
Abstract
Abstract
Background:
Current literature on chronic groin pain suggests that laparoscopic mesh repair on athletes enables a faster recovery and subsequent return to unrestricted athletic activities. The aim of this study was to evaluate the role of transabdominal preperitoneal (TAPP) mesh repair in athletes resistant to conservative therapy.
Methods:
A multidisciplinary approach with tailored physiotherapy. Thirty-nine professional athletes with chronic groin pain were referred to surgery at a single clinic. A full assessment was carried out on each, including medical history, physical examination, dynamic ultrasound, and pelvic magnetic resonance imaging. TAPP repair was performed using a polypropylene mesh and fibrin glue fixation on 30 athletes who had exhibited typical symptoms, shown resistance to conservative therapy, not benefited from accompanying physiotherapy, and had ceased training in the 3 to 6 months prior. The outcome measures were early postoperative recovery of 6 weeks and full resumption of athletic activities.
Results:
Mean duration of symptoms from onset to surgical repair was 7 months. Conservative treatment had improved symptoms temporarily or to some extent in 7 athletes, while 2 ceased competing altogether. Twenty-three athletes exhibited unilateral and 16 bilateral groin pain. Laparoscopy confirmed posterior wall deficiency in 24 and true inguinal hernia in 6 athletes. Mild scrotal hematoma occurred in 2 athletes postoperatively; all were discharged within 24 hours of surgery. Twenty-one (70%) returned to sports activities after 6 weeks of convalescence. Persistent mild pain was experienced by 5 athletes postoperatively for up to 1 year, yet did not interfere with normal daily activity. Twenty-five participants (85%) reported full satisfaction with the procedure 1 year after treatment; all returned to the same or even higher level of athletic performance.
Conclusion:
The study confirms that the endoscopic placement of retropubic mesh is an efficient, safe, and minimally invasive treatment that enables fast early recovery.
Introduction
C
Chronic groin pain is also encountered in the general population among the physically active. A proposal has thus been made to unite the terminology as pubic inguinal pain syndrome (PIPS). 6 The Manchester Consensus Conference of the British Hernia Society introduced another new term, inguinal disruption, after reaching agreement that “increased tension in the inguinal ligament” is the key to this condition. 7
SG occurs in a variety of sports and is more common among elite athletes. It may endanger an athlete's career and may even lead to early retirement from competitive sports.8–10
Currently, there is debate on whether the actual cause is weakness of the musculotendinous part of the posterior inguinal wall or rather the result of imbalance of the muscles inserting at the pubis.
On the one hand, the most common intraoperative finding in these patients is a deficiency of the posterior inguinal wall developing an imbalance between the adductors and lower abdominal musculature. The pull of the adductors in the presence of relatively under-conditioned abdominal muscles creates a shearing force across the hemipelvis, resulting in attenuation or tearing of the transversalis fascia and/or overlying musculature.3,11,12 On the other hand, the imbalanced opposing forces of the rectus/transversus abdominis muscle and the adductor longus muscle at their insertion site at, or near, the pubis, as a crossing point of kinematic forces, can cause a disruption of the muscle/tendon. This produces a weak area at the groin, the so-called “syndrome of muscle imbalance of the groin.” 13
Current literature on chronic groin pain in athletes suggests that laparoscopic mesh repair may enable a faster recovery and subsequent return to unrestricted athletic activity.14,15–21 Furthermore, a controlled clinical trial demonstrated clearly that for SG, endoscopic preperitoneal hernioplasty is more effective than nonoperative treatment. 22
The aim of this prospective clinical cohort study was to evaluate the role of transabdominal preperitoneal (TAPP) patch plasty repair in athletes with SG who have not responded to conservative therapy.
Patients and Methods
This study was initiated in December 2011 in response to growing demand among professional athletes for surgical treatment of SG that had been resistant to conservative treatment for 3 to 6 months.
Prospective study participants were referred from sports clinics, physiotherapists, and team doctors and included soccer players, runners, triathletes, and tennis players. All experienced dull diffuse pain in the groin region near the pubic tubercle that abated with rest, but typically recurred upon resumption of athletic activity.
Conservative treatment included rest; anti-inflammatory medication or corticosteroid injection; and physiotherapy, with stretching and strengthening of adductor muscles, abdominal wall muscles, iliopsoas muscles, quadriceps, and hamstrings.
A separate evaluation of patient history was performed to distinguish between SG and the more commonly occurring osteitis pubis and musculotendinous injuries.
Physical examination included palpation of bulging in the superficial inguinal ring during coughing and the Valsalva maneuver and palpation of dilatation of the external inguinal ring. The presence of hypersensitivity of the skin in the groin area and palpation pain near the pubic tubercle was also determined.
Preoperative dynamic ultrasound was performed in all athlete participants to identify inguinal canal posterior wall deficiency with anterior bulge and ballooning of the inguinal canal at the superficial inguinal ring during coughing and Valsalva maneuver.
Pelvic magnetic resonance imaging (MRI) was performed to identify other pathologies and abnormalities, but not used as a tool for deciding on operative treatment. All changes on MRI were recorded, including bone marrow edema or an increased signal at the insertion of the adductor muscle. Follow-up MRI was performed to monitor any changes in response to treatment.
All study participants received conservative treatment first, then reevaluation. TAPP repair was performed if a weak area in the groin was identified through physical examination or dynamic ultrasound.
The main intended outcomes were early postoperative recovery of 6 weeks, diminished palpation pain in the groin area, full resumption of athletic activities without pain during activity, and overall satisfaction with treatment after 1 year.
A dedicated team composed of a general surgeon, orthopedic surgeon, sport physician, and a sport physiotherapist with experience in treating groin pain supervised the study participants.
Data were collected prospectively and analyzed retrospectively.
Operative approach
Endoscopic total TAPP mesh placement was performed by an experienced single surgeon in laparoscopic surgery using a 3-trocar technique. One 12-mm blunt trocar was inserted in supraumbilical position and two 5-mm blunt trocars pararectal bilaterally.
After peritoneal incision from the anterior iliac spine to the medial umbilical plica, a thorough nontraumatic dissection from below the symphysis was performed, enabling full view of the pubic tubercle and the insertions of the conjoined tendons and abdominal rectus muscles. The retropubic space was covered with a 10 × 15 cm macroporous, polypropylene lightweight mesh (35 g/m2) and fixed with Fibrin glue. Fibrin glue is used to avoid any other potential cause of groin pain through, for example, the use of staples or tacks. The mesh was placed on the symptomatic side only (as determined by examination and imaging techniques), with wide overlay to the symphysis pubis and over the rectus abdominis muscle. After visual confirmation of correct mesh placement and Fibrin glue fixation, peritoneal closure was performed by continuous suturing with a slowly absorbable monofilament suture, and then all trocars were removed under direct vision.
Postoperative rehabilitation
Study participants resumed athletic activities 3 weeks after the TAPP procedure. A single surgeon evaluated all participants 6 weeks and 12 months postoperatively. The extent of recovery and resumption of competitive athletic activity was assessed based on time required.
Six to eight weeks of targeted physiotherapy supplemented the participants' active training program. Physiotherapy goals included improving the coordination and strength of the muscles that stabilize the pelvis, hip joints, lower abdominal muscles, and adductor muscles. Static adduction exercises, hip flexion, balance training, and exercises for core stability on a sliding board were also included.
Athletes participating in the study were not allowed to compete during physiotherapy.
Results
Of the 39 male athletes referred to our clinic, 23 (60%) presented with unilateral groin pain and 16 (40%) with bilateral symptoms. The surgical TAPP mesh repair procedure was performed on 30 athletes presenting with typical SG symptoms who had not responded to conservative therapy, had ceased training in the 3 to 6 months prior, and had received accompanying physiotherapy. Twenty-five (65%) athletes had been unable to practice their sport, while 14 (35%) had been unable to train or compete at normal levels (Table 1).
SD, standard deviation.
Pubic bone marrow edema with increased signal intensity was detected in 21 athletes (70%). In the postoperative follow-up, the presence of bone marrow edema decreased or disappeared in 10 athletes (30%) (Figs. 1 and 2). Simultaneous insertion tendinitis of the adductor longus, based on clinical diagnosis and MRI with increased signal intensity at the insertion of the adductor longus, was found in 10 athletes (30%). The presence of bone marrow edema in MRI did not correlate with time of recovery; fast early recovery and satisfaction after 12 months were the same in athletes with or without bone marrow edema in MRI (Table 2).
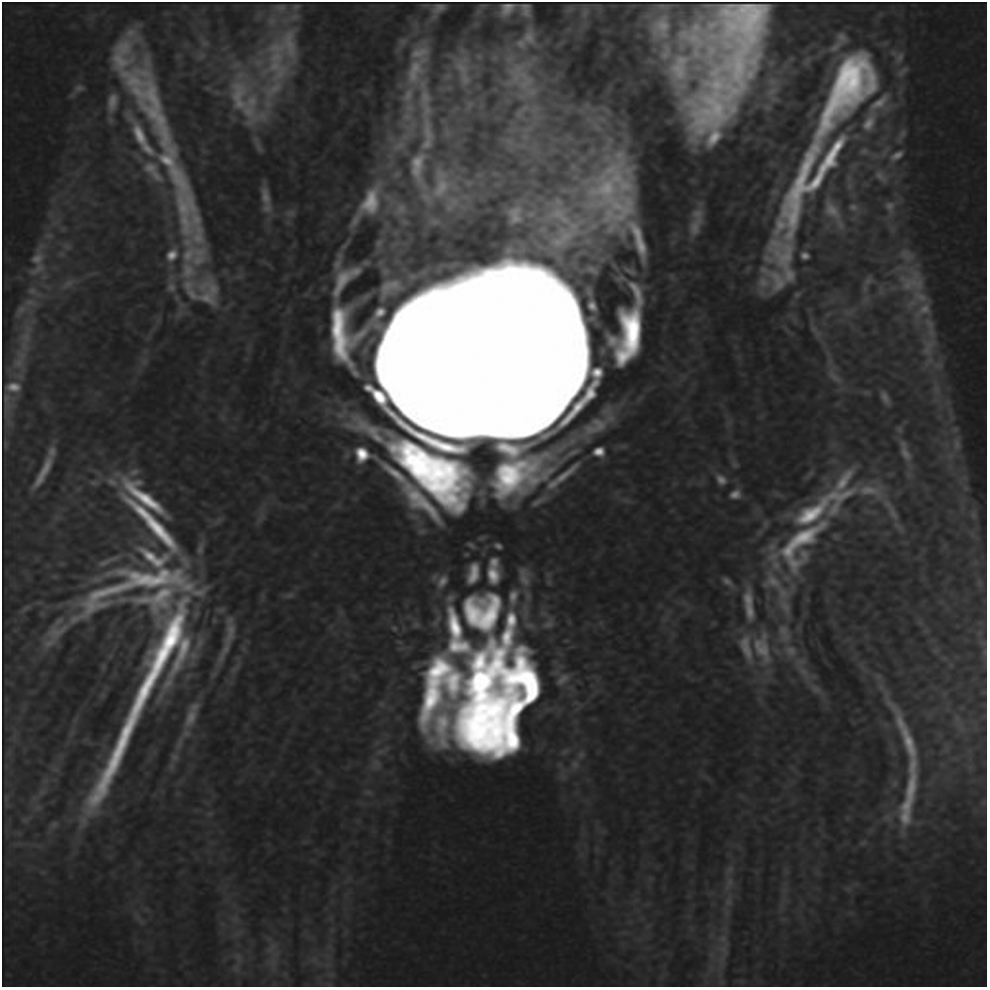
Bone marrow edema with intense signal in preoperative pelvic magnetic resonance imaging.
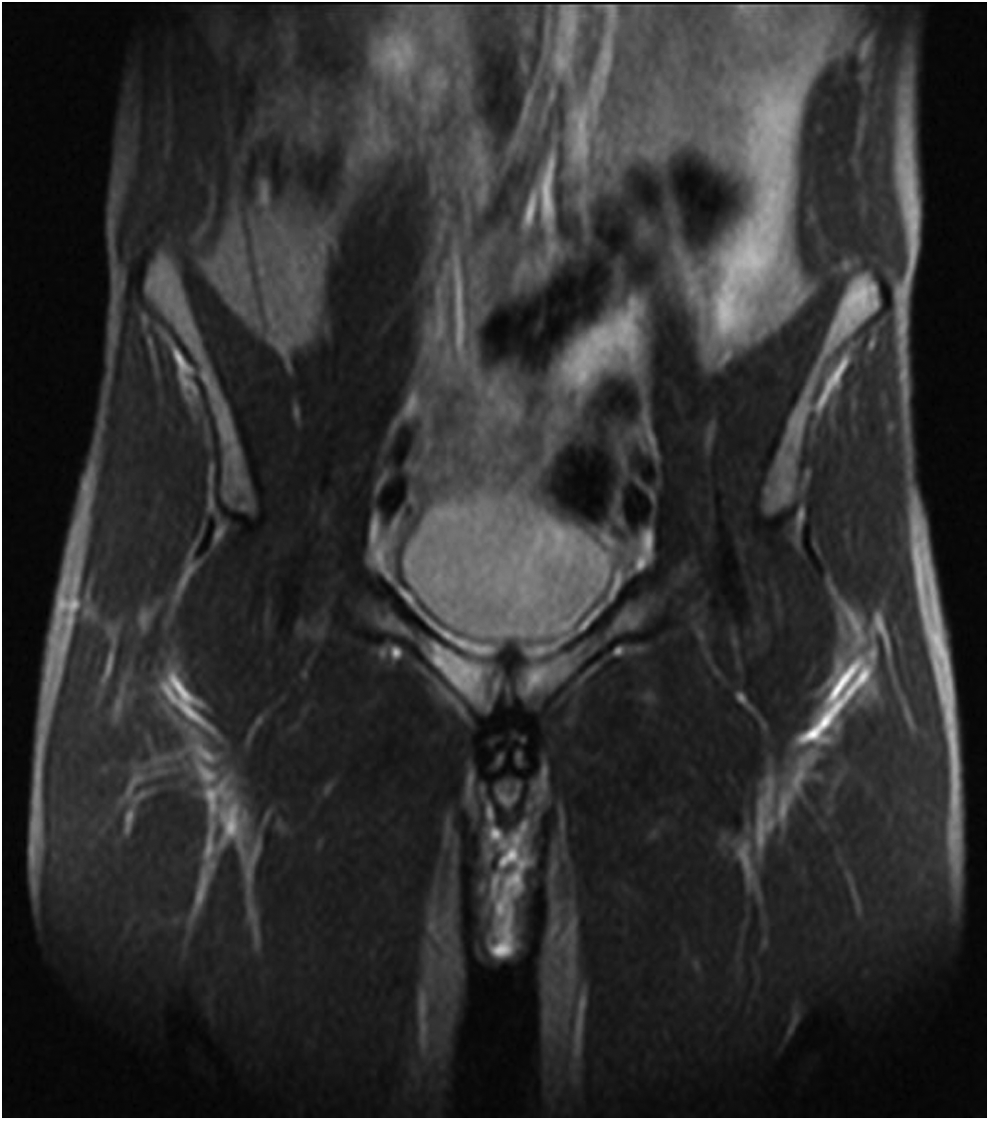
Disappearing signal in pelvic magnetic resonance imaging 6 weeks postoperatively after transabdominal preperitoneal repair.
TAPP, transabdominal preperitoneal.
Laparoscopy confirmed posterior wall deficiency with significant bulge in the posterior wall in 24 (80%) participants (Fig. 3), and true inguinal hernia was found in 6 (20%).

Laparoscopic view of posterior wall deficiency with significant bulge in the posterior wall.
Mean operation duration was 45 (±17) minutes. All study participants spent one night in hospital and were discharged within 24 hours of surgery. Nonsteroidal anti-inflammatory drugs were prescribed for postoperative pain relief. Only two participants experienced mild scrotal hematoma, which was resorbed within 2 weeks. None of the participants reported urinary system complications.
All 30 study participants receiving the TAPP repair participated in the follow-up examination 12 months after the procedure. Twenty-one (70%) had returned to sports activities after 6 weeks of convalescence. Persistent mild pain was experienced by 5 athletes postoperatively for up to 1 year, yet did not interfere with normal daily activity. Twenty-five participants (85%) reported full satisfaction with the procedure 1 year after treatment (Table 3); all participants returned to the same or even higher level of athletic performance they had enjoyed before developing chronic groin pain.
Discussion
Gilmore and other authors have determined that chronic groin pain is caused by posterior wall deficiency resulting from trauma to the musculotendinous part of the posterior inguinal wall, that is, the transversalis fascia or conjoint tendon formed by the medial portion of internal oblique and transversus abdominis muscle. 23
In this prospective cohort study, SG was found exclusively in male athletes, although there are several reports of chronic pain in women. Male athletes have a greater propensity to develop an imbalance between the adductors and lower abdominal musculature due to the higher amount of torque, or twisting, of the muscles inserting at or near the pubis that occurs during sudden acceleration, deceleration, and directional changes. In females, tissue and collagen ratio may provide protection from SG, as, for example, during pregnancy.
Several reports present excellent results when using repair of the posterior inguinal wall deficiency as the main approach. Laparoscopic mesh repair in particular is believed to enable a faster recovery and return to unrestricted sports activities.15–21 Ingoldby's nonrandomized study comparing open and laparoscopic approaches concludes that endoscopic repair can permit an early return to sporting activity: the total postsurgical recovery time (based on return to sports activity) was 17.7 weeks for patients having undergone open repair and 6.1 weeks for those having received laparoscopic repair. 14
In our opinion, the problem does not lie in the lower abdominal muscles; neurotomy of the ilioinguinal or genitofemoral nerve for nerve entrapment is a radical solution. We therefore recommend immediate TAPP repair once the posterior inguinal wall deficiency has been clearly diagnosed.
In this study, typical clinical signs during physical examination that led to surgical treatment included a dilated external inguinal ring in conjunction with a soft bulge during coughing at deep palpation and hypersensitivity or pain when tapping the finger at the floor of the canal where the genitofemoral nerve passes.
Our diagnostic tools included dynamic ultrasound with anterior bulge and ballooning of the inguinal canal at the superficial inguinal ring during coughing and the Valsalva maneuver.24,25
MRI reveals various etiological causes of chronic groin pain. However, in our opinion, MRI is not a tool for surgical decision-making, but instead correlates with successful response to treatment. Furthermore, it may provide positive feedback for the athlete. Among some athletes participating in this study, an increased signal intensity on MRI can be seen due to pubic bone marrow edema consistent with the diagnosis of osteitis pubis.22,26,27
Both the TAPP patch plasty and the total extraperitoneal preperitoneal patch plasty are performed in athletes with SG. Studies have shown the efficacy of both techniques. In this study, our decision to use the TAPP procedure to place a retropubic mesh is based on the salutary outcomes (postoperative pain levels, quality of life, early recovery, and return to daily activities) we have achieved using TAPP as a standardized technique at our hernia center. 28
What is more, a thorough exploration of the retropubic space is advantageous, as it may detect other pathological findings such as true inguinal hernia, wide internal ring and peritoneal dimple, 20 hernia femoralis, 16 hernia obturatoria, 16 or a significant bulge in the posterior wall. Even if no clear pathology is identified, reinforcement of the wall using a mesh offers good clinical results for athletes and is often a long-term resolution to the problem of groin pain. 21
Mesh fixation with tacks or staples was scrupulously avoided. Instead, Fibrin glue was used to secure the mesh to achieve tension-free repair and eliminate chronic pain.
Athletes diagnosed with a weak area of the groin should consider laparoscopic surgical repair of the groin in which the posterior wall is reinforced with mesh. Sufficient support of the conjoined tendon by mesh may uniformly resolve adductor discomfort when supplemented by postoperative rehabilitation. Adductor strain may play a role in this pathological syndrome, and therefore, operative release, tenotomy, or perforation on the pubis should not be performed; in our study, athletes reported relief from adductor-related pain in the postoperative follow-up.
Additional studies on postsurgical rehabilitation for earliest return to full athletic activity are urgently needed. Previous randomized controlled trials have demonstrated that an active physical training program designed to strengthen the muscles to stabilize the hip and pelvis is more advantageous than passive measures.29,30 After laparoscopic repair, patients should participate in a 6-week rehabilitation program of gradually increasing intensity in physical activity.
In this prospective clinical cohort study, we investigated a homogenous group of patients with clear selection criteria based on medical history, physical examination, dynamic ultrasound, and MRI.
The results of this prospective clinical cohort study validate the effectivity of TAPP patch plasty in athletes with SG in respect to fast early recovery (6 weeks postoperation), full resumption of athletic activity without pain, and diminished or absent palpation pain in the groin area.
The posterior positioning of a 10 × 15 cm macroporous, polypropylene lightweight mesh, fixed with Fibrin glue, absorbs muscle pressure and provides firm support to the posterior wall deficiency.
Salutary outcomes depend on an experienced team of specialized general surgeons, orthopedic surgeons, radiologists, and sport physiotherapists with experience in various aspects of groin pain. Multidisciplinary evaluation in both diagnosis and treatment planning is essential to determine underlying causes and to eliminate other possible musculoskeletal and nonmusculoskeletal conditions as a source of groin pain.
Footnotes
Disclosure Statement
H.P., C.R., I.F., V.L., H.N., S.P., and F.L. declare no conflicts of interest related to the submitted work.