
Abstract
Abstract
Introduction:
Few studies have assessed the impact of obesity on laparoscopic cholecystectomy (LC) in pediatric patients.
Materials and Methods:
Children who underwent LC were identified from the 2012 to 2013 American College of Surgeons' National Surgical Quality Improvement Program Pediatrics data. Patient characteristics, operative details, and outcomes were compared. Multivariable logistic regression was utilized to identify predictors of increased operative time (OT) and duration of anesthesia (DOAn).
Results:
In total, 1757 patients were identified. Due to low rates of obesity in children <9 years old, analyses were limited to those 9–17 (n = 1611, 43% obese). Among obese children, 80.6% were girls. A higher proportion of obese patients had diabetes (3.0% versus 1.0%, P < .01) and contaminated or dirty/infected wounds (15.1% versus 9.4%, P < .01). Complication rates were low. The most frequent indications for surgery were cholelithiasis/biliary colic (34.3%), chronic cholecystitis (26.9%), and biliary dyskinesia (18.2%). On multivariable analysis, obesity was an independent predictor of OT >90 (odds ratio [OR] 2.02; 95% confidence interval [95% CI] 1.55–2.63), and DOAn >140 minutes (OR 1.86; 95% CI 1.42–2.43).
Conclusions:
Obesity is an independent risk factor for increased OT in children undergoing LC. Pediatric surgeons and anesthesiologists should be prepared for the technical and physiological challenges that obesity may pose in this patient population.
Introduction
I
In adults, obesity has been reported to increase operative time (OT),13–20 postoperative length of stay (LOS), 15 and rates of surgical site infections (SSIs).13,15,17 To date, only two, single-center experiences have been published on the relationship between obesity and LC in pediatric patients.6,21 Garey et al. 6 found that 31% of 312 American children undergoing LC at their institution were obese but that there were no differences in OT, LOS, or postoperative complications between this group and normal-weight patients. Similarly, Kiuru et al. 21 found no difference in OT or LOS between low and high body mass index (BMI) groups in a cohort of 59 Finnish children.
Given that these studies had smaller sample sizes, were illustrative of single institutions, and utilized different definitions of obesity, we believe that a larger, broader, and more standardized assessment is necessary. Therefore, we evaluated a large, multi-center database to evaluate the differences in patient characteristics and perioperative outcomes of obese and nonobese children undergoing LC.
Materials and Methods
The American College of Surgeons' National Surgical Quality Improvement Program Pediatric (ACS-NSQIP-P) 2012 to 2013 data were queried for children aged 2–17 years who underwent LC. The ACS-NSQIP-P collects preoperative risk factors, intraoperative variables, and 30-day mortality and morbidity outcomes for children aged 2–17 undergoing major inpatient or outpatient surgical procedures at all ACS-NSQIP-P participating centers. In 2013, 63,387 cases were included from 56 participating sites. 22
Patients were classified as overweight and obese based on sex and age-adjusted BMI ≥ the 85th and 95th percentiles, respectively, as defined by the Centers for Disease Control and Prevention (CDC). 23 Children with missing BMI values (n = 224), those with BMI in the 1st (n = 20) and 99th (n = 22) percentiles, those undergoing concurrent procedures (n = 237), those with primary postoperative diagnoses unrelated to the gallbladder (n = 5), and patients with severe comorbidities (n = 205) such as ventilator dependence and need for dialysis were excluded. Patient characteristics (sex, age, American Society of Anesthesiologists (ASA) status, etiology leading to LC) and operative details (OT, duration of anesthesia [DOAn], case type) were extracted. Cases with OT <30 minutes (n = 37) and DOAn <40 minutes (n = 8) were not included in the final analysis. Etiologies requiring LC were classified as cholelithiasis/biliary colic, biliary dyskinesia, acute cholecystitis, and chronic cholecystitis. Other etiologies including hematologic disorders, choledocholithiasis/common bile duct pathologies, congenital disorders, and pancreatic pathology (<50 cases each) were combined to create a category labeled “other.”
Univariate analysis (using Wilcoxon rank sum, Student's t-test, Pearson's chi-square, and Fisher's exact tests for significance) comparing obese and nonobese children was initially utilized to assess available outcome measures including OT, DOAn, SSI, need for transfusion, readmission, and unplanned reoperation. A P-value <.05 was considered statistically significant.
Multivariable logistic regression models were then constructed to assess for independent predictors of OT and DOAn by using patient and operative covariates. Operative time and DOAn were assessed as binary variables, by using approximately the 75th percentile as a cutoff. A sensitivity analysis was performed to assess the effect of excluding cases with OT <30 minutes or DOAn <40 minutes. Statistical analyses were performed by using SAS (SAS version 9.3; SAS Institute, Inc., Cary, NC, USA, 2010). This study was exempt from institutional review board review due to the use of publicly available, de-identified data.
Results
In total, 1757 LC patients were identified; 725 (41.3%) were obese. Due to low rates of obesity in children less than 9 years of age (Fig. 1), further analyses were limited to those 9–17 (n = 1611, 43.2% obese). Patient and operative characteristics are summarized in Tables 1 and 2, respectively. Among obese children, 80.6% were girls and 19.4% were boys. More obese patients had diabetes (3.0% versus 1.0%, P < .01) and contaminated or dirty/infected wounds (15.1% versus 9.4%, P < .01). Hematologic disorders and need for blood transfusion preoperatively were more common in nonobese children (both P < .01). The most frequent indications for surgery were cholelithiasis/biliary colic (34.3%), chronic cholecystitis (26.9%), and biliary dyskinesia (18.2%).
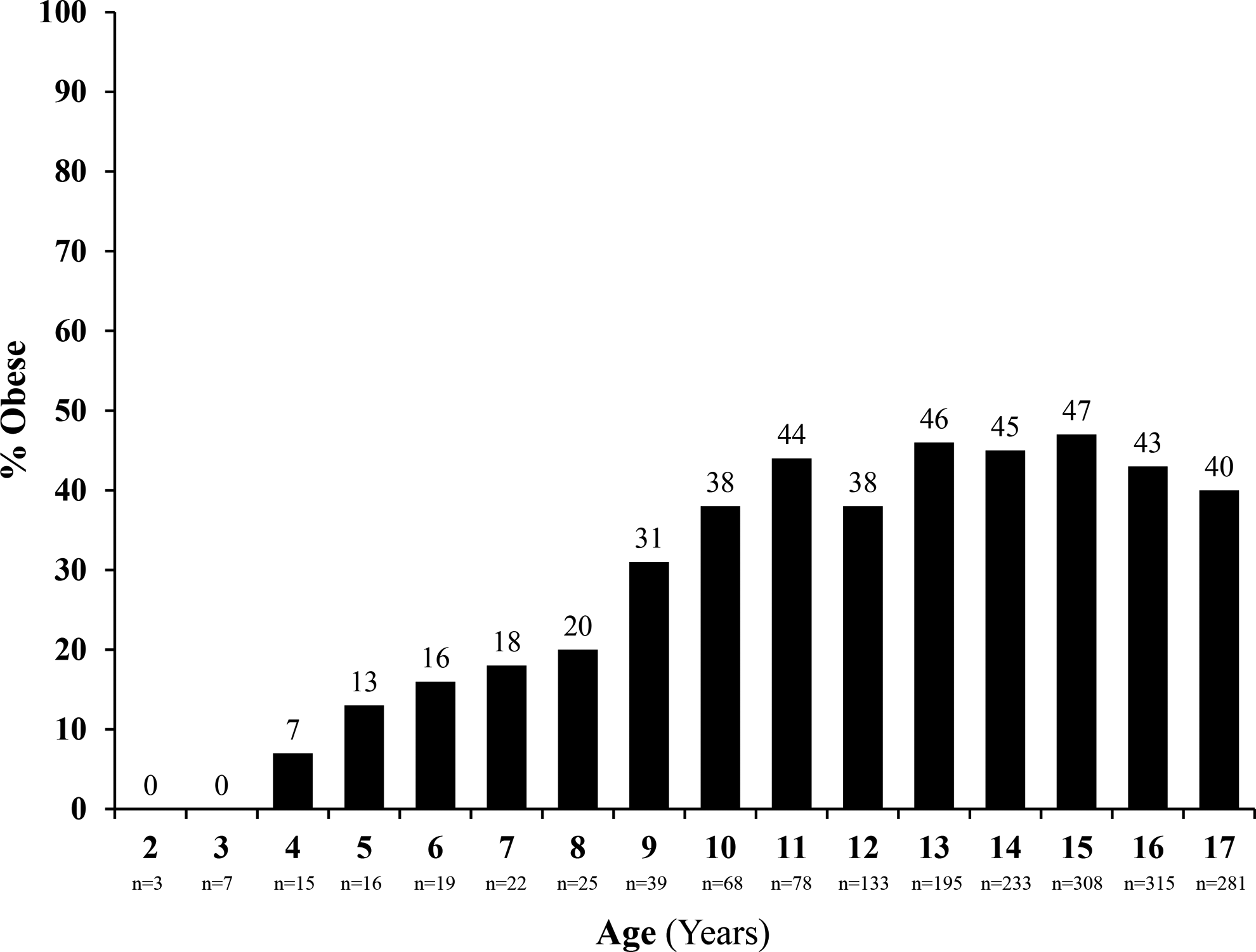
Proportion obese by age.
ASA, American Society of Anesthesiologists; BMI, body mass index; IQR, interquartile range.
BMI, body mass index; IQR, interquartile range; SD, standard deviation.
Obese children had extended anesthesia duration (median 124 versus 110 minutes, P < .01) and longer OT (median 78 versus 66 minutes, P < .01). Nonobese patients required intraoperative or postoperative transfusion (≤72 hours from surgery) more frequently (0.7% versus 0%, P = .04). Obese children also had a higher rate of SSI, although only marginally statistically significant (1.4% versus 0.4%, P = .054). Length of hospital stay, 30-day rates of readmission, and unplanned reoperation were similar for both groups (all P > .05).
On multivariable analysis (refer to Table 3), obesity (versus nonobese), age increase per 1 year, non-white non–African American race (versus white), and diagnosis of biliary dyskinesia (versus cholelithiasis/biliary colic) were independent predictors of OT >90 minutes and DOAn >140 minutes. Concordance statistics for the multivariable models were found to be 0.69 for OT and 0.67 for DOAn. Interestingly, overweight (BMI ≥85th percentile and <95th percentile) children did not have higher odds of having longer OT or DOAn compared with obese and normal-weight (<85th percentile) children, when adjusted for the same patient and operative characteristics. No differences in the aforementioned analysis were found in a sensitivity analysis, which included cases with OT <30 minutes or DOAn <40 minutes.
Chosen to approximate the 75th percentile.
C statistics: 0.69 for operative time and 0.67 for duration of anesthesia.
95% CI, 95% confidence interval; ASA, American Society of Anesthesiologists; BMI, body mass index; OR, odds ratio.
Discussion
To our knowledge, this study is the largest, multi-center pediatric LC study to date and it utilizes the currently recommended CDC definition of obesity for American children aged 2–19. 24 In our analysis, we demonstrate that nearly half of the children undergoing LC are obese, which is higher than the rates of obesity reported nationwide in this age group. 1 Although the overall rate of 30-day complications was low, we found that obesity was an independent predictor of increased OT and DOAn. In addition, children who were obese had higher rates of SSI. This is in contrast to previous smaller studies published in the pediatric literature that showed that LC outcome was not dependent on obesity.6,21 This difference is likely explained by varying definitions of obesity and sample size in those studies. The adult literature also attests to increased OT in laparoscopic surgery due to obesity, but other perioperative morbidities and complications are described with less consistency and homogeneity.13–20,25
Our findings that obesity is an independent predictor of increased OT and DOAn has multiple important patient and healthcare implications. Increased OT is a known risk factor for postoperative wound infections.26–29 Although our overall rate of SSI was low, and the difference in median OT between obese and nonobese children was only 12 minutes, the obese group did have a higher SSI rate. This may be explained by the longer OT itself, underlying physiological predisposition toward infection inherent to obesity, 30 or our data suggesting that obese patients had a higher rate of contaminated or dirty/infected wounds.
Increased OT and DOAn affect the workload of both surgeons and anesthesiologists. Longer times spent in the operating room equate to decreased case volume and less time for these medical professionals to participate in their myriad of daily responsibilities. In addition, the majority of LC in children are performed by pediatric surgeons, who are in high demand but low in supply. 31 Increasing case volume demands due to longer OT and DOAn, combined with a lack of surgeon resources, is a difficult problem that would potentially have a significant impact on pediatric healthcare in this country.
Although some may dispute that an increase in OT by 12 minutes and DOAn by 14 minutes is not clinically meaningful, we would disagree. At our institution, the cost of the operating room is estimated to be ∼$42 per minute (includes anesthesia and facility fees). 32 Therefore, a 14-minute longer period of anesthesia (our median increase in DOAn) in an obese child equates to an additional cost of $588. Furthermore, elective day-case LC is known to be safe and is becoming more common in children. 33 In this setting, delays of 10+ minutes for a case may impact subsequent cases in the day and lead to unnecessary hospital admissions.
It is possible that risk factors for obesity such as a sedentary lifestyle34,35 can negatively affect an individual's cardiopulmonary fitness, and as a result, potentially lead to problems with mechanical ventilation or oxygenation and, subsequently, increase DOAn. In addition, there are a few reasons that explain how obesity may directly increase OT and DOAn. Increasing BMI has been shown to predict more challenging intubations (due to difficult visualization of the vocal cords) 36 and to prolong recovery time after discontinuation of general anesthesia. 37 The specific reason for the latter finding is unknown, but it may be related to differences in metabolism of anesthetics in the setting of increased adiposity. From a technical operative standpoint, laparoscopic access may be more difficult in larger patients due to a thicker abdominal wall. Visualization intracorporeally may be hindered by fatty omentum, liver, or tissue planes. In addition, after the procedure is completed, closure of the fascia through minimal access port sites in a thick abdominal wall can be challenging. Collectively, all these issues may increase OT and SSI occurrence.
Our study is limited by the procedure-specific nature of the ACS-NSQIP-P database and the intrinsic limitations of retrospective databases. Outcomes are limited only to 30 days, and, therefore, our cohort may underestimate the true rate of SSI. The dataset does not include preoperative information regarding symptoms and therefore, timing (other than procedure urgency) of the operation could not be analyzed. Finally, the severity of the disease state is not captured and, therefore, not factored into analysis. For example, all patients with acute cholecystitis were included together; however, the magnitude of the inflammatory response in one case may be worse than another, which increases the technical difficulty and, subsequently, the OT. Despite these limitations, we believe that our study provides the literature with a more standardized and robust assessment of the effect of obesity on LC in children.
In this large, multi-center database study, we found that obesity is an independent risk factor for increased OT and DOAn for children undergoing LC. Common surgical indications in this cohort include cholelithiasis, chronic cholecystitis, and biliary dyskinesia. Overall complication rates for LC were low, but SSIs were more common in obese children. Pediatric surgeons and anesthesiologists should be prepared for the potential technical and physiological challenges that obesity causes in these patients. Due to previously increasing numbers of obese children, pediatric surgeons should expect a larger number of patients to require LC in the future.
Footnotes
Disclosure Statement
No competing financial interests exist.