, and no biliary complications were encountered. The median follow-up period was 56 months (range 12.9–93.7 months). Recurrence occurred in 2 out of 4 HCC patients (patients 1 and 2). Both recurrences occurred at segment 8 of the liver at 10 and 55 months postoperative, respectively. The patients received transarterial chemoembolization and radio frequency ablation for the recurred lesions, respectively.
Patient 4 was diagnosed with a ruptured pyogenic abscess of the caudate lobe before the operation, but on final pathology analysis, it was confirmed as a ruptured cholangiocarcinoma. Nine months after operation, she was diagnosed with carcinomatosis by laparoscopic biopsy. Patients 4 and 5 received systemic chemotherapy. No patient died during the follow-up period.
Discussion
Since the first report of LLR in 1992, 9 laparoscopic caudate lobectomy is still considered a surgical challenge and is rarely performed due to its deep location close to major vasculatures.2,5,6 Our results were comparable with other report series, and we also had shown that the laparoscopic caudate lobectomy could be performed without complications. Precise dissection and efficient hemostasis during caudate lobectomy are crucial due to the proximity of the major vasculatures. Cavitron Ultrasonic Surgical Aspirator and/or an ultrasonic device with bipolar electrocautery are essential for meticulous parenchymal transection. Unlike the open method, during laparoscopic surgery, clear visual image can be better exposed by illumination and additional magnification. Also by using flexible scope, various approaching angles are easily obtained, which further improves the quality of the operation. The IAP is usually maintained at a minimum of 11 mmHg, which is the lowest pressure at which a clear view can be obtained while minimizing the risk of hemodynamic complications. However, if there is bleeding from hepatic veins or the IVC, the IAP can be temporarily raised up to 15 mmHg so that the IAP is balanced with the central venous pressure and the bleeding can be controlled.
Another benefit for laparoscopic caudate lobectomy is that only a small incision is necessary to retrieve the specimen. When caudate lobectomy is performed using the open method, a 20 to 30 cm incision is required to obtain an adequate operative field. However, in LLR for the caudate lobe, extension of the infraumbilical incision to the size of the specimen is sufficient to retrieve the specimen. This length is usually less than 5 cm. According to our study, although it was a relatively small case series, the laparoscopically isolated caudate lobectomy seems to be a safe and feasible procedure. Further investigations with a larger number of patients are warranted to confirm these results.
Conclusions
Laparoscopically isolated caudate lobectomy appears to be a safe and feasible procedure. Thus, laparoscopically isolated caudate lobectomy is an attractive alternative to open hepatectomy. However, this procedure requires extensive experience in both laparoscopic surgery and open liver resection.
Footnotes
Disclosure Statement
Dr. Kwon is a consultant for Novartis, Ethicon, Medtronics and Olympus. For all other authors no financial interests exist.