
Abstract
Abstract
Purpose:
To evaluate two-incision laparoscopic cholecystectomy (2I-LC) in children, and compare outcomes with four-port laparoscopic cholecystectomy (4P-LC).
Methods:
A retrospective review was performed on children (≤21 years) with gallbladder disease treated with 2I-LC or 4P-LC between February 2010 and February 2016. 2I-LC is performed using two 5-mm ports and a 2-mm endoscopic grasper within a 12-mm umbilical incision, and a 3-mm subxiphoid port for dissection. Demographic, diagnostic, operative, and outcome data were recorded, and the two groups were compared with chi-squared, Fisher, and t-tests. Patients requiring conversion from 2I-LC to 4P-LC were examined to determine factors predicting the need for additional ports.
Results:
Three hundred eighty-nine laparoscopic cholecystectomies were performed (2I-LC 72.0%, 4P-LC 19.0%). Body mass index (BMI) was greater in the 4P-LC group. 2I-LC was more commonly performed for biliary dyskinesia, but not biliary colic, acute cholecystitis, choledocholithiasis, and gallstone pancreatitis. Operative time was greater in 4P-LC. There were 6 wound infections (2I-LC 1.8%, 4P-LC 1.5%), 1 common bile duct injury (2I-LC 0.4%, 4P-LC 0.0%), and 1 small bowel injury (2I-LC 0.0%, 4P-LC 1.5%). 2.4% of 2I-LC required conversion to 4P-LC, with BMI and operative time greater than the 2I-LC group, but not different from 4P-LC with no complications.
Conclusions:
2I-LC is a safe alternative to 4P-LC for pediatric gallbladder disease, allowing for traction and countertraction to expose the critical view. Operative time was longer in the 4P-LC group, likely secondary to selection bias with higher BMI and preoperative diagnosis of gallstone disease. Overweight patients are more likely to require additional ports.
Introduction
W
Although initial experience with single-incision surgery required specialized single-port equipment, it is possible to perform this technique using conventional ports. Given potential concerns regarding complications, prolonged operative time and steep learning curve, we previously described the use of modified single-incision laparoscopic surgery that has recently been adapted further by the introduction of miniature laparoscopic instruments. 4 At our institution, we now perform a two-incision laparoscopic cholecystectomy (2I-LC), in which three working instruments are used for traction and countertraction to define the critical view of safety. In this study, we sought to describe our technique and examine the outcomes of 2I-LC and 4P-LC in our large cohort of 389 pediatric patients, as well as factors that predict conversion of 2I-LC to 4P-LC.
Materials and Methods
With ethics approval, a retrospective chart review was performed on children younger than 21 years, who were treated with laparoscopic cholecystectomy for gallbladder disease at a single institution between February 2010 and February 2016. Types of gallbladder disease included cholelithiasis, cholecystitis, choledocholithiasis, gallstone pancreatitis, polyps, and biliary dyskinesia. Demographic data (age, sex, weight, height, BMI [body mass index]), diagnosis, operative findings, and complications were collected.
Patients were stratified by procedure based on 2I-LC, 4P-LC, and those requiring conversion from 2I-LC to 4P-LC. Patients with unclear port placement or different arrangements of ports were excluded. Results are expressed as mean ± standard deviation (SD) and analyzed using chi-squared, Fisher, and t-tests. All statistical tests were performed using GraphPad Prism 6.0 statistical software (GraphPad, San Diego, CA). P < .05 was deemed statistically significant.
Operative technique
A Veress needle is used to access the peritoneal cavity within an infraumbilical incision and insufflate to pressures of 15 mmHg. After insertion of ports and graspers (described in sections “Two-incision laparoscopic cholecystectomy” and “Four-port laparoscopic cholecystectomy”), the critical view is demonstrated, the cystic duct and artery are clipped and divided, and the gallbladder is dissected off the liver bed with cautery before delivery through the umbilical site within an endoscopic bag (5-mm Inzii Universal Retrieval System; Applied Medical, Rancho Santo Margarita, CA) after widening the fascial defect. 13
Two-incision laparoscopic cholecystectomy
We previously described a modified single-port laparoscopic cholecystectomy method that included a 10-mm working port at the umbilicus and a 3-mm subxiphoid port. 4 This two-incision technique was used in the initial 69 patients included in this group. This was further adapted to the 2I-LC method used for the remaining patients in this group that replaces the 10-mm working port with two standard ports instead. A camera and 5-mm grasper are placed via two 5-mm ports (one Applied Medical, Rancho Santo Margarita, CA; one Karl Storz Endoscopy-America, El Segundo, CA) within a 12-mm umbilical skin incision through separate fascial openings (right and left lateral, respectively) for manipulation of the infundibulum. A 2-mm endoscopic grasper (Stryker Mini-Lap Alligator Grasper, Morrisville, NC) is inserted via the umbilicus through a fascial stab incision for retraction of the gallbladder fundus. A 3- to 5-mm subxiphoid port is then used for dissection with hook cautery.
The surgeon controls the 5-mm grasper (left hand) and the hook cautery (right hand) from the left side of the bed, while the assistant holds the camera (right hand) and 2-mm grasper (left hand) from the patient's right. The 5- and 2-mm graspers are used to triangulate tissues with traction–countertraction. Figures 1 and 2 depict the external port placement and the intraoperative view attained for gallbladder dissection, respectively.

Port placement for two-incision laparoscopic cholecystectomy. Two 5-mm ports are placed via separate fascial punctures within a 12-mm umbilical incision and a 5-mm camera (5C) and 5-mm grasper (5G) inserted. A 2-mm grasper (2G) is inserted via a fascial stab incision in the umbilicus. A 3-mm port and 3-mm hook dissector (3H) are placed subxiphoid. The surgeon controls 5G (left hand) and 3H (right hand) from the left side of the bed, while the assistant holds 5C (right hand) and 2G (left hand) from the right side of the bed.
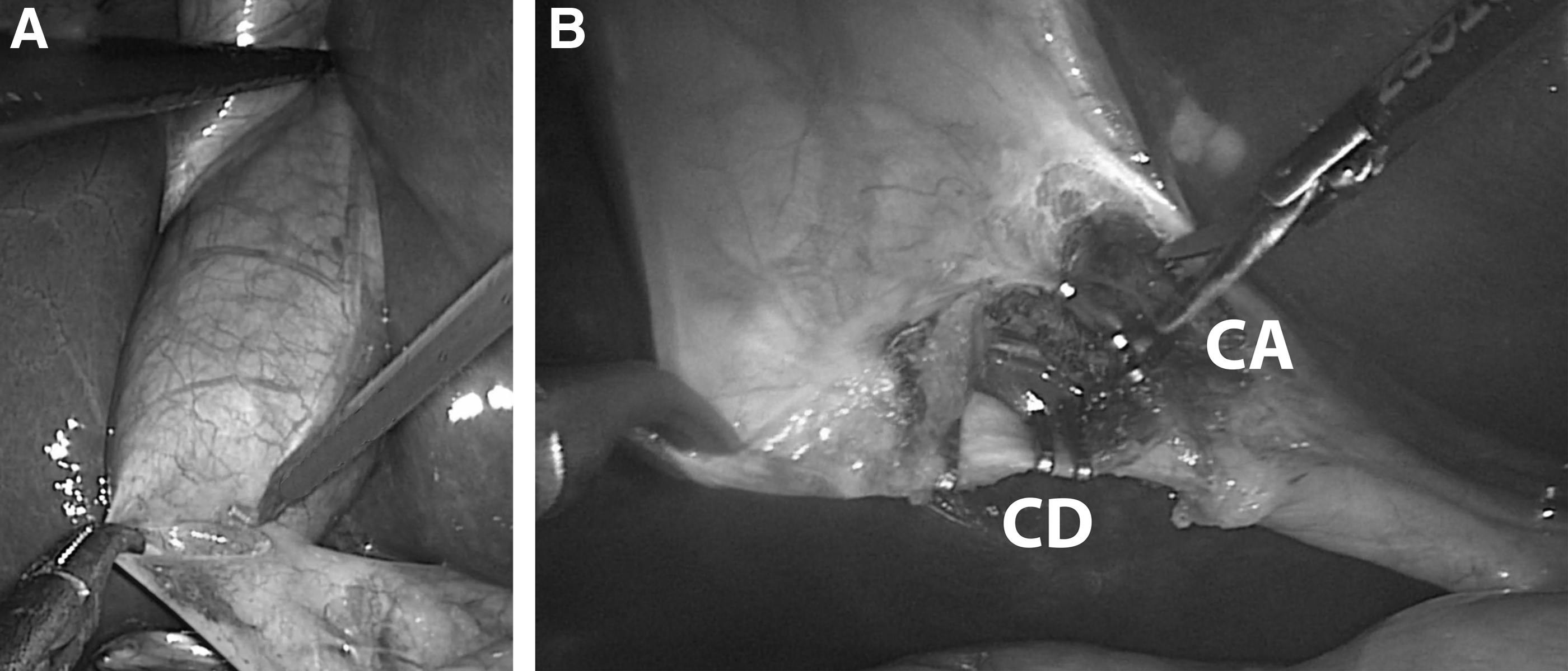
Intraoperative view of two-incision laparoscopic cholecystectomy.
Four-port laparoscopic cholecystectomy
The 4P-LC method is performed using a 5-mm umbilical camera port, a 3- to 5-mm subxiphoid working port for dissection with hook cautery, and two 3- to 5-mm ports inferior to the right costal margin. The right costal margin ports are used for graspers to retract the gallbladder fundus and infundibulum, allowing for triangulation of tissues with traction–countertraction.
Results
A laparoscopic cholecystectomy was performed in 389 children. Of these, 28 patients were excluded from the study due to unclear port placement (based on operative reports) or different arrangements of ports than 2I-LC or 4P-LC. Table 1 shows the study participant characteristics stratified into groups of patients receiving 2I-LC, 4P-LC, or those requiring conversion from 2I-LC to 4P-LC. Of note, only 337 patients were younger than 18 years of age. The intraoperative rationale for conversion from 2I-LC to 4P-LC included obesity (5 patients), duodenal inflammation and unclear anatomy (1 patient), and instruments too short (1 patient).
P < .05 versus 2I-LC.
P < .05 versus 4P-LC.
2I-LC, two-incision laparoscopic cholecystectomy; 4P-LC, four-port laparoscopic cholecystectomy; BMI, body mass index; ERCP, endoscopic retrograde cholangiopancreatography; SD, standard deviation.
BMI was higher in the 4P-LC and conversion groups, compared with 2I-LC. There were more patients diagnosed with complications of gallstone disease (biliary colic, acute cholecystitis, choledocholithiasis, and gallstone pancreatitis) in the 4P-LC groups, whereas biliary dyskinesia was more common in 2I-LC and conversion groups. The odds of performing 4P-LC were greater than 2I-LC for BMI >25.0 kg/m2 and any preoperatively diagnosed complication of gallstone disease, though the opposite was true for biliary dyskinesia, and no differences noted for patients with previous abdominal surgery or planned concurrent procedures (Table 2).
BMI, body mass index.
Operative time was longer in the 4P-LC and conversion groups, compared with 2I-LC. There were no significant differences in operative time in the 2I-LC group over the years of the study (data not shown). When stratified based on preoperative diagnosis, operative time was longer in the 4P-LC group for patients with biliary colic (P = .01) and biliary dyskinesia (P = .04), but not for acute cholecystitis, choledocholithiasis, or gallstone pancreatitis. Although this study is not powered to determine differences in postoperative complications, the incidence of wound infection, small bowel injury, and common bile duct injury remained low in all three groups, in keeping with risks described previously. 10 Odds ratios of complications with 2I-LC versus 4P-LC are listed in Table 3. No patients required conversion to open cholecystectomy in either group.
Discussion
Minimally invasive surgery for gallbladder disease has become increasingly popular in pediatric patients, with advantages of less pain, shorter length of stay, smaller scars, and quicker return to normal activities.1,2,14 Although several authors have documented the efficacy of single-incision laparoscopic cholecystectomy, there are conflicting concerns regarding increased risks of pain and port-site hernia formation with a larger umbilical incision, bile duct injury, prolonged operative time, and the need for specialty ports and instruments.4–12 Visualization of the critical view is challenging with single-port laparoscopic cholecystectomy as all instruments are in line with the camera and there is reduced ability to triangulate ports.10,13,15
In this study, we describe a 2I-LC technique that uses conventional ports and allows for optimal triangulation with three handheld graspers for traction and countertraction to demonstrate the critical view, while minimizing residual scarring and maintaining cosmesis. Moreover, we demonstrate that this procedure can be performed for multiple types of benign gallbladder disease in children without prolonging operative time or increasing risks of complications and can be converted easily to a traditional 4P-LC if necessary.
Previous studies have compared traditional 4P-LC to other 2I-LC techniques that use different methods to retract the fundus of the gallbladder.16–18 Instead, we use a 2-mm grasper that has the unique advantage of manipulating the degree of fundus retraction, allowing traction and countertraction to be optimized for exposure of the critical view. We also use conventional ports and cameras obviating the need for further specialized equipment, facilitating dissemination of this technique.
Although we found no differences in operative time based on number of cases performed, the data covering the period where we began to use and refine this technique was unavailable, thus, we are unable to assess the true learning curve for this method. Despite this, we believe that the use of three working instruments and a camera via two incisions is minimally different from the use of three working instruments and a camera via four ports. This learning curve could be examined via prospective studies examining adoption of this technique in other centers or with trainees.
Our data indicate that 2I-LC can be performed with shorter operative times than 4P-LC. This is likely secondary to selection bias with the odds of performing 4P-LC instead of 2I-LC, greatest for patients with BMI >25.0 kg/m2 and preoperative diagnosis of any type of gallstone disease and least for patients with biliary dyskinesia. When stratified by preoperative diagnosis, operative time was shorter with 2I-LC than 4P-LC for biliary colic and biliary dyskinesia, and no different for all remaining gallstone complications. Previous abdominal surgery and planned concurrent procedures were not predictive of the technique performed. Operative time for patients requiring conversion of 2I-LC to 4P-LC was significantly longer than 2I-LC, but no different from 4P-LC, suggesting that difficult cases (including obese patients or unclear anatomy) are easily switched from one procedure to the other. The ability to fall back on the familiar 4P-LC approach is reassuring for surgeons interested in attempting the 2I-LC method.
There are several limitations to our study, including its retrospective nature and the aforementioned selection bias. There were a greater number of complex cholecystectomy patients, including those with obesity and gallstone disease, undergoing 4P-LC instead of 2I-LC, thus reducing the validity of direct outcome comparisons between the two methods. As a result, we can only conclude that 2I-LC is noninferior to 4P-LC as it does not clearly prolong operative time.
Although we have examined a large cohort of pediatric laparoscopic cholecystectomy patients, this study is not powered for detecting differences in complications. However, the incidence of wound infection, small bowel injury, and bile duct injury remain low, comparable to historic risk descriptions. 10 An additional limitation of this study is that long-term follow-up data are lacking. Long-term follow-up may improve the detection of delayed complications, such as port-site hernias.
Based on our experience, we recommend that 2I-LC is a viable option to reduce scarring in pediatric patients with multiple types of benign gallbladder disease, without increasing operative time or complications. Further prospective studies should be performed comparing single-, two- and four-incision techniques to examine learning curves and determine effects on immediate and delayed surgical outcomes, including postoperative pain, cosmesis, and complications such as port-site hernias.
Footnotes
Disclosure Statement
Dr. Steven Rothenberg is a consultant for Just Right Surgical. His role is not in conflict with any aspect of this study. No products from Just Right Surgical are used for the techniques described. Just Right Surgical has not had (and will not have) any impact on research conduct and manuscript preparation. All remaining authors declare that no competing financial interests exist.