
Abstract
Abstract
Purpose:
Midureteral obstruction is an extremely rare condition. This retrospective study assessed the outcomes of laparoscopic ureteroureterostomy (UU) in 13 children with midureteral obstructions.
Methods:
Records of patients with midureteral obstruction who underwent laparoscopic end-to-end UU between July 2011 and August 2015 were reviewed. The medical records comprised patient demographic data, intraoperative details, postoperative outcomes, and related complications. Renal ultrasound, magnetic resonance urography, and radioisotope renography were used for pre- and postoperative assessment. Success was defined as removal of symptomatic obstruction or improvement of hydronephrosis.
Results:
Thirteen patients from 3.0 months to 12 years old were identified: 6 patients presented with asymptomatic hydronephrosis (according to the renal ultrasonography), 3 with intermittent abdominal pain, and 2 with gross hematuria. The remaining 2 patients presented with urinary extravasation after inguinal hernia repair and the Soave procedure, respectively.
All patients underwent laparoscopic end-to-end UU. Procedures were performed using either the laparoscopic transperitoneal approach or laparoscopic retroperitoneal approach. All surgeries were performed successfully except for one case that required open surgery because of difficult anastomosis. There were no intraoperative or immediate postoperative complications. The etiology of the midureteral obstruction included congenital midureteral stricture, ureteral polyp, retrocaval ureter, and iatrogenic injury. The mean surgical time was 148.4 min, and postoperative hospital stay was 4.0–9.0 d. Postoperative outcomes were successful in all 13 patients (100%); median follow-up was 19.1 months.
Conclusion:
Laparoscopic UU was found to be feasible and safe for the management of midureteral obstruction in children.
Introduction
U
Management of midureteral obstructions presents a great challenge. Ureteroureterostomy (UU)—a procedure whereby the segments of the same ureter are reconnected (anastomosis) after excision of an obstruction—is a classic treatment option for this condition. In contrast to ureteric reimplantation, UU can often avoid the necessity for bladder reconstruction, such as creating a Boari flap. In 1992, Nezhat et al. 2 reported a case of laparoscopic resection and UU as a minimally invasive intervention for an obstructed ureter resulting from endometriosis. In 1998, he reported the first series of laparoscopic ureter anastomosis in a prospective follow-up study. Eight patients were treated by ureteral transection or resection with primary laparoscopic repair by UU; outcomes were excellent with few postoperative complications. 3 Some robot-assisted UU cases (adults and pediatric patients) were reported4–6 ; however, laparoscopic UU for the treatment of midureteral obstruction in pediatric patients is rare, and few case reports of minimally invasive surgery have been published. In 2015, Chandrasekharam 7 reported seven cases of successful repair of congenital midureteral stricture using laparoscopic surgery.
This retrospective case series outlines our laparoscopic UU technique experience of a small group of pediatric patients with midureteral obstruction; intraoperative and postoperative outcomes are highlighted.
Materials and Methods
Thirteen consecutive midureteral ureterostenosis patients ranging in age from 3.0 months to 12 years (mean age, 6.1 years) underwent laparoscopic end-to-end UU at Children's Hospital of Fudan University, Shanghai, China, between July 2011 and August 2015. Two patients were aged under 1 year.
We retrospectively reviewed the medical records, including patient images, intraoperative details, postoperative outcomes, and any complications. Ultrasound, magnetic resonance urography (MRU), and diuresis renography were used in both pre- and postoperative assessments. Among these patients, 6 were admitted with asymptomatic hydronephrosis, 5 complained of intermittent abdominal pain, and 2 had concomitant urinary extravasation from an iatrogenic ureteral injury. The two midureteral polyp cases were transferred to our division for gross hematuria.
Two patients who were diagnosed with iatrogenic injury during inguinal hernia repair and the Soave procedure underwent a retrograde ureterogram at the time of surgery. The precise location of the stricture segment was found using a retrograde ureterogram performed concurrently with laparoscopic UU. The remaining 11 patients were diagnosed with obvious dilatation of the proximal ureter in the MRU image and confirmed during laparoscopic exploratory (Fig. 1).

MRU image of a congenital midureteral stricture shows the dilatation of the proximal ureter in the MRU image. MRU, magnetic resonance urography.
All patients underwent laparoscopic excision of the midureteral obstruction combined with UU using an intracorporeal suture technique. A transperitoneal three-port laparoscopic approach was taken in all cases except for the two retrocaval ureter cases, in which the retroperitoneal approach was used. During the procedure, the retrocaval segment of the right ureter was divided and anastomosed anterior to the inferior vena cava (IVC) using 5–0 Vicryl sutures. Because of difficulty associated with the anastomosis procedure, one case was converted to open surgery. The other 12 surgeries were completed by laparoscopy without the need to convert to laparotomy and these patients had uneventful postoperative recoveries. Each resected specimen was subjected to a pathological examination to better assess the etiology of the condition.
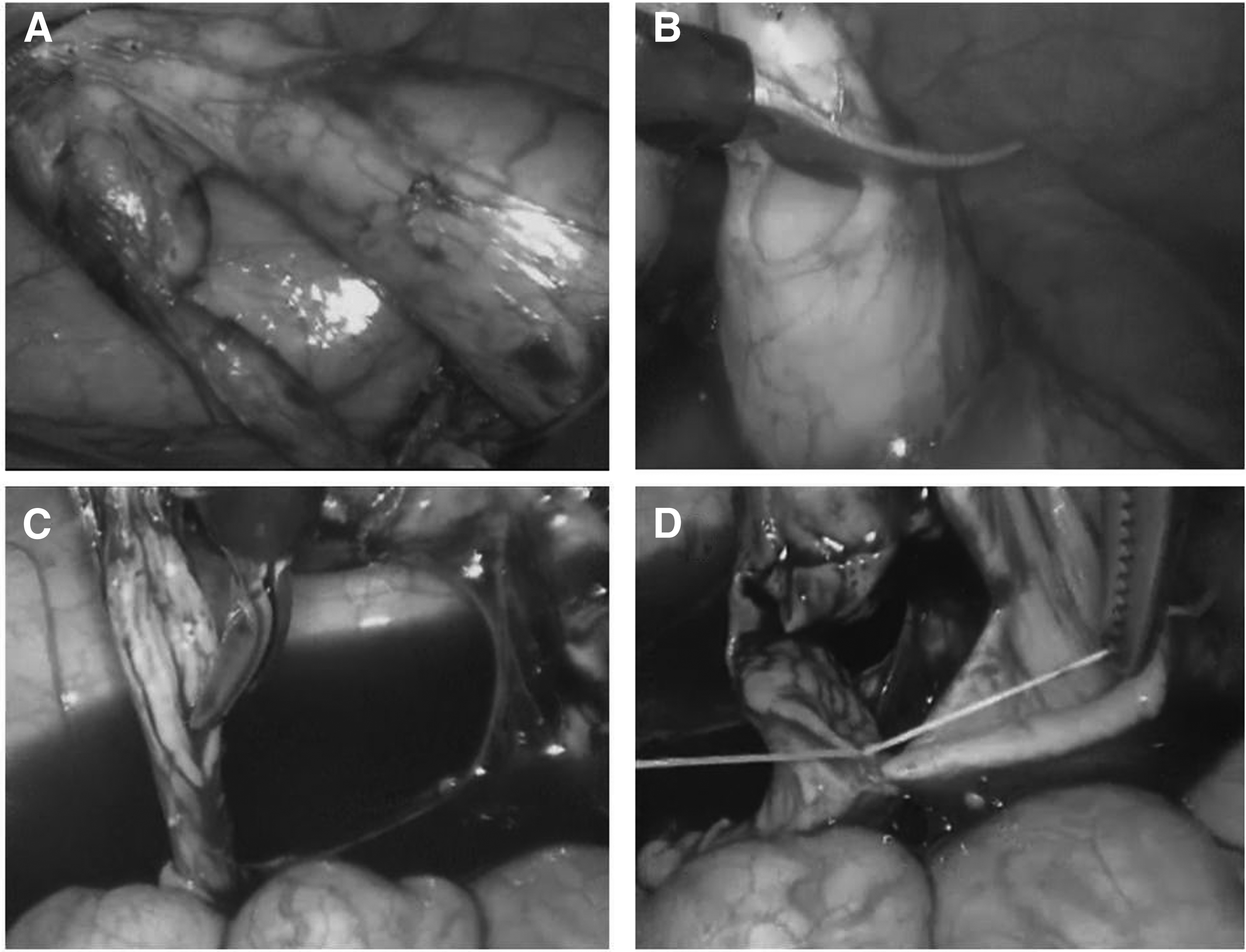
Most of the strictures were typically located at or above the entrance to the pelvic iliac blood vessels. Each blockage was removed laparoscopically, and a UU was sutured and placed over a Double-J stent. A hitch stitch was used at the proximal ureter to facilitate the anastomosis. The distal ureter far from the blockage was then divided and splayed open on its lateral wall and the UU was sutured with a single layer of interrupted 5–0 Vicryl sutures (Fig. 2). A Double-J stent was placed during the surgery using a cystoscope and removed 8.0 weeks later under anesthesia. A drainage tube was inserted during surgery and removed when drainage had ceased.
The patient was discharged 4.0–9.0 d after surgery. The follow-up plan included a regular ultrasound examination and diuresis renography at 6.0 and 12 months after surgery.
Results
The study comprised 13 patients with a median age of 6.1 years (3.0 months–12 years). Patient characteristics were reviewed retrospectively (Table 1). The lesions were on the left side of the ureter in seven and on the right side in six cases. The resected specimens were subjected to pathological examination to attempt to identify the etiology of the midureteral obstructions, which included a congenital midureteral stricture, retrocaval ureter, midureteral polyp, and iatrogenic injury.
CMUS, congenital midureteral stricture; HN, hydronephrosis; HUN, hydroureteronephrosis; LOPS, length of postoperative hospital stay; MRU, magnetic resonance urography; RLUU, retroperitoneal laparoscopic ureteroureterostomy; TLUU, transperitoneal laparoscopic ureteroureterostomy; UTI, urinary tract infection.
Of the 13 patients, 6 had a congenital midureteral stricture that was asymptomatic with severe ipsilateral obstructive hydronephrosis (APD > 30 mm) or split renal function <40% (2 patients had only one kidney). The remaining 7 patients presented with symptoms such as intermittent abdominal pain (three cases comprising two with a retrocaval ureter stricture and one with a congenital midureteral stricture), gross hematuria (two cases with a midureteral polyp), and urinary extravasation after iatrogenic ureteral injury (two cases). Two patients with a retrocaval ureter underwent laparoscopic UU using the retroperitoneal approach. Open surgery was necessary in one case because of the difficulty in intracorporeal anastomosis. The strictures in all other patients were successfully excised using a transperitoneal laparoscopic approach, and anastomosis was completed between the dilated proximal ureter and the distal ureter. The median duration of surgery in the laparoscopic UU procedures was 148.4 min (range, 90–300 min). The estimated blood loss related to the procedure was <10 mL. There were no complications during or after surgery.
One 3.5-year-old boy (patient 2) had undergone a preoperative voiding cystourethrography, and a grade I–II vesicoureteral reflux was found in the affected side because of a urinary tract infection. After surgery, repeated voiding cystourethrography showed that the reflux had aggravated to grade III because of the released midureteral stricture; however, the split renal function of the affected side had obviously improved from 10% before surgery to 19% after surgery. The conservative treatment of prescribing daily antimicrobial prophylaxis proved effective and there was no breakthrough febrile urinary infection. No other postoperative complications were encountered.
Of the two iatrogenic ureteral injury cases, one had abdominal pain and urinary extravasation after the inguinal hernia repair while the other had abdominal pain and urinary extravasation after the laparoscopic-assisted Soave procedure.
A retrograde ureterogram was performed during surgery to confirm the position of an iatrogenic ureteral injury. During the laparoscopic procedure, the iatrogenic injury position was found in both cases to be located at the entrance to the pelvic iliac blood vessels. The laparoscopic UU was completed with no complications after the resection of the midureteral obstruction.
All patients were discharged 4.0–9.0 d after the procedure following removal of the drain and urinary catheter. Double-J stents were removed cystoscopically after 8.0 weeks under general anesthesia. All patients were given prophylactic antibiotics until the ureteral stent was removed. The follow-up plan included ultrasound every 3.0 to 6.0 months and diuresis renography 6.0–12 months later.
Total follow-up was from 2.0 to 51 months (mean, 21 months). Four patients were reported to complete only a short-term follow-up (<6.0 months). The results of ultrasound evaluation during the average follow-up period showed that hydronephrosis decreased substantially. Split renal function in patients with impaired renal function improved or stabilized after surgery. Urinary symptoms were obviously relieved in those patients with abdominal pain or gross hematuria. None of the patients needed repeated surgery and none showed evidence of renal insufficiency (Table 2).
APD, anterior and posterior diameter of the renal pelvis; CMUS, congenital midureteral stricture; SRF, split renal function.
Discussion
Midureteral obstruction is a rare condition in children and adults. Ureter size, the need for careful mucosal apposition, and precise suturing all necessitate advanced laparoscopic skills for this procedure.
We believe that this study comprised the largest number of reported cases of pediatric laparoscopic UU. The location of the stricture of midureteral obstruction in our cases was similar to that described in the literature.1,8
Retrocaval ureter is relatively rare. In 1999, Salomon et al. 9 reported the first retroperitoneal laparoscopic UU for this condition. Since then, there have been some reports of laparoscopic UU in adults using a transperitoneal or retroperitoneal approach with good results.10–12 There are advantages and disadvantages to each technique and surgeons often have their own preferences. Of the two approaches, retroperitoneoscopy requires minimal dissection and avoids violating the peritoneal cavity, but the working space in which to perform the surgery is relatively limited. MRU was used to diagnose the retrocaval ureter in our study. Normally, the proximal ureter descends to the level of the third or fourth lumbar vertebra and curves back to behind the IVC, described as a type I retrocaval ureter. 13
All cases were diagnosed with midureteral obstruction following presurgery ultrasound and MRU. Two cases with iatrogenic ureteral injury were confirmed by retrograde ureterogram at the time of surgery. MRU is helpful in the diagnosis of a midureteral obstruction because it clearly shows the details of the morphology of the urinary system; however, MRU cannot assess the status of the distal ureter before surgery.
Arlen et al. 14 compared the value of an MRU with that of ultrasound and diuretic renal scan (DRS) in diagnosing ureteral strictures in children. Only 42% of these conditions were found by ultrasound or DRS. Their study concluded that MRU is an excellent protocol for assessing the entire urine-collecting system. Moreover, it provides accurate diagnoses and information for managing ureteral strictures in children.
We suggest that urinary ultrasound alone is not accurate enough for presurgery evaluation of hydronephrosis and that MRU should be the routine procedure for determining hydronephrosis and other upper urinary tract deformities.
An ultrasound used in presurgery diagnosis is rarely an accurate diagnosis of congenital ureteric obstructions. In our series, only four cases (30.7%) of dilated proximal ureter were identified using ultrasound; however, 100% were identified using MRU. Other techniques, such as the intraoperative retrograde ureteroscopy, are useful for localizing the stricture15,16; however, in pediatric patients (especially infants), ureteroscopy is not always feasible.
A retrograde ureterogram was used in our series solely for the evaluation of the precise location of the iatrogenic ureteral injury because it requires radioactive examination, which can potentially damage the child's health. We did not routinely use the retrograde ureterogram during surgery because the distal ureter could be viewed and assessed during the laparoscopic laparotomy, and it was always normal in our cases.
It is common for patients to be diagnosed with iatrogenic ureteral injuries during or after surgery. A laparoscopic approach to repair these injuries offers many possible benefits to the patients, including positive cosmetic results. Han et al. 17 studied 12 cases of ureter transections in adults that were diagnosed and repaired laparoscopically. One patient had undergone a segmental resection and laparoscopic UU for deep infiltrative endometriosis. Of the remaining 11 iatrogenic ureteral transections, 10 were repaired using laparoscopic UU and 1 underwent a laparoscopic ureteroneocystostomy. The ureteral injury was successfully repaired using the laparoscopic approach for 11 of the 12 patients. By the end of the study period, all patients had fully recovered.
Laparoscopic UU is a specialized surgical technique that has not previously been standardized. Moreover, few cases of midureteral stricture in children and subsequent laparoscopic repair have been published.7,18 Compared to open surgery, laparoscopic UU offers several advantages, such as less postoperative pain, shorter hospital stay, and less scarring. In our group, the postoperative hospital stay appeared to be a little longer, most likely because parents were anxious about their child's health and would not allow their child to be discharged early following surgery. Indeed, parents always prefer to wait for the drainage tube and catheter to be removed from the patient and for the patient to resume normal activities during the hospital stay.
Rare cases should also be carefully monitored after surgery and a delayed discharge can ensure a more thorough observation of the patient's recovery. Laparoscopic magnification allows for adequate dissection of the ureter in situ.
For successful surgery, particularly in infants, some technical protocols must be considered such as placing working ports so that suturing can be triangulated at the pelvic brim level. During surgery, the cut end of the transected distal ureter was spatulated to increase ureteral circumference at the site of anastomosis.
It is important to avoid rotation of the distal ureter, and the proximal dilated ureter should be anchored using a single transabdominal stitch to facilitate anastomosis. The structure must be carefully excised (resecting the narrow ureter completely), and the vascularity of the ureter must be preserved by restricting any separation to the focal lesion area.
In our cases, a Double-J ureteral stent was inserted retrograde to the ureter using a cystoscope when one side of the anastomotic suture was completed because it was difficult to transanastomotically place the proximal end of the Double-J ureteral stent into the renal pelvis. Some surgeons prefer to insert the stent after surgery using a cystoscope.19,20
Conclusion
To our knowledge, this retrospective study presents the largest number of laparoscopic UU cases ever reported in children and infants. It confirms that laparoscopic UU is a safe, effective, and minimally invasive option for the repair of midureteral obstruction in children and infants. MRU also plays an important role in preoperatively diagnosing this rare condition.
Retrograde ureterograms were selectively used in cases of iatrogenic ureteral injury to determine the precise location of the injury during surgery. Cystoscopy facilitated ureteral stent placement across the anastomosis and into the renal pelvis during the surgery. Few postoperative complications occurred, blood loss was negligible, and pleasingly the initial results were comparable to those of open surgery.
Footnotes
Acknowledgment
This study was supported by the Special Scientific Research Fund of Public Welfare Profession of China (Grant No. 2014136).
Disclosure Statement
No competing financial interests exist.