
Abstract
Abstract
Aim:
Scoliosis, which is often associated with neurological impairment in children, sometimes makes it difficult to perform laparoscopic procedures. This study assessed the impact of scoliosis on performing laparoscopic Nissen fundoplication.
Methods:
Medical records and radiographic examinations of patients who underwent laparoscopic Nissen fundoplication at a single institution from 2006 to 2015 were reviewed retrospectively. Patients' data on age at surgery, height, weight, duration of pneumoperitoneum, and amount of bleeding were collected. The Cobb angle was measured using X-rays, and the direction (right or left) of the scoliotic curve was recorded. The chest compression ratio was calculated using computed tomography axial images.
Results:
Eighty-five patients were included and analyzed in this study, of which 89% were neurologically impaired. Median age, height, and weight were 120 months, 110 cm, and 17 kg, respectively. A positive correlation between age and the Cobb angle (ρ = 0.64) and a negative correlation between age and the chest compression ratio (ρ = −0.56) were observed. The right-curved scoliotic group showed significantly more bleeding than the nonscoliotic (<10°) group (P = .01; nonscoliotic, 0 mL; right curved, 7.5 mL; left curved, 0 mL). The severe scoliotic group (≥45°) showed more bleeding than the nonscoliotic group (P = .02). Neither the direction of the scoliotic curve nor scoliotic severity showed a significant difference in the duration of pneumoperitoneum.
Conclusions:
The older the patient, the more severe their scoliosis and chest compression were. Right-curved or severe scoliosis could be risk factors for intraoperative bleeding in laparoscopic Nissen fundoplication.
Introduction
L
Materials and Methods
The subjects were patients who underwent laparoscopic Nissen fundoplication from June 2006 to September 2015 at our institution. Medical charts, operative records, X-rays of the chest and abdomen, and computed tomography (CT) images were reviewed retrospectively by the first author. Patients' data on age at surgery, height, weight, neurological condition, duration of intraoperative pneumoperitoneum, amount of bleeding, and the procedure performed concurrently were collected. The Cobb angle was measured on preoperative X-rays using commercially available image processing software (Medical Image Analyzer; Inotech Co., Ltd., Hiroshima, Japan), and the direction (right or left) of the scoliotic curve was recorded. Scoliotic severity was classified into four groups according to the Cobb angle, that is, nonscoliotic (<10°), mild (≥10°), intermediate (≥25°, <45°), and severe (≥45°) according to the management strategy for adolescent idiopathic scoliosis. 4 Typical X-rays are shown in Figure 1. The chest compression ratio, which was introduced by Harada et al. 5 and defined as the shortest length (thickness) of the thoracic cavity divided by the longest length (width) of the thoracic cavity at the level of the lower end of the sternum, was calculated on CT axial images using the software (Fig. 2).
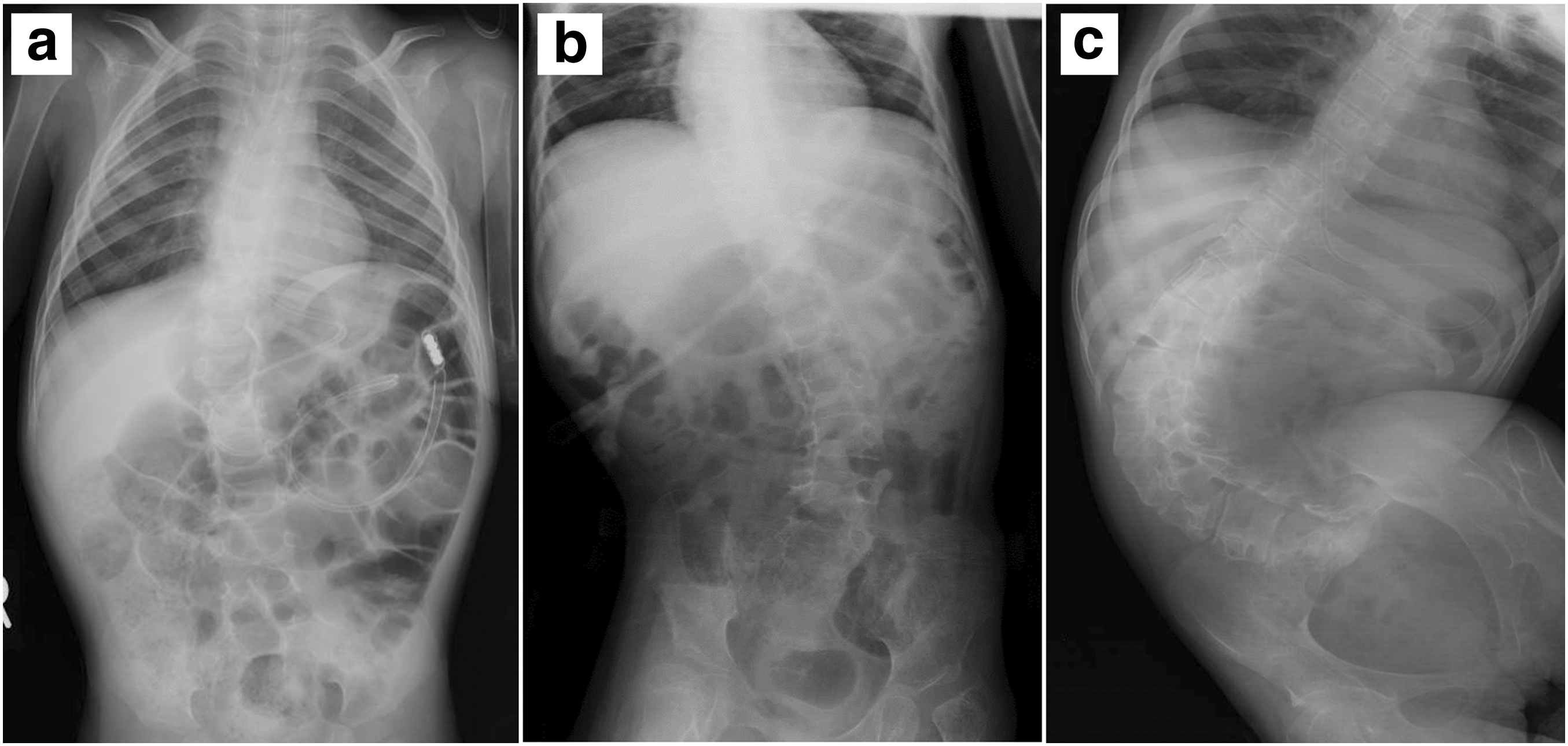
Typical X-rays of scoliotic patients.

Calculation of the chest compression ratio. The shortest length (thickness; short two-headed arrow) of the thoracic cavity is divided by the longest length (width; long two-headed arrow) of the thoracic cavity at the level of the lower end of the sternum.
All procedures were supervised by a board-certified pediatric surgeon qualified by the Endoscopic Surgical Skill Qualification system, which was developed by the Japan Society for Endoscopic Surgery. 6 Our procedure was a Standard Nissen fundoplication with a loose and short wrap, similar to the method described by Rothenberg, 7 and fixation of the wrap to the diaphragm was added depending on the case. The first trocar was placed using the open Hasson technique, and four or five ports were used depending on whether there was a need to elevate the left lobe of the liver.
Statistical analysis was performed by the Steel–Dwass method for nonparametric multiple comparisons, Fisher's exact test for contingency tables, and Spearman's rank correlation coefficient for identifying the strength of associations between two variables using commercially available software (JMP® Pro 11.0.0; SAS Institute Japan Ltd., Tokyo, Japan). P values less than .05 were considered to be statistically significant. All data are shown as median (interquartile range) values.
This retrospective observational study was approved by the Research Ethics Committee of the Graduate School of Medicine and Faculty of Medicine, The University of Tokyo (protocol no. 2996-1).
Results
Laparoscopic fundoplication was attempted in 86 patients during the study period. Only one case, which had previously undergone surgery for omphalocele, was converted to laparotomy immediately after insertion of the scope due to the presence of dense intra-abdominal adhesions, and this case was excluded from the analyses. Seventy-six (89%) of the remaining 85 patients were neurologically impaired. Their age, height, and weight were 120 (29.5–211.5) months, 110 (81.6–133.5) cm, and 16.6 (9.0–23.8) kg, respectively. The duration of intraoperative pneumoperitoneum was 184 (144–220) minutes, and the amount of bleeding was 0 (0–30) mL.
As for the patients' physical features, 24 showed no scoliosis (<10°), and there were 23 right-curved and 38 left-curved scoliotic patients. Among the 61 scoliotic patients, 12, 15, and 34 were classified into mild, moderate, and severe scoliosis, respectively. In the analysis of 85 patients, a positive correlation was seen between age and the Cobb angle (Fig. 3; ρ = 0.68; P < .01). The chest compression ratio was calculated in 77 patients with the exception of 8 patients, in whom a preoperative CT scan was not performed, and the ratio was 0.56 (0.50–0.67). A negative correlation was seen between age and the chest compression ratio (Fig. 4; ρ = −0.56; P < .01).
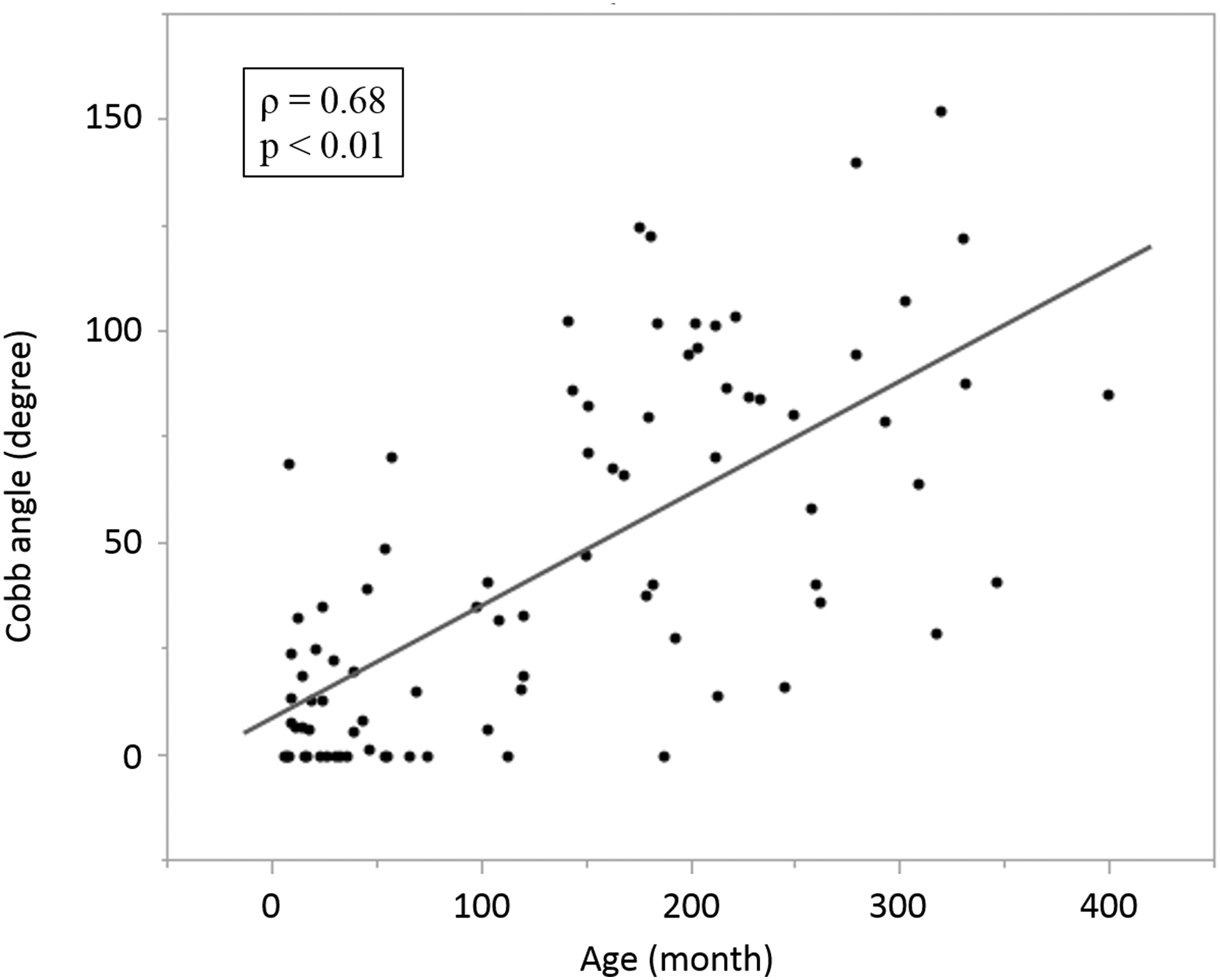
Relationship between age and scoliotic severity (Cobb angle). A positive correlation was seen between age and the Cobb angle.
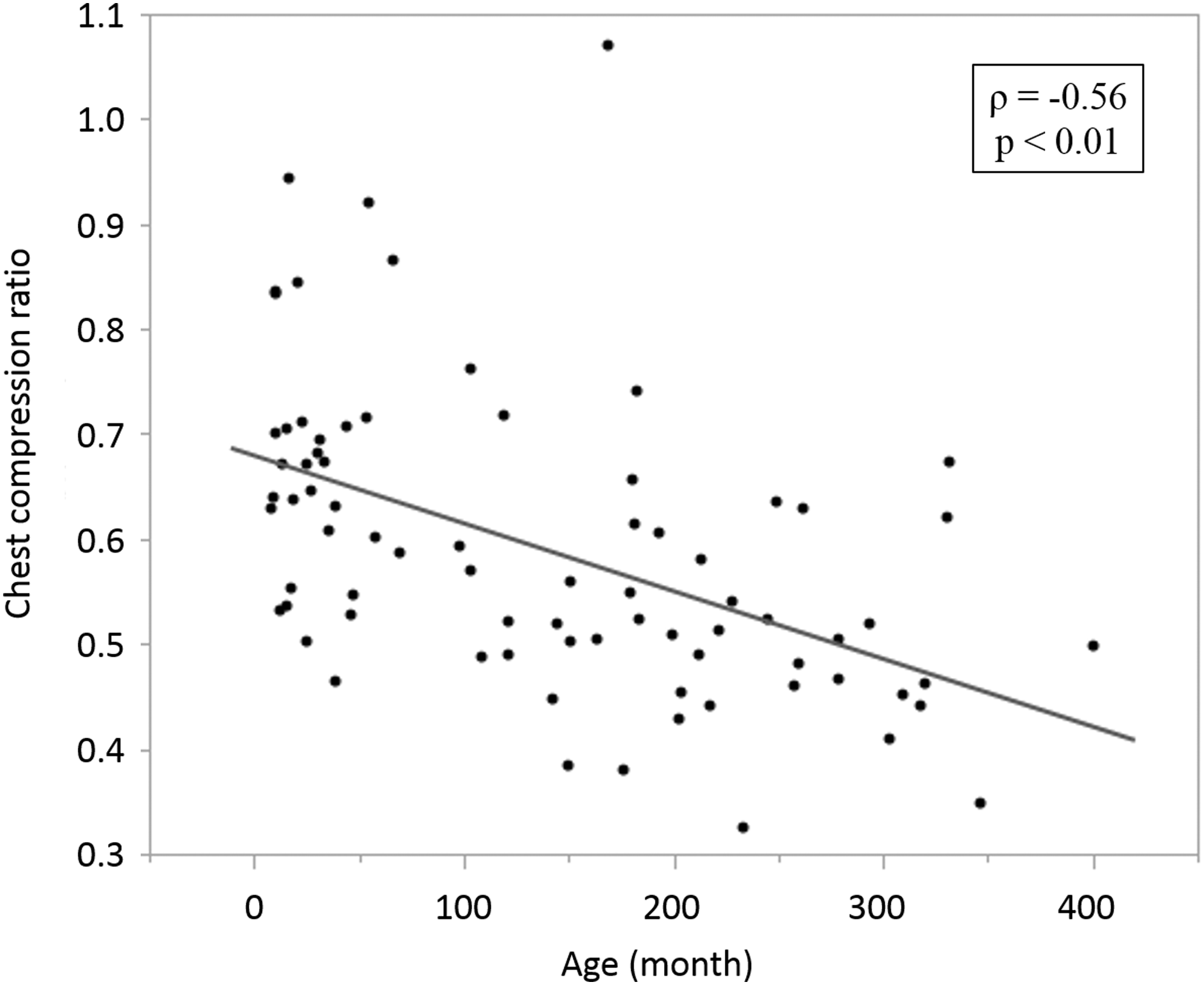
Relationship between age and chest compression ratio. A negative correlation was seen between age and the chest compression ratio.
As for the simultaneously performed procedure, gastrostomy tube (G-tube) placement was the most frequent (76 cases; 91%), and an intervention to the trachea, including tracheotomy, tracheoesophageal diversion, and laryngotracheal separation, was the second most frequent (12 cases; 14%). The ratio of patients with concurrent G-tube placement was not significantly different among the groups classified according to scoliotic curve (P = .17; nonscoliotic, 20 [83%]; right curved, 23 [100%]; left curved, 34 cases [89%]), as well as among the groups classified according to scoliotic severity (P = .57; nonscoliotic, 20 [83%]; mild, 11 [92%]; intermediate, 14 [93%]; severe, 32 cases [94%]). The ratio of patients in whom tracheal intervention was performed was also not significantly different according to scoliotic curve (P = .68; nonscoliotic, 2 [8.3%]; right curved, 4 [17.4%]; left curved, 6 cases [15.8%]) and scoliotic severity (P = .61; nonscoliotic, 2 [8.3%]; mild, 1 [8.3%]; intermediate, 2 [13.3%]; severe, 7 cases [20.6%]).
Upon comparison according to the direction of the scoliotic curve, the right-curved group showed significantly more bleeding than the nonscoliotic (<10°) group (Fig. 5; P = .01; nonscoliotic, 0 [0–0] mL; right curved, 7.5 [0–81.3] mL; left curved, 0 [0–40] mL). Upon comparison according to scoliotic severity, significantly more bleeding was seen in the severe group than in the nonscoliotic group (Fig. 6; P = .02; nonscoliotic, 0 [0–0] mL; mild, 0 [0–37.5] mL; intermediate, 0 [0–32.5] mL; severe, 7.5 [0–62.5] mL). Only one patient in the nonscoliotic group required a blood transfusion as a total of 300 mL bleeding was seen due to injury of the short gastric artery. With regard to the duration of pneumoperitoneum, neither the direction of the scoliotic curve (nonscoliotic, 183 [134–211] minutes; right curved, 173 [142–215] minutes; left curved, 190 [155–229] minutes) nor scoliotic severity (nonscoliotic, 183 [134–211] minutes; mild, 168 [134–199] minutes; intermediate, 169 [142–232] minutes; severe, 189 [156–229] minutes) showed a statistically significant difference among the groups.
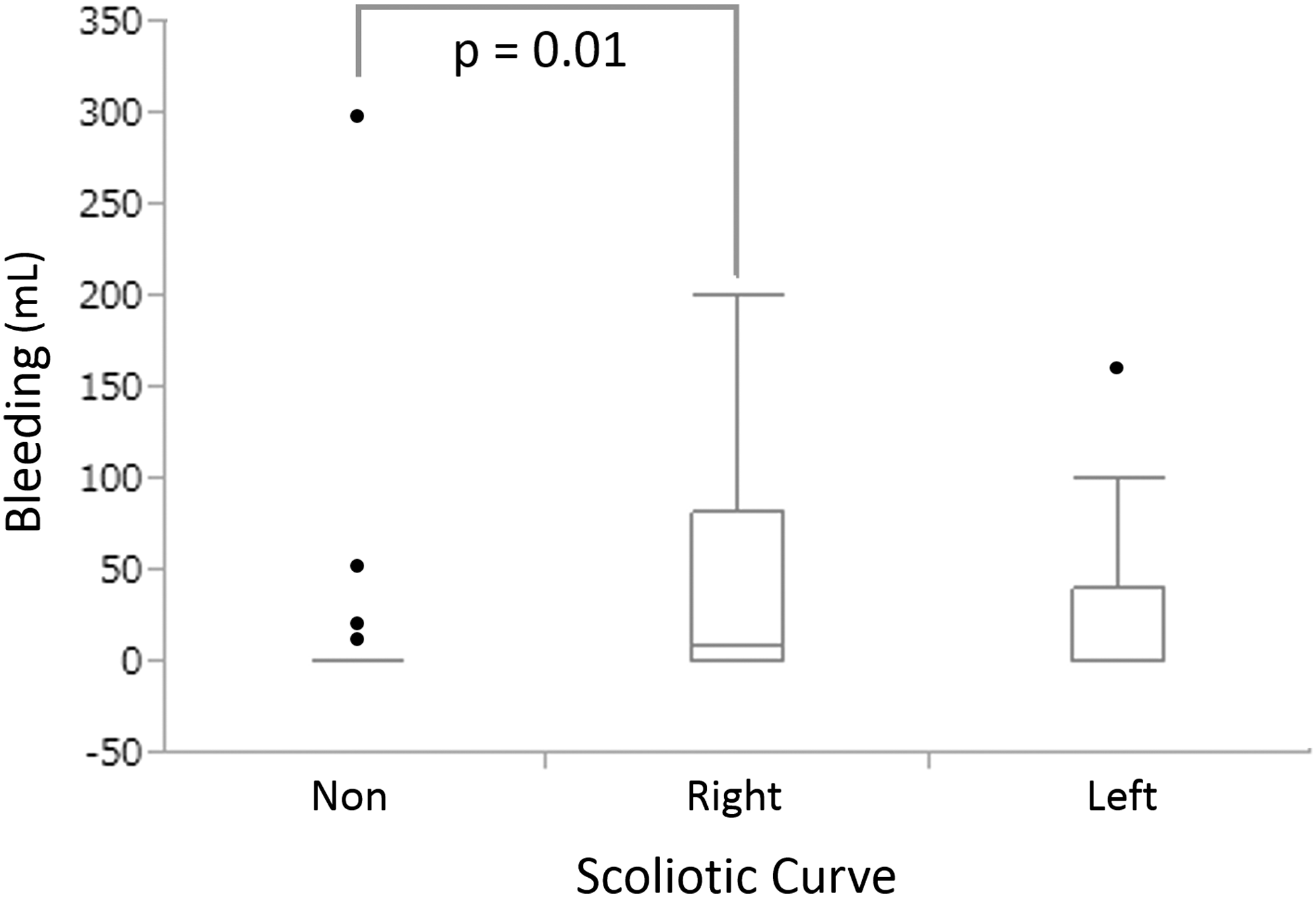
Bleeding compared by the direction of scoliotic curve. The right-curved group showed significantly more bleeding than the nonscoliotic group (P = .01).

Bleeding compared by scoliotic severity. The severe group showed significantly more bleeding than the nonscoliotic group (P = .02).
Discussion
Surgeons seem to acknowledge empirically that laparoscopic procedures are often difficult in scoliotic patients, but there are no available data regarding the impact of scoliosis on their performance. This retrospective study investigated the relationships between the typical physical features of neurologically impaired children, such as scoliosis, and difficulty in performing laparoscopic Nissen fundoplication and showed the possibility of intraoperative bleeding in right-curved or severe scoliotic patients.
The difficulties in performing a laparoscopic procedure were evaluated objectively using the duration of intraoperative pneumoperitoneum and the amount of bleeding. We used pneumoperitoneum time and not operative time because the majority of patients underwent additional procedures, such as G-tube placement and/or tracheal intervention, and it was difficult to extract reliable information for the duration of the laparoscopic procedure from anesthetic records. Similarly, it was also difficult to distinguish the amount of bleeding during fundoplication and that of the adjunctive procedure. However, there were no significant differences in the ratios of patients in whom G-tube placement or tracheal intervention was performed simultaneously among the groups classified according to scoliotic direction or scoliotic severity. Therefore, the effect of the adjunctive procedures was minimized.
Our observational study showed that laparoscopic Nissen fundoplication in right-curved or severe scoliotic patient is more difficult than in normal, left-curved or nonsevere scoliotic patients as there is an increased risk of bleeding. We hypothesized that it is more difficult for surgeons to perform a laparoscopic procedure on left-curved patients and they showed more bleeding and had a longer pneumoperitoneum time as the working space of these patients seemed to be smaller compared with right-curved scoliotic patients. The reason for the increased risk of bleeding in right-curved patients is unclear, but we did not measure the actual intra-abdominal volume, and scoliosis is a three-dimensional deformity of the spine. If we had measured the volume of the operative field or evaluated the patients' physical features using other items in consideration of lordosis or kyphosis, the results might have been different. A clinical association between kyphoscoliosis and the development and progression of a paraesophageal hernia has been suggested, 2 and rotation of the hiatus has also been observed in severely scoliotic patients. 3 The size of the enlarged hiatus, the degree of its rotation, and the depth of the gastroesophageal junction might also contribute to the difficulty in performing laparoscopic Nissen fundoplication in such patients.
Our study showed that scoliotic severity progresses as patients grow. The prevalence of scoliosis in the adult population ranges from 1.4% to 15% in the literature and increases with age.2,8 The tendency was similar in our study population, but the incidence was quite different. Scoliosis is seen more frequently in neurologically impaired children, and only 24 patients (28%) were classified into the nonscoliotic group at the time of antireflux surgery. However, these children also might suffer from scoliosis in the future, given its high incidence in these patients.
As for chest compression, it also becomes more severe as patients age. Harada et al. reported that the mean (standard deviation) chest compression ratios for normal adults and neurologically impaired patients were 0.72 (0.06) and 0.64 (0.08), respectively, 5 and our patients developed more severe chest compression (0.56). Both scoliosis and chest compression worsen with age and these factors seem to limit the working space more severely in older patients than in younger patients.
This study has a few limitations that merit consideration. The sample size was not large, and the data were collected retrospectively. In addition, various surgeons performed the procedures, although they were always supervised by an expert. These issues could result in a bias in our data and findings.
Despite these limitations, the current study revealed that the older the patient, the more severe their scoliosis and chest compression were. Moreover, although the direction and severity of scoliosis did not affect the procedure time, right-curved or severe scoliosis could be risk factors for intraoperative bleeding in laparoscopic Nissen fundoplication. Preoperative understanding of these risks is quite useful for surgeons to avoid such morbidity.
Footnotes
Disclosure Statement
No competing financial interests exist.