
Abstract
Abstract
Background:
We assessed postoperative outcome in relation to the level of transection of the biliary remnant at the time of laparoscopic Kasai portoenterostomy (LKP) in biliary atresia (BA) patients.
Methods:
The subjects for this study were 12 consecutive nonsyndromic type III BA patients who had LKP at our institute between 2009 and 2014. All LKPs were video recorded. Four board-certified pediatric surgeons assessed the level of transection of the biliary remnant and suturing during the anastomosis in each video blindly. A standard protocol was used for postoperative management.
Results:
The level of transection was assessed as being shallow and suturing techniques as being identical in all. Although all cases achieved jaundice disappearance, 4 required liver transplantation (NNL group) for relapse of jaundice and 8 remain anicteric with native livers after mean follow-up of 4.6 years (NL group). Demographic data (birth weight, weight and age at LKP, duration from onset of symptoms to LKP, size of microbile ducts, and preoperative biochemical markers) were similar for both groups.
Conclusions:
The level of transection of the biliary remnant and suturing techniques would appear to not directly influence the outcome of LKP.
Introduction
T
In this study, intraoperative video recordings were assessed to confirm what influence the level of transection of the biliary remnant at the porta hepatis during laparoscopic Kasai portoenterostomy (LKP) has on postoperative outcome in BA.
Materials and Methods
There were 14 consecutive BA patients treated by LKP at our institute between 2009 and 2014. Classification of BA was isolated type, that is, nonsyndromic type III BA (n = 12), syndromic type III BA (n = 1), and isolated type II BA (n = 1). Syndromic type III BA and type II BA were excluded, leaving only nonsyndromic isolated BA (n = 12) as subjects for this study.
LKP was indicated based on a patient's capacity to tolerate surgery and size determined by the patient's clinical status and weight at the time of planned surgery. These two parameters provide a good indication of a patient's ability to tolerate longer surgery and size. Thus, heavier patients in better clinical condition can generally tolerate longer surgery, and LKP is usually chosen. Staff availability may also affect choice of procedure to an extent because 2 of the coauthors, A.Y. and H.K., are more experienced with LKP.
We compared outcome of cases who survived with native livers (NLs) with those who did not survive with native livers (NNLs) with respect to birth weight, weight and age at LKP, duration between onset of symptoms and LKP, jaundice disappearance (JD) ratio, size of microbile ducts, and preoperative biochemistry (aspartate aminotransferase: AST, alanine aminotransferase: ALT, alkaline phosphatase: ALP, total bilirubin: T-Bil, and cholinesterase: ChE). In this study, age at onset of symptoms was defined as the age when an acholic stool was passed or when jaundice or abnormal biochemistry was detected.
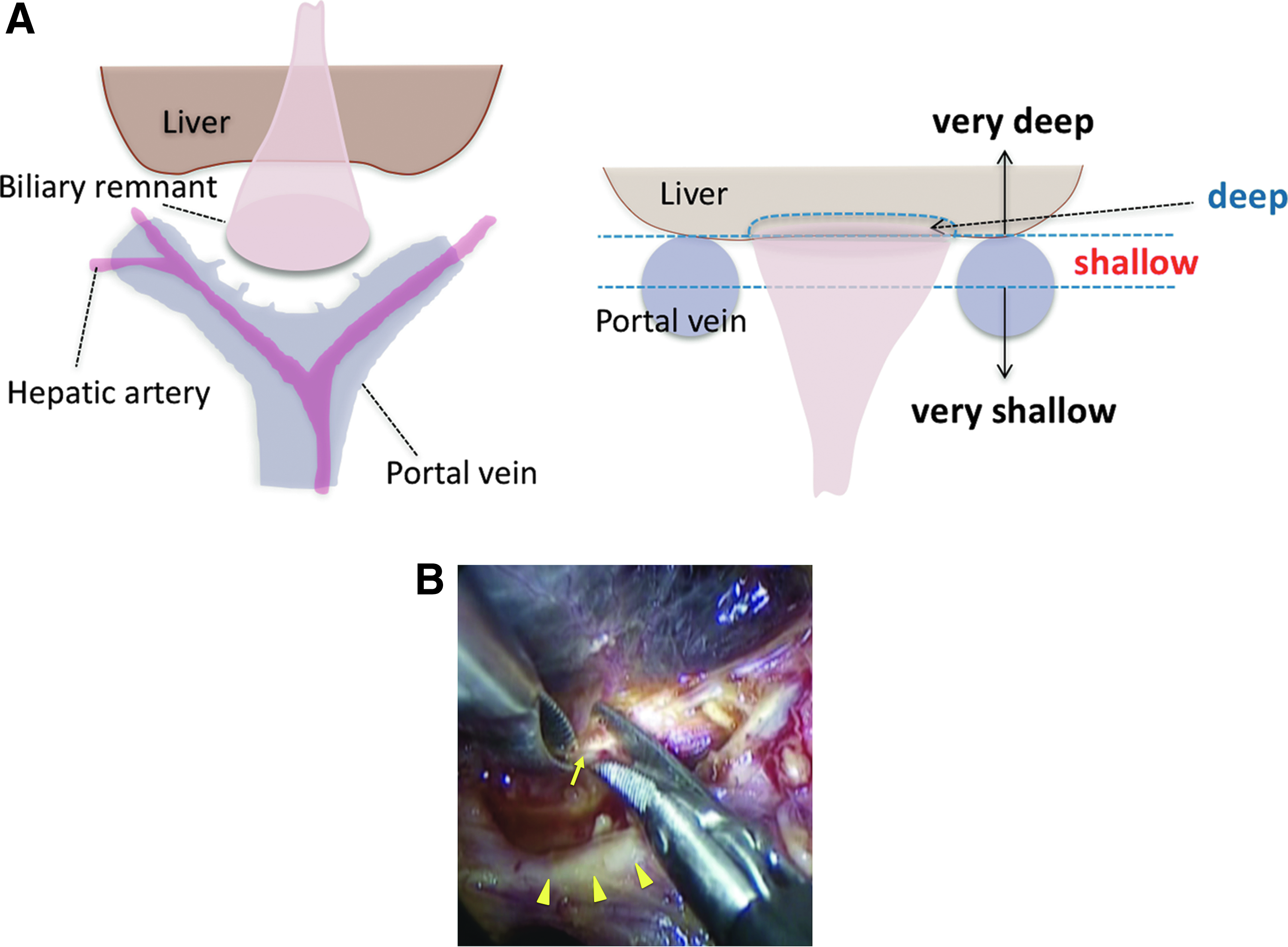
Details of our LKP procedure may be found elsewhere. 4 Dissection of the porta hepatis is confined to the area around the base of the biliary remnant. In our series, because the level of transection of the biliary remnant was shallow, there was no need to retract the right and left portal veins and hepatic arteries; sutures placed at the 2 and 10 O'clock positions were for reinforcement only.
Four board-certified specialist pediatric surgeons (2 from our institute and 2 from elsewhere with no knowledge of our subjects) who had each performed a total of at least 30 open and LKPs reviewed intraoperative video recordings of each LKP blindly. Each reviewer was asked to assess the level of transection of the biliary remnant at the porta hepatis as being very shallow if above an imaginary plane between the right and left portal veins, that is, furthest from the porta hepatis; shallow if below this plane, that is, closer to the porta hepatis; deep if the liver parenchyma was visible through the transected biliary remnant without lateral dissection; and very deep if the liver parenchyma was visible through the transected biliary remnant with lateral dissection (Fig. 1). Suturing at the anastomosis such as the depth and location of sutures was also reviewed.
Postoperative management
All cases were managed by the same standard postoperative management protocols for antibiotics, corticosteroids, and cholagogues, details of which may be found elsewhere. 6
Statistical analyses
Survival rates of patients with NLs were calculated by the Kaplan–Meier method with end points of death or liver transplantation (LTx). The Student's t test and Chi-squared test were used for statistical analysis. A P value <.05 was considered to be statistically significant.
Ethics
This study was approved by the Ethics Committee of Juntendo University School of Medicine and complies with the Helsinki Declaration of 1975 (revised 1983).
Results
Results are summarized in Table 1. JD was achieved initially in all 12 subjects. However, 4 required LTx for relapse of jaundice (NNL group) and 8 remain anicteric with native livers (NL group) after mean follow-up of 4.6 years (range 1.3–7.0 years). On comparing the 8 NL cases with the 4 NNL cases, mean birth weight was 2.7 kg (range 2.2 to 3.4 kg) for NL and 2.8 kg (range 2.7–3.0 kg) for NNL (P = NS); mean weight at LKP was 4.0 kg (range 3.3–4.6 kg) for NL and 4.7 kg (range 4.5–5.0 kg) for NNL (P = NS); mean age at LKP was 59.6 days (range 29–79 days) for NL and 81.0 days (range 58–119 days) for NNL; mean duration between onset of symptoms and LKP was 31.3 days (range 11–53 days) for NL and 60.3 days (range 15–110 days) for NNL; and mean microbile duct size was 91.3 μm (range absent to 200 μm) for NL and 212.5 μm (range 100–400 μm) for NNL. Differences in mean age at KP, mean duration between onset of symptoms and age at KP, and mean microbile duct size did not reach statistically significant levels but were less in the NL group probably because of the small number of subjects in each cohort. JD after LKP was 100% for both NL (8/8) and NNL (4/4) (P = NS). Results for postoperative biochemistry such as AST, ALT, ALP, T-Bil, and ChE were similar. Each reviewer assessed the level of transection as being shallow, and suturing at the anastomosis to be identical in all 12 cases.
Duration: between onset of symptoms and LKP.
AST, aspartate transaminase; ALT, alanine transaminase; ALP, alkaline phosphatase; ChE, cholinesterase; NL, native liver; NNL, non-NL; LKP, laparoscopic Kasai portoenterostomy; NS, not significant; T-Bil: total bilirubin.
Rates for survival with the NL calculated by the Kaplan–Meier method for the 12 cases in our series with end points of death or LTx were 95.2%, 79.6%, 79.6%, and 66.3% at 0.5, 1, 3, and 5 years after LKP, respectively (Fig. 2). Currently, at just under 5 years, survival with the NL in this series is 8/12 (66.6%).
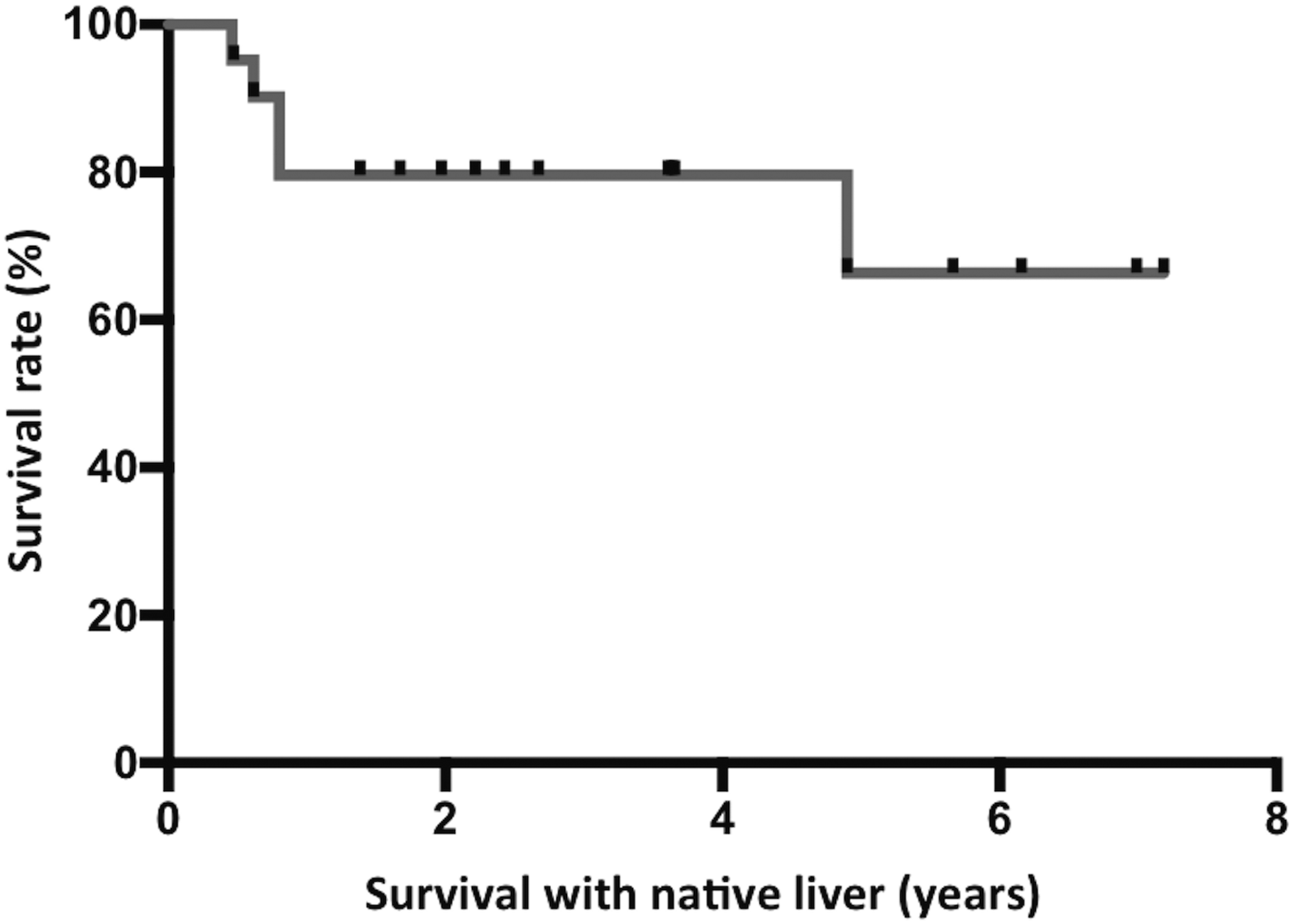
Kaplan–Meier analysis showing survival rates of patients with native livers. Survival rates were calculated with end points of death or liver transplantation.
For reference, results for the syndromic type III and isolated type II BA cases excluded in this study were the syndromic type III case did not achieve JD and required LTx and the isolated type II BA case achieved JD and remains anicteric at the time of writing.
Discussion
In this study, we excluded syndromic BA and type II BA cases, and used only nonsyndromic BA cases because the postoperative outcome of syndromic BA is worse than nonsyndromic BA and isolated BA, 7 and type I and type II BA have better prognosis than type III BA,8,9 and we wished to focus on assessing the level of transection and depth of suturing. Thus, by excluding types of BA with poorer prognosis, bias related to differences in histopathology that might affect outcome would be eliminated, allowing a direct comparison of surgical technique to be performed. Most studies on outcome of BA surgery assess a mix of types of BA, which may give rise to a spectrum of results. Ideally, research on outcome of BA surgery should be reported with respect to each type of BA, or at least be divided into syndromic (isolated) and nonsyndromic, respectively. In this study, only isolated type III BA data were analyzed, thus, we feel our conclusions are not biased by the presence of syndromic BA and other BA types.
Mean microbile duct size was 91.3 μm (range absent to 200 μm) for NL and 212.5 μm (range 100–400 μm) for NNL. This is interesting because NNL group cases eventually had liver transplants but had larger microbile ducts at the porta hepatis than NL cases, although the difference was not statistically significant (P = .06). This finding is very similar to the results of an article we published previously, which included open Kasai portoenterostomy 10 cases. The size of microbile ducts would generally be accepted as a predictor of postoperative JD, with larger microbile ducts expected to contribute to better bile flow, which, in turn, would suggest that bile drainage over a wide area of the liver should be better; however, this study and our previous article 10 showed that the size of microbile ducts does not appear to be a prognostic factor in BA patients.
In this study, we used intraoperative video recordings of LKP to assess the level of transection of the biliary remnant and suturing techniques at the anastomosis, a first for BA research. A limitation of our study is that we were not able to make any comparison with laparoscopic transection of the biliary at a deep margin, which makes it difficult to draw meaningful conclusions about the depth of transection as a variable that influences outcome. What we did confirm here is that despite the level of transection of the biliary remnant and suturing being the same in all 12 cases, postoperative outcome varied. Thus, outcome would not appear to be reliant on surgical factors alone because the level of transection and suturing was the same in all our subjects.
Although our series is small, we are the first to show that if the level of transection of the biliary remnant is kept shallow, outcome of LKP would appear to be influenced by nonsurgical factors rather than surgical technique. Shallow transection would appear to be associated with JD, but factors affecting final outcome are still a mystery and treating BA continues to be difficult, causing considerable dilemma to pediatric surgeons.
Footnotes
Disclosure Statement
No competing financial interests exist.