
Abstract
Abstract
Objectives:
T1 ventral renal hilar tumors (VRHTs) represent a very special type of tumor, for which laparoscopic partial nephrectomy (LPN) by the retroperitoneal approach is challenging. In this study, we report our surgical technique and Trifecta results.
Methods:
Renal rotation technique has been established for retroperitoneal laparoscopic partial nephrectomy (RLPN) for VRHTs in our institution. Trifecta was used as a composite outcome measure for assessing quality of PLPN using this technique. A retrospective analysis of RLPN cases in 12 patients with VRHTs was performed.
Results:
Mean tumor size was 3.4 cm and median R.E.N.A.L. score was 8 (range 7–9). Mean warm ischemia time was 23.1 minutes, suture time 28.1 minutes, estimated blood loss 139.2 mL, operation time 122.8 minutes, and median hospital stay was 4 days. Three patients (25.0%) had Clavien-Dindo grade I–II complications. Seven patients (58.3%) achieved Trifecta. Postoperative pathological examination showed renal cell carcinoma in all cases with negative surgical margin. A median follow-up of 7 months revealed no local recurrence or distant metastases.
Conclusions:
Our Trifecta outcomes demonstrate that RLPN with renal rotation technique is feasible, safe, and effective for moderately complex VRHTs. The short-term functional and oncologic outcomes are promising; however, long-term follow-up is needed.
Introduction
L
LPN was initially limited to patients with small, superficial, and exophytic tumors at a non-hilar location, and difficult tumor locations have traditionally been regarded as a contraindication to LPN even in the hands of experienced laparoscopic surgeons. With technological advancements and increased surgical expertise, the indication for LPN has expanded to include specific, difficult-to-access tumors, such as hilar tumors. Several retrospective studies have reported the safety and feasibility of LPN for hilar tumors.3–10 Most LPNs for hilar tumors were performed by transperitoneal approach. However, no study has specifically focused on the LPN for hilar tumors with ventral location by the retroperitoneal approach.
Hung et al. introduced the concept of Trifecta outcomes during LPN, in which the three key outcomes of negative surgical margins, minimal renal functional decrease, and no complications are simultaneously realized. 11 However, simultaneous achievement of all three goals in patients with hilar tumors remains technically challenging. This study described our single-center experience of LPN for cT1 ventral renal hilar tumors (VRHTs) with retroperitoneal approach and also discussed the preliminary results of the application of our technique using Trifecta outcomes as surrogate marker of efficacy.
Materials and Methods
Patients
Retrospective analysis was carried out for a total of 12 cases of VRHTs undergoing retroperitoneal laparoscopic partial nephrectomy (RLPN) at a single center in South Central China from September 2012 to December 2015. The informed consent was obtained from all patients for the use of their data. All patients underwent ultrasonography colored doppler, enhanced computed tomography (CT), and computed tomography angiogram examinations with detailed reconstruction of renal vasculature. A hilar tumor was defined as a renal cortical tumor that came in direct physical contact with the renal artery, vein, or both as identified on preoperative imaging (Fig. 1A), and secondarily confirmed by intraoperative findings at RLPN. In all patients, the indication for LPN was selective. Tumor complexity was evaluated based on R.E.N.A.L. nephrometry scores (RNS) as proposed by Kutikov and Uzzo. 12

Preoperative computed tomography imaging and renal rotation technique
Surgical techniques
Three-port RLPN was carried out in all patients. Anesthesia, surgical position, skin incision, retroperitoneal space creation, trocar insertion, CO2 pneumoperitoneum establishment, retroperitoneal fatty tissue clearance, and Gerota's fascia incision were completed as previously described by others. 3
Renal rotation technique was used for these complex tumors (Figs. 1 and 2). The whole kidney was fully dissociated between the kidney capsule and adipose capsule to expose the renal artery, renal vein, and ureter (Figs. 1B and 2A). From this viewing angle, the tumor located at the ventral renal hilum cannot be observed by the retroperitoneal laparoscope (Figs. 1C and 2A). The renal artery was blocked by a vessel clamp (both the renal artery and the renal vein were blocked when necessary) (Fig. 2B), and the blocking time was recorded. The kidney was delicately rotated ∼180° around the renal pedicle, and as a result, the ventral hilar tumor was directly exposed to the visual field of retroperitoneal laparoscopy (Figs. 1D and 2B). This technique eliminates the operation “dead corner.” Thus, the tumor excision and kidney suture can “go smoothly” (Fig. 1E, F).
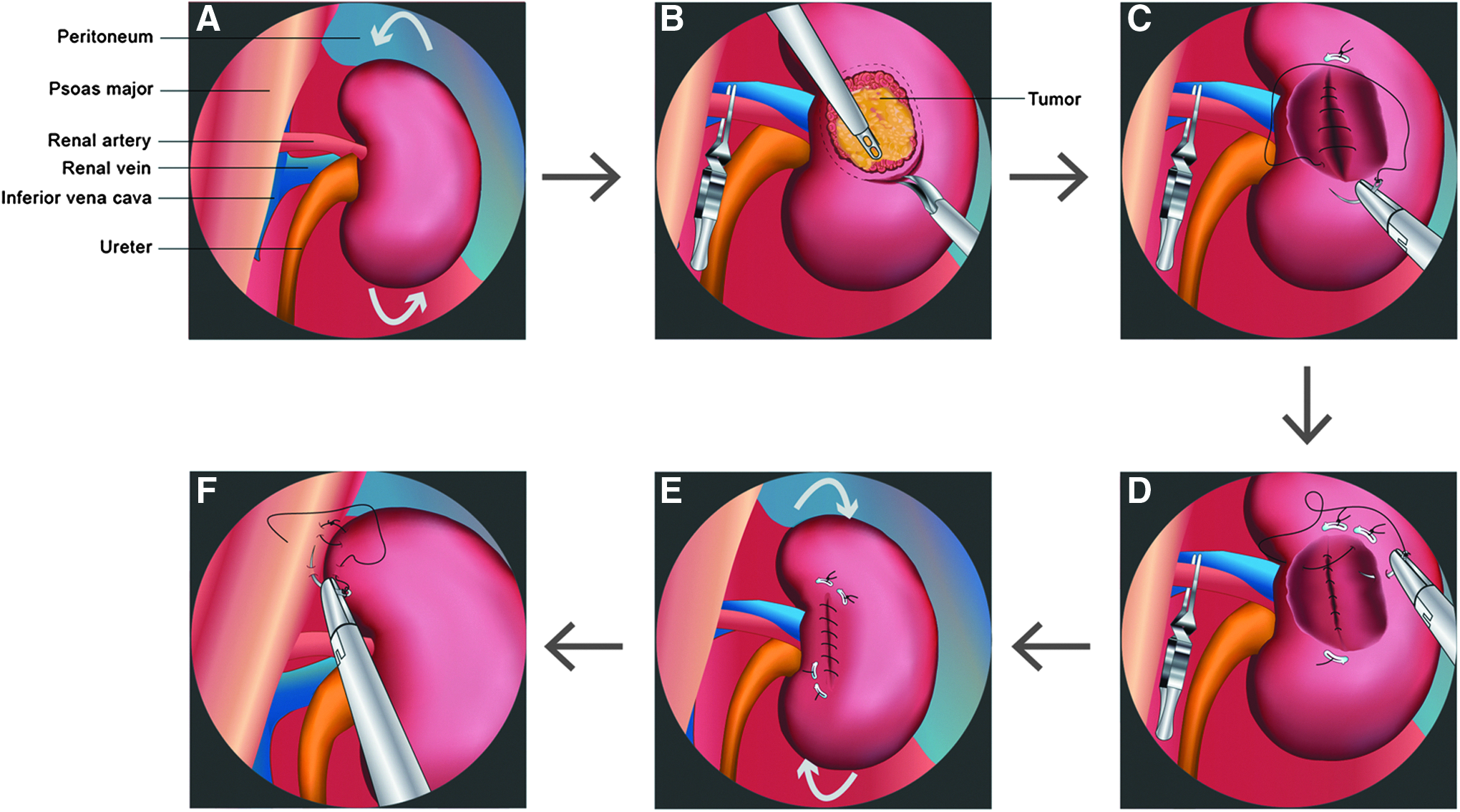
Schematic diagram of retroperitoneal laparoscopic partial nephrectomy for ventral hilar tumors (right kidney is depicted from retroperitoneal visualization
Tumor excision was performed from a lateral to medial direction. 10 While handling the base portion of the tumor, the dissociation from the vessels of the renal pedicle was mainly performed in a delicate blunt manner. Large visible vessels directly entering the tumor were defined and controlled with Hem-o-lok clips.
The renal reconstruction after PN was conducted with two layers of continuous suture using the newly developed absorbable knotless suture with bidirectional barbs (Quill SRS, Angiotech) (Fig. 2C, D). The inner layer of sutures was applied to the kidney medulla on the wound surface, and it was used to close the rupture in the collecting system and the blood vessels in the deep renal parenchyma. Because the base of the wound was close to the large blood vessel and the collecting system of the kidney, the first layer suture could not be too deep. 10 The outer layer of continuous sutures was applied to the outer wound of the kidney in full thickness to reinforce the inner layer of sutures.
If the inner layer was precisely sutured, the outer layer of sutures could be performed after releasing the blood vessel clamps (early unclamping technique). 13 The blood vessel clamp was released and hemostasis was confirmed (Fig. 2E).
After renorrhaphy was completed, the kidney was rotated to restore it to the original position (Figs. 1G and 2E) and then sutured to the psoas muscle to fix the kidney in place (Figs. 1H and 2F). The specimens were collected and submitted for pathological examination.
Methods of evaluation
Preoperative parameters collected included gender, age, mean body mass index (BMI), American Society of Anesthesiologists physical classification (ASA) score, tumor size, tumor side, RNS, serum creatinine (SCr), and estimated glomerular filtration rate (eGFR). Intraoperative and postoperative data, including operative time (OT), warm ischemia time (WIT), suture time, estimated blood loss (EBL), conversion to open surgery, the length of stay, need for transfusion, complications, tumor margin status, tumor histology, SCr, and eGFR, were calculated at the 3-month postoperative follow-up.
GFR was calculated by the use of a modified Modification of Diet in Renal Disease (MDRD) formula based on the Chinese population. 14 Complications were classified according to the Clavien-Dindo grading system. 15 Trifecta outcomes were defined as the combination of total WIT ≤25 minutes, negative surgical margins, and no surgical complications. 16 Patients were evaluated for recurrence based on clinical evidence and the findings on the most recent imaging study (renal ultrasound and/or CT scans).
Statistical analysis
All of the clinical data were statistically analyzed using SPSS 10.0 (Statistical Package for Social Science). Descriptive data are presented as numbers and percentages. For a normal or skewed distribution, continuous data are shown as mean ± standard deviation or median and interquartile range separately. The pre- and postoperative level of SCr and eGFR were separately compared by paired t-test and Wilcoxon Signed-Rank Test according to the distribution of the differences between the two related groups, and a P value <.05 was considered statistically significant.
Results
All 12 patients successfully completed the RLPN, including 8 males and 4 females with a mean age of 48.8 years (range: 32–68). Demographic and tumor characteristics and perioperative, functional, and oncological outcomes are shown in Table 1. The median ASA score was 1.5 (range 1–2) and mean BMI was 23.3 kg/m2. The maximum tumor diameter was 2.5–4.3 cm, with a mean value of 3.4 cm. All cases were single tumor. The preoperative clinical American Joint Committee on Cancer Tumor Node Metastasis (AJCC TNM) staging of the kidney cancer was T1N0M0. The RNS was 7–9 with a median value of 8, and all tumors were classified as being of moderate complexity.
ASA, American Society of Anesthesiologists physical classification; BMI, body mass index; EBL, estimated blood loss; eGFR, estimated glomerular filtration rate; OT, operative time; RCC, renal cell carcinoma; RNS, R.E.N.A.L. nephrometry scores; SCr, serum creatinine; WIT, warm ischemia time.
No case was converted to open surgery, and no nephrectomy was performed. The mean EBL was 139.2 mL (range 80–250) and no blood transfusion was necessary. The mean WIT was 23.1 minutes (range 15–32) and the mean suture time was 28.1 minutes (range 20–40). Three cases required clamping of the renal artery first and then clamping the renal vein due to disturbed visualization of the tumor bed by venous oozing. Early unclamping was achieved in 4 patients. The mean OT was 122.8 minutes (range 110–250). No renal pedicle vascular damage was noticed. In 2 patients, a collecting system entry was noticed and managed laparoscopically.
Three patients (25.0%) had complications consisting of 2 patients with hematuria managed conservatively (Clavien-Dindo grade I) and 1 patient with superficial wound infection at a trocar site managed with antibiotic therapy (Clavien-Dindo grade II). Although a significant difference was found between the mean preoperative and postoperative SCr (P = .000) and eGFR (P = .002), all of the postoperative SCr levels were within normal limits, and no patient required dialysis due to renal insufficiency. The median postoperative hospital stay was 4 days (range: 3–7). Postoperative pathological examination showed RCC in all cases with negative margins. Follow-up was performed for 3–30 months, with a median value of 7 months, and no local recurrence or distant metastases were observed. The rate of Trifecta accomplishment was 58.3% (7/12).
Discussion
RLPN has the advantages of less abdominal interference and easy access to the renal artery. Because of the obese characteristics of patients, transperitoneal approach is recommended in European and American daily practice. 3 However, the retroperitoneal approach is the most common laparoscopic surgical approach used by Chinese urologists because Chinese patients often have smaller body contour. 3 However, this surgical approach also bears drawbacks, including a lack of obvious anatomical markers, a relatively narrow operational space, and suboptimal manual angles for tumors located at the ventral side, renal hilum, or at inferior pole of the kidney. 17
As shown in Table 2, most LPNs for hilar tumors were performed by transperitoneal approach. The renal rotation technique can solve the exposure problem for tumors located at these specific locations and can guarantee tumor excision and kidney suture with a best operating angle. In our case series, we used this technique to facilitate RLPN for VRHTs (Fig. 2).
EBL, estimated blood loss; eGFR, estimated glomerular filtration rate; NA, not available; OT, operative time; WIT, warm ischemia time.
The renal rotation technique was first reported by Lin et al. 17 and subsequently by Song et al. 18 with another description of “renal pedicle rotation.” We also use this technique in our daily clinical practice during the same period. In these case series, we focused on the application of this technique in RLPN for VRHTs (Figs. 1 and 2). Herein, we clearly define the technique of renal rotation. During laparoscopic NSS, for some renal tumors in some difficult-to-access locations, after fully dissociating the kidney and the renal pedicle, the kidney is delicately rotated by a certain angle according to the requirements of the surgery, to allow full exposure of the tumor to direct laparoscopic visualization.
No specific provision has been made for the angle of kidney rotation, which could be adjusted at any time during the surgery for better exposure of the tumor. Generally, the tumor should be optimally visible after kidney rotation, allowing the surgeon to have the best operating angle. Usually, rotations of less than or equal to 180° were able to satisfy these requirements. Damages or tears of the blood vessels and ureter caused by excessive rotation should be avoided. After completing the renal reconstruction, the kidney must be restored to its original position. We recommend the use of prophylactic nephropexy to prevent torsion of the kidney and nephroptosis, which is not highlighted by others.17,18
This technique eliminates the operation dead corner caused by the directional restriction of the laparoscopic operation channel, facilitating tumor resection and renal reconstruction, and reducing the WIT. Further studies referring to the application of this technique in transperitoneal approach are warranted. 18
LPN for renal hilar tumors is extremely challenging. Our preliminary outcomes of our composite RLPN techniques for VRHTs seem to be satisfactory. As shown in Table 2, which summarizes results from contemporary series of LPN for hilar tumors, outcomes in our series are comparable with those in previous LPN series.3–10 In our analysis, we used the Trifecta as a surrogate measure of surgical quality using the renal rotation technique. All patients completed RLPN successfully with a mean WIT of 23.1 minutes and 58.3% patients achieved Trifecta. A total of 9 patients had total WIT ≤25 minutes, no patient had positive surgical margins, and only 3 patients had Clavien-Dindo grade I–II complications. No renal pedicle vascular damage, hemorrhage, or urine leakage was observed.
A recent study demonstrated that hilar location of RCC was an independent predictor of recurrence in T1 RCCs after nephrectomy and in T1a hilar tumors, patients treated with PN showed poorer recurrence-free survival than radical nephrectomy. 19 Although there is no evidence of recurrence or metastases after a median follow-up of 7 months (range: 3–30 months) in our patients, long-term follow-up is needed to determine the oncologic outcome of hilar tumors managed by RLPN.
Several limitations still exist in our study. First, it is a retrospective study with limited follow-up in a single center. Second, this is a small series of 12 cases performed over a 3-year period because the study specifically focuses on hilar tumors with ventral location, which are rare in nature. Third, because over the same study period, we have not treated the same type of tumors with a transperitoneal approach, we cannot provide a control group and failed to demonstrate the advantages and disadvantages of our techniques in comparison with LPN for VRHTs with a transperitoneal approach. Thus, long-term, multicenter clinical trials with larger patient samples are needed to further confirm the advantages of our RLPN technique for hilar tumors.
Conclusions
Our Trifecta outcomes demonstrate that RLPN with our techniques is feasible, safe, and effective for moderately complex VRHTs. The short-term functional and oncologic outcomes are promising; however, long-term follow-up is needed.
Footnotes
Disclosure Statement
No competing financial interests exist.