
Abstract
Abstract
Aim:
To quantitatively determine whether a three-dimensional (3D) image improves laparoscopic performance compared with a two-dimensional (2D) image.
Method:
This is a prospective study with two groups of participants: novices (5) and experts (5). Individuals within each group undertook a validated laparoscopic task on a box simulator, alternating between 2D and a 3D laparoscopic image until they had repeated the task five times with each imaging modality. A dedicated motion capture camera was used to determine the time taken to complete the task (seconds) and instrument distance traveled (meters).
Results:
Among the experts, the mean time taken to perform the task on the 3D image was significantly quicker than on the 2D image, 40.2 seconds versus 51.2 seconds, P < .0001. Among the novices, the mean task time again was significantly quicker on the 3D image, 56.4 seconds versus 82.7 seconds, P < .0001. There was no significant difference in the mean time it took a novice to perform the task using a 3D camera compared with an expert on a 2D camera, 56.4 seconds versus 51.3 seconds, P = .3341.
Conclusion:
The use of a 3D image confers a significant performance advantage over a 2D camera in quantitatively measured laparoscopic skills for both experts and novices. The use of a 3D image appears to improve a novice's performance to the extent that it is not statistically different from an expert using a 2D image.
Introduction
O
There is a growing interest in three-dimensional (3D) laparoscopic equipment to overcome this barrier; however, there are few studies that directly compare the performance of a 3D image with that of a 2D image using quantitative motion capture techniques. 1
A recently published systematic review of 3D versus 2D vision in laparoscopy concluded that overall, 3D laparoscopy appears to improve speed and reduce the number of performance errors when compared with 2D laparoscopy. 2
The potential benefits of simulated 3D laparoscopy as a training tool for prospective surgeons have been highlighted by Votanopoulos et al., 3 who were able to demonstrate that 3D offered significant advantages in the teaching of laparoscopic skills to inexperienced individuals.
We have previously described a validated laparoscopic simulated task to test one's laparoscopic skills 4 and the novel “InsTrac” instrument-tracking software that is able to give objective feedback on one's laparoscopic performance. 5
The aim of this study was to quantitatively determine whether a 3D image improves laparoscopic performance compared with a 2D image and what effect it has on the learning curve, using a validated laparoscopic task and motion capture technology.
Materials and Methods
This is a prospective study with two groups of participants: novices (5) and experts (5). Novices are defined as junior doctors or medical students with no prior laparoscopic experience. Experts are defined as surgical trainees or consultants with 50 or more independent laparoscopic cases.
The laparoscopic task and simulator used in this study have been previously validated 4 as has the “InsTrac” instrument-tracking software. 5
Individuals within each group undertook a validated laparoscopic task (threading a string through a series of five hoops) on an eoSim (eoSurgical™ Ltd., Edinburgh, Scotland, United Kingdom) laparoscopic simulator, alternating between a 2D and a 3D laparoscopic image on the same camera until they had repeated the task five times with each imaging modality. The camera position was fixed in a standard position for all the participants. The start point was with the tips of the left and right hand laparoscopic graspers held just outside the ports. The end point was the removal of the laparoscopic instruments from the simulator on completion of the task (Figs. 1 and 2).

Standard configuration of 2D/3D camera and the eoSim laparoscopic simulator box fitted with the “InsTrac” instrument tracking software. 2D, two-dimensional; 3D, three-dimensional.

Completed laparoscopic task showing the thread passed through the five hoops.
Using a dedicated motion capture camera, data collected included time taken to complete the task (seconds) and instrument distance traveled (meters).
Statistics were performed using Stats Direct 2.7.8 (Stats Direct Ltd., Altrincham, Cheshire, United Kingdom). A paired t-test was used to compare the performance on a 2D versus a 3D image within each group. An unpaired t-test was used to compare the performance between the two groups on a 2D and a 3D laparoscopic image.
Results
Among the experts, the mean time taken to perform the task on the 3D image was significantly quicker than on the 2D image, 40.2 seconds (95% confidence interval [CI] 35.1–45.3) versus 51.2 seconds (95% CI 44.4–58.1), P < .0001.
Among the novices, the mean task time again was significantly quicker on the 3D image, 56.4 seconds (95% CI 27–114) versus 82.7 seconds (95% CI 41–207), P < .0001.
There was no significant difference in the mean time it took a novice to perform the task using a 3D camera compared with an expert using a 2D camera, 56.4 seconds (95% CI 27–114) versus 51.3 seconds (95% CI 29–80), P = .3341.
Among experts, there was no significant difference in the distance traveled with the laparoscopic instruments when using a 2D image compared with when using a 3D image, 1.08 m (95% CI 0.64–1.86) versus 1.01 m (95% CI 0.58–1.6), P = .2721.
Among novices, there was a significant difference in the distance traveled between 2D and 3D camera use, 1.37 m (95% CI 0.61–3.59) versus 1.12 m (95% CI 0.64–2.23), P = .0193 (Fig. 3).
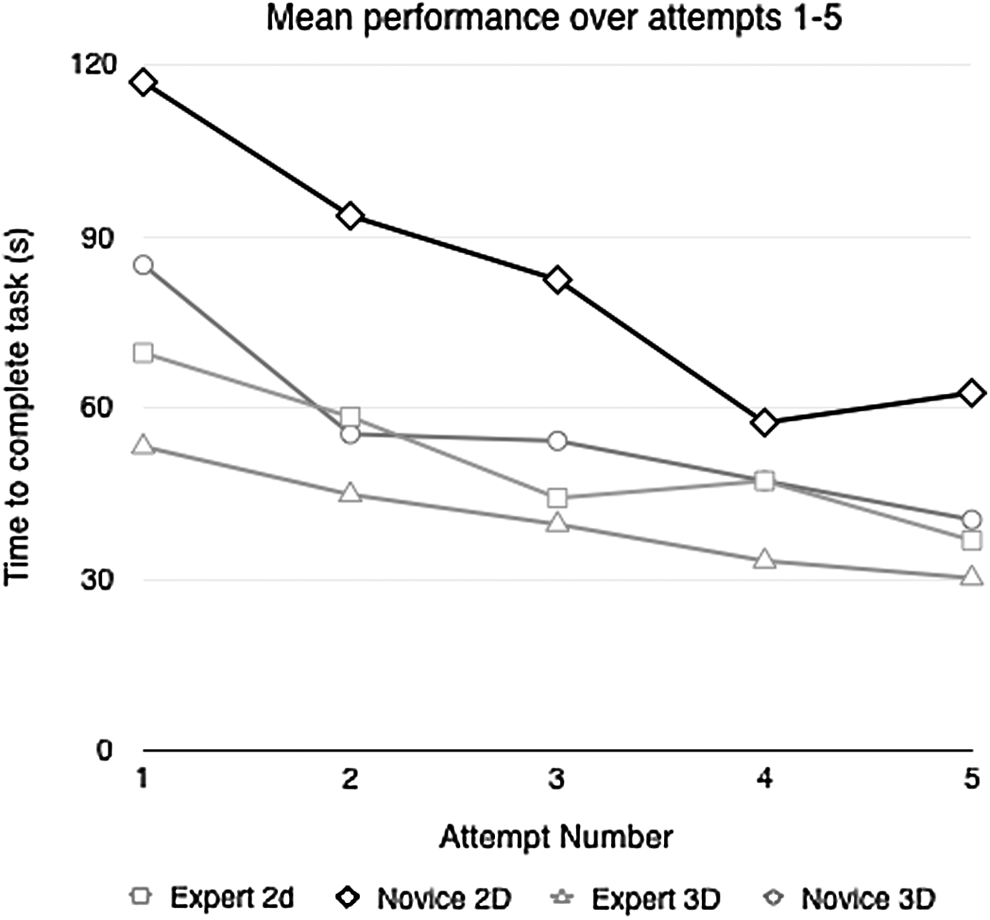
Graph showing the mean times taken to complete the task over five attempts by the experts and novices using the 2D and 3D laparoscopic image. 2D, two-dimensional; 3D, three-dimensional.
Discussion
Our study demonstrates that there is a clear advantage of a 3D image over a 2D image in the performance of a laparoscopic task, with regard to the time taken to complete the task and the reduction of the learning curve, particularly for novices. Expert surgeons were able to perform the laparoscopic task significantly quicker using a 3D camera as opposed to using a 2D camera (40.2 seconds versus 51.2 seconds, P < .0001). The explanation for this is multifold: the 3D image confers a superior depth of perception, thereby enabling the surgeon to position the thread in the hoops with greater precision, ultimately leading to quicker task completion time.
It was striking to see that there was no significant difference in the mean time it took a novice to perform the task using a 3D camera compared with an expert using a 2D camera (56.4 seconds versus 51.3 seconds, P = .3341). The obvious interpretation of this result is that a 3D laparoscopic image enables a novice surgeon to perform a simple task to the same level in terms of completion time as an expert surgeon using a 2D laparoscopic image. This could have implications for future surgical training in that the learning curve for laparoscopic training and performance could be shortened for trainees by the use of a 3D laparoscopic camera as opposed to a 2D camera.
There have been a number of studies demonstrating that 3D laparoscopy confers a shorter operating time, a shorter learning curve, and better depth of perception.6–8 Where this study stands out is that we have made a direct comparison between novices and experts and have demonstrated that the rate of acquisition of laparoscopic skill fostered by the use of a 3D laparoscopic camera can propel a novice surgeon to the same level as an expert surgeon using a 2D laparoscopic camera in the performance of a given task.
Interestingly, the use of the 3D image resulted in a shorter distance being traveled to complete the task than when using a 2D image, for novices but not for experts. This could be due to the fact that the number of subjects tested was not large enough to detect a difference if there indeed was a difference. Also it could be attributed to the experts being able to adapt better and compensate for the inferior image because of their superior baseline laparoscopic skills set. In addition, the experts have become experts on 2D laparoscopic image, hence they are preconditioned to working with a 2D laparoscopic image and would have made adjustments throughout their years of training to compensate for the shortcomings of the 2D laparoscopic image. On the contrary, novices without any prior laparoscopic experience would be better at bringing to the fore the superiority of one image modality over the other because they would not have had years of preconditioning and adaptation to one image modality.
The “InsTrac” instrument-tracking software is capable of measuring the average speed (mm/second), average acceleration (mm/second 2 ), average motion smoothness (mm/second 3 ), percentage off screen and handedness, in addition to the time taken to complete the task and instrument path distance. We decided to focus on the last two metrics, as these have been identified as the key performance metrics for laparoscopic skills assessment. 9
Conclusion
The use of a 3D image confers a significant performance advantage over a 2D image in quantitatively measured laparoscopic skills for both experts and novices. The use of a 3D image appears to improve a novice's performance to the extent that it is not statistically different from an expert using a 2D image.
Footnotes
Disclosure Statement
R.W.P. and I.A.M.H. have taken steps to address the poor access to surgical simulation tools by designing and manufacturing affordable take-home simulation equipment. They established a company “eoSurgical Ltd.” (eoSurgical.com) to achieve this. R.W.P. and I.A.M.H. are shareholders in eoSurgical Ltd. The “eoSim” take-home laparoscopic simulator used in this study is manufactured by eoSurgical Ltd. (eoSurgical™ Ltd., Edinburgh, United Kingdom). The “InsTrac” software also used in this study was developed in conjunction with a separate company “Peekabu Studios” (Peekabu Studios Ltd., Edinburgh, United Kingdom), and is marketed by eoSurgical Ltd.