
Abstract
Abstract
Aim:
Laparoscopy has been widely used in surgical practice in pediatric age, and many techniques for laparoscopic hernia repair have been described till now. In this study, we compared two laparoscopic techniques performed by two surgeons; each surgeon practicing only one of the two techniques.
Materials and Methods:
A retrospective analysis was performed on the surgical charts, enrolling 71 patients with uncomplicated inguinal hernia. Patients were divided into two groups according to the type of surgery: (Group A, 24 patients aged 2 months–8 years) laparoscopic percutaneous internal ring suturing technique and (Group B, 47 patients aged 35 days–12 years) three-port mini-laparoscopic technique. The hernia sac was ligated at the level of internal ring, using nonabsorbable 4/0–3/0 suture. Any unexpected contralateral opening was repaired in the same manner for both groups. Follow-up period was 4 months–2 years and 9 months–8 years, respectively. Operative time and complications were analyzed.
Results:
Operation time (19.58 ± 7.06 minutes versus 35.87 ± 10.34 minutes, P < .001) was shorter in the percutaneous repair group. However, when subdivided by unilateral and bilateral presentation, only unilateral operative time was shorter compared to three-port group. There were no recurrences in Group A, while two recurrences occurred in Group B during the learning curve period. A contralateral opening accompanied the presenting unilateral hernia in 3 cases for Group A and 16 for Group B. One patient had to be converted open resulting from epigastric vessel injury, and postop hydrocele formation was seen in another in Group A. No intraoperative complications were seen in Group B.
Conclusion:
The overall experience shows that laparoscopic repair is a reliable approach regardless of the chosen technique. Percutaneous repair seems to be a less invasive method with shorter operative time, but it is not free of complications according to this series.
Introduction
I
The introduction of laparoscopic intervention is a milestone in understanding the concept of contemporary pediatric inguinal hernia repair. The procedure is minimally invasive, associated with less pain, and enables more rapid return to normal functional status, in addition to excellent visual exposure, minimal dissection, and improved cosmetic results compared with the conventional open surgery.8,9 Laparoscopic inguinal hernia repair in children has become a popular alternative to the open procedure with majority of parents demanding for the procedure. 10
Different surgical techniques have been introduced varying from a single stitch to a purse-string procedure using laparoscopy. 11 Several publications concerning large laparoscopic series have been published, aiming to clarify the feasibility of laparoscopic approach in pediatric inguinal hernia repair, as well as comparing laparoscopy versus conventional repair.12–14 In this study, we compared single-port percutaneous internal ring suturing versus three-port mini-laparoscopic hernia repair techniques performed by two surgeons, each surgeon practicing only one of the two techniques.
Materials and Methods
Surgical charts of seventy-one patients with an uncomplicated inguinal hernia who underwent laparoscopic repair were enrolled in this retrospective study. Patients were divided into two groups according to the type of surgery: Group A, 24 patients (aged 2 months–8 years) treated by laparoscopic percutaneous internal ring suturing technique and, Group B, 47 patients (aged 35 days–12 years) three-port mini-laparoscopic hernia repair technique (Table 1). The hernia sac was ligated at the level of internal ring, using nonabsorbable 4/0–3/0 suture material in all patients. An unexpected contralateral opening was repaired in the same manner in both groups. All patients were discharged on day of operation. Follow-up period was 4 months–2 years and 9 months–8 years, respectively. Operative time, demographic data, accompanying contralateral opening, and complications of the techniques were statistically analyzed.
IQR, interquartile range.
Laparoscopic single-port percutaneous internal ring suturing technique
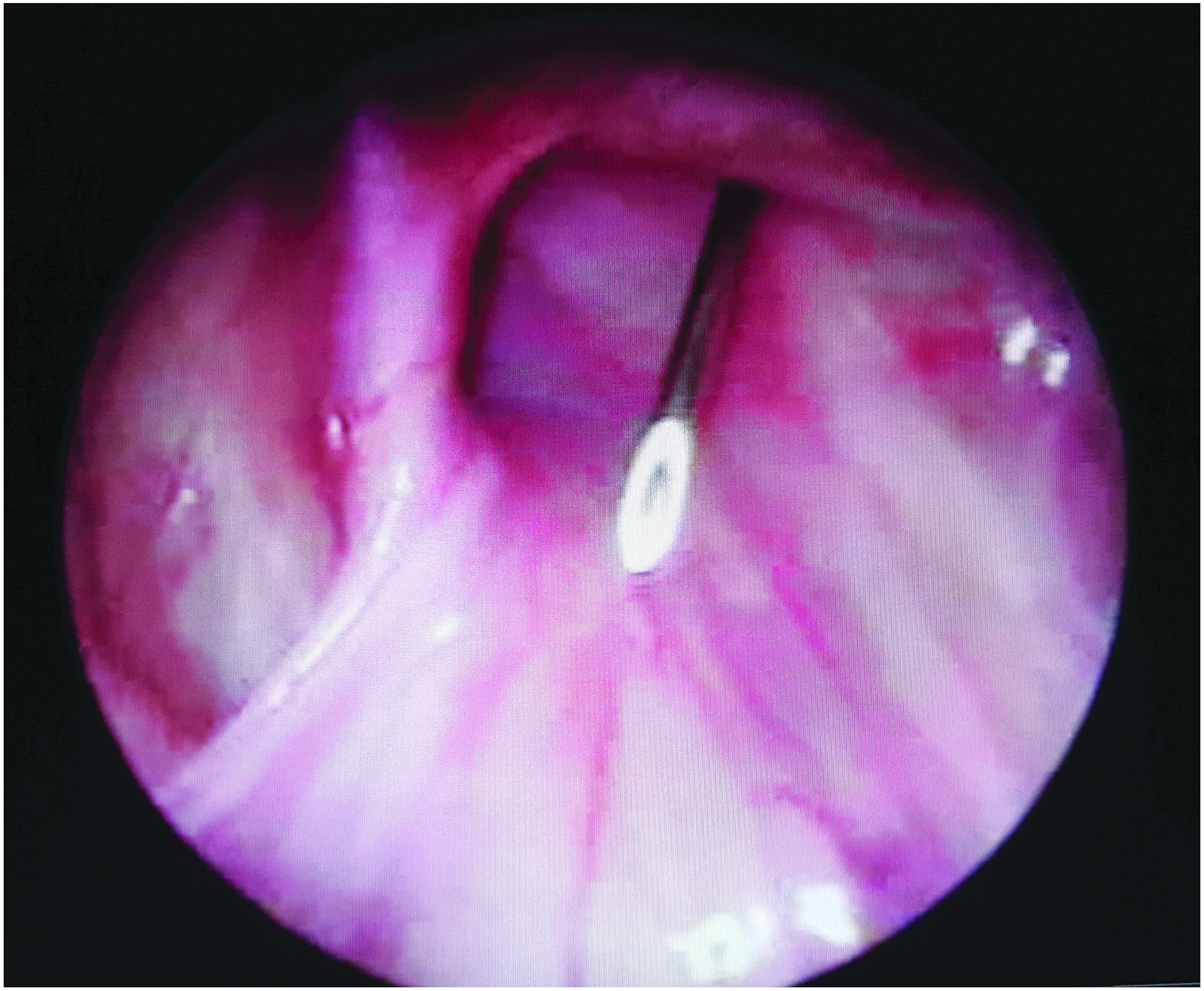
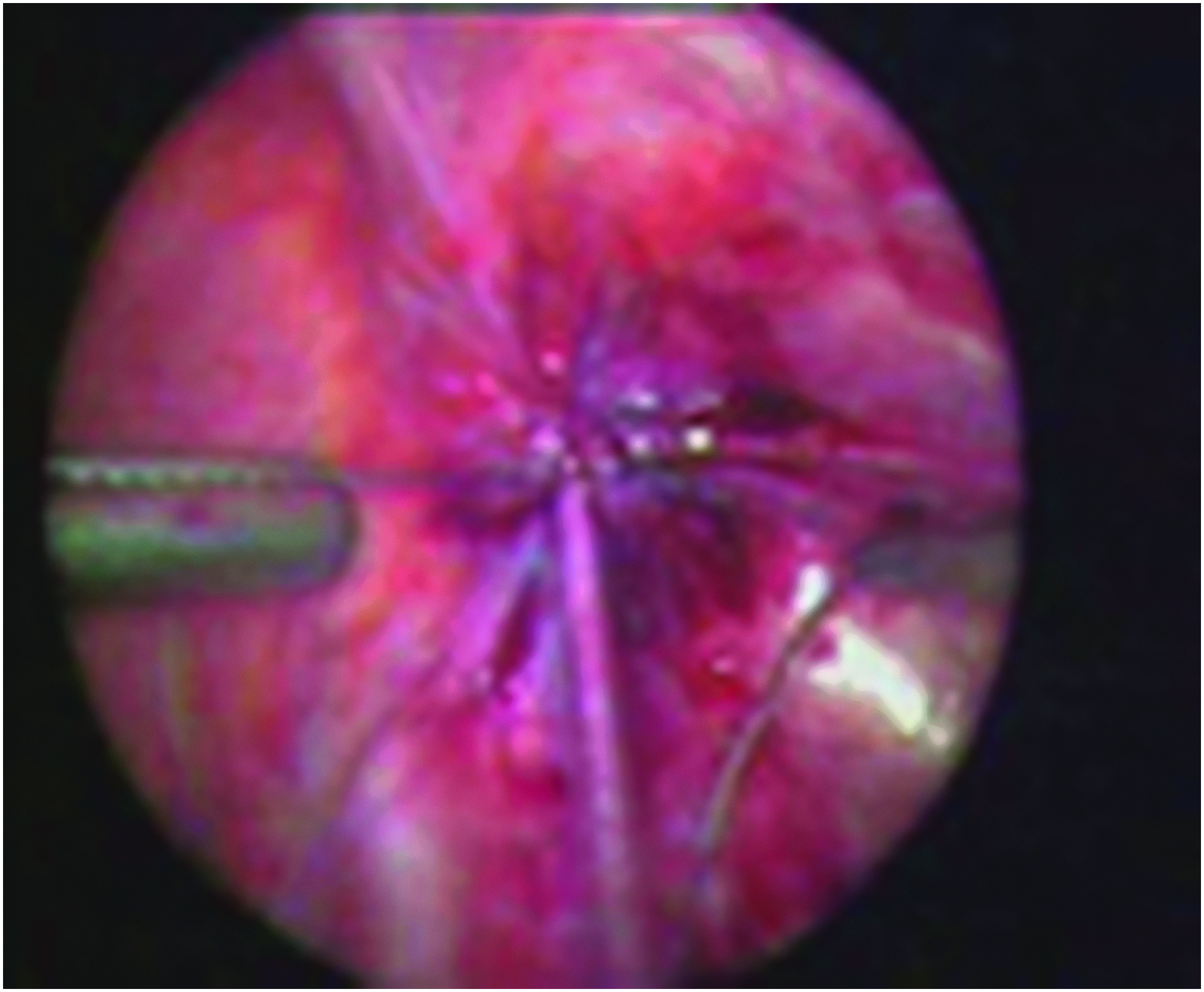
Pneumoperitoneum was created using veress needle, and the intraabdominal pressure was kept at 6–8 mmHg. The patient was placed in Trendelenburg position. A 3 mm 0° telescope was used to examine the whole abdominal cavity and pelvis. An 18-gauge angiocut needle and 3/0 monofilament nonabsorbable suture were used during repair (Fig. 1). Both ends of the suture were passed through the needle to form a loop. The needle was inserted through the anterior abdominal wall over the site of internal inguinal ring (IIR) under direct vision. The suture was placed between the peritoneum and the fascia with preservation of the testicular vessels and the vas deferens in boys. One half of the internal ring was passed, and loop of suture was pushed into the abdomen and then needle was removed. Needle was reinserted from the other side of the inguinal ring until it reached the loop. The suture tip was then pushed through needle and located inside the loop. The loop was pulled out bringing the suture tip outside while circulating the ring. Suture was secured after checking closure of the neck of the hernia, thus ligating the IIR subcutaneously (Fig. 2).

Single-port laparoscopic inguinal hernia repair and equipments.
Single-port laparoscopic inguinal hernia repair.
Three-port mini-laparoscopic hernia repair technique
An infraumbilical incision (Hasson technique) was used in obtaining an abdominal access. Pneumoperitoneum was established with carbon dioxide according to appropriate age (8–10 mmHg). Initially the abdomen was visualized using a 5-mm 30° scope with the operating table positioned in moderate reverse Trendelenburg position. Two 2.7-mm working instruments were introduced through two lower abdominal stab incisions. The needle and thread were passed into the abdomen directly through the abdominal wall. By the help of a needle holder and grasping dissector, a 3/0–4/0 nonabsorbable monofilament purse suture was sewn just around the internal ring. In doing this, the suture must not cut deep in the surrounding tissue, to enable a strong and even strangling force on the peritoneal covering of the neck of the sac. Great care was taken to exclude all cord structures and vessels along the medial aspect of the internal ring in boys. In girls, the final bite was passed through the neck of the inverted sac. The suture was then secured intraperitoneally at the base of the internal ring. The needle was retrieved through the working port, and the wounds were then closed with absorbable sutures (Figs. 3 and 4).
Three-port laparoscopic inguinal hernia repair in male patient.
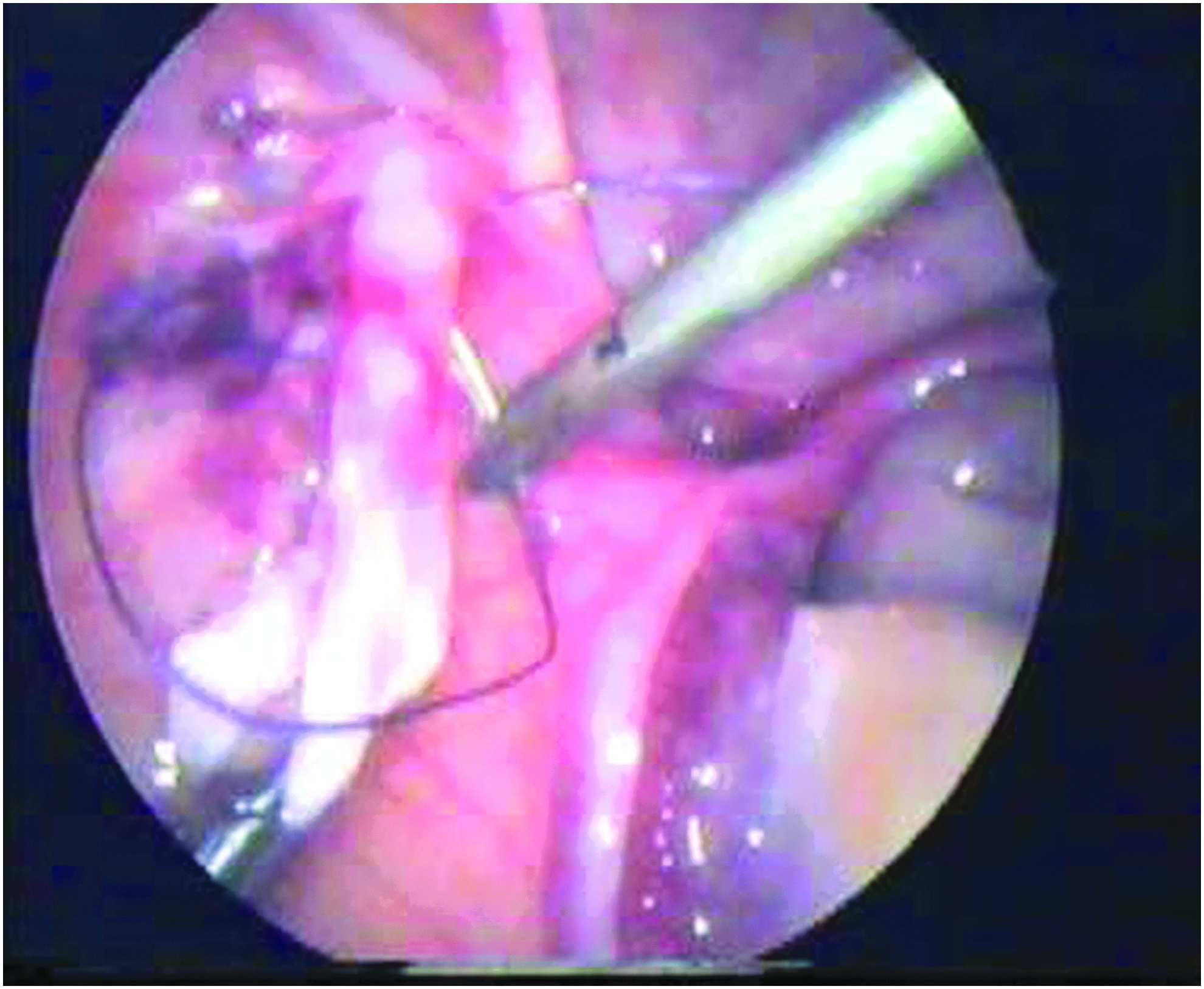
Three-port laparoscopic inguinal hernia repair female patient.
Statistical analysis
All variables are described using mean—standard deviation or percentages, properly. Only age was described with median and range. Chi-square test or independent samples t-test was used to compare variables between two surgical groups. Two-way analysis of variance (ANOVA) test was used for the effect of lateral and port groups on operation time. All data were analyzed with Statistical Package for the Social Sciences Windows version 20.0 (SPSS 20.0 for Windows; SPSS, Inc., Chicago, IL), and statistical significance was accepted at P value <.05.
Results
Table 1 shows patients' preoperative characteristics and postoperative results of Groups A and B. There was no statistical difference between two groups with regards to age, gender, lateralization, presence of contralateral patent IIR, and recurrence. Two recurrences occurred in Group B during the learning curve period. One patient had to be converted open resulting from epigastric vessel injury, and postop hydrocele formation was seen in another in Group A.
Operative details are shown in Table 2. Overall operation time was shorter for percutaneous repair compared to Group B (P < .001). However, when subdivided by unilateral and bilateral group, only unilateral operative time was shown shorter compared to Group B (P < .001). Furthermore, unilateral repair was statistically shorter compared to bilateral among Group A (18.41 ± 6.05 minutes versus 32.50 ± 3.54 minutes, P = .038).
Two-way ANOVA test was used for effects of lateral and port groups on operation time. Post hoc power analysis amongst the difference in operative times, related to port groups is 100 %, confirming the appropriate group size in this study.
Values shown in bold denote statistically significant results.
ANOVA, analysis of variance; SD, standard deviation.
Discussion
The advent of laparoscopy has changed many dogmas in all fields of surgery, including pediatric hernia repair. Many operations that were considered as “gold standard” are being challenged by the laparoscopic approach. Laparoscopic treatment, initially, has gathered much dispute as to whether it would be safe to deploy in pediatric age patients. This controversy lingered on until several reports established that this procedure was feasible and safe in children.10,14–21 The diagnostic precision of a contralateral internal inguinal opening has been mastered through hard-earned lessons, in search for a less invasive method following introduction of diagnostic laparoscopy starting from the early 1990s.22–25 The adopted regular laparoscopic closure of the IIR was usually accomplished through a three-port access. The most commonly used techniques mastered the use of two needle holders to close the IIR by either purse-string or Z-shaped suture. 20 These procedures required advanced experience in dealing with intraabdominal suturing technique using laparoscopic needle holders. In 1997, El-Gohary reported a series of 28 patients, all girls, in whom laparoscopic herniorrhaphy was performed using 1 or more endoscopic loops placed at the base of the inverted hernia sac. 26 In 2008, Schier et al. stated that laparoscopic inguinal hernia repair using suture of the internal ring does not impair testicular perfusion and this encouraged the surgeons to use laparoscopic procedure amenably. 10
As intracorporal suturing and knot tying became popular among pediatric surgeons, reported hernia recurrence rates reflected an increase varying from 0.4% to 4.1% from large series.27–28 This in turn raised the concern of the safety and effectiveness of laparoscopic repair. Recurrence was related to the skip areas during placement of purse-string sutures, as well as the tension resulting from intracorporal knotting, particularly in closure of large defects. 29 Technical modifications, including injection of saline to lift the peritoneum and the placement of single suture in N-shaped manner, have all been proposed to reduce the recurrence rates. 30
In the meantime, the percutaneous insertion of a purse-string suture under laparoscopic guidance was introduced by numerous centers.31–33 The use of extracorporeal knot tying, relative rapidity, and published results popularized this approach. The proponents of this technique state that it only requires the use of extracorporeal knotting and decreases use of working ports and endoscopic instruments.34–36 Initial reports of this technique showed a recurrence rate of 4.8%, infection, development of granuloma, and skin puckering at the site of a subcutaneously placed knot.34,37 Recent reports, however, declare the recurrence as 0.35%–1.5% and advocate percutaneous repair as a safe technique for inguinal hernia repair with respect to testicular vascularization.36,38
In the present study, all operations were performed by two senior surgeons, familiar with laparoscopic procedures, trained in intracorporal knot tying. The learning curve period depends on two factors: the surgeon's ability to reach a personal optimal operating time performance and to obtain a water tight repair to prevent a recurrence. It is justified to start practicing inguinal hernia repair in girls where there is limited risk of much feared collateral damage. Both surgical techniques are relatively safer and easier to perform in females. Author performing the three-port technique maintained an optimal operating time performance following 3 female and 5 male operative procedures. The second author maintained his personal optimal operating time performance, following 4 female and 6 male operative procedures using the percutaneous technique. The unilateral operative time for percutaneous approach was significantly shorter compared to Group B patients. This was most probably due to time consuming intracorporal knot tying procedure. Bilateral repair for both groups on the other hand showed no statistical difference. This may be due to dexterity of the surgeon while performing percutaneous repair on different sides. Although we did not compare operating time differences between presenting sides in unilateral repair, bilateral operating time for percutaneous repair was statistically longer than a unilateral repair only. Such statistical difference was not noted using three-port technique.
Both laparoscopic approaches provide easier access and excellent visual exposure to the detection and repair of contralateral patency. The techniques entail minimal manipulation of the vas deferens and testicular vessels during hernia repair, with suggested benefits of smaller scars, shorter bilateral operation times, and better chance of repair of recurrent hernias. Laparoscopy may also allow a hernia closure in an undescended testicle without compromising the forthcoming orchidopexy. 24
The recurrence rate is yet another issue and is most probably case dependent and may be confronted in any time sequence not related to operating time performance. The two recurrences happened to occur within the first eight repairs. One of the recurrent cases was a 3-month-old female with a large hernia containing ovary which was repaired in classical open manner. It was evident that the attachments between the sac and the ovary were not dissected high enough to obtain a true repair. The other was a 4-year-old male, re-repaired using laparoscopic approach. The reason for recurrence was due to loosened knot leaving a gap close to vas deferens at the level of internal ring.
The key to obtain a safe hernia repair relies on the healing process startled by firm ligation of the sac high enough at the internal ring, finally creating good re-peritonealization characterized by smooth and even surface. The inexperienced surgeon learns to feel and keep tactile control of this appropriate suture tension for obtaining an even bisecting and trans fixating force during open hernia repair. A time-consuming, complex cognitive course is required to gain this tactile sense of feeling. The shorter operative time and better recurrence rates using extracorporeal suturing technique may depend on this familiar tactile sense of feeling. The safety of a knot in a mini-laparoscopic procedure, on the other hand, relies on its limits in imitating an identical open procedure. What is meant by the “steep learning curve” is the surgeon's ability to regain expertise and persevere this mentioned, but new tactile feeling.25,39
Great care should be taken in repairing a wide internal ring with a large hernia sac. The redundant sac creates difficulty in creating appropriate sized skip areas over the vas and vessels, leading to much larger gaps rather than expected. The possibility of a slipped knot, weakness of the material used, and interference of repair technique due to anatomical variance may all have an effect in a possible recurrence beyond the expertise.
The two complications observed in Group A were also due to early phase of series. An inadvertent puncture of nearby vessels may cause serious morbidity. If this happens, gently removing the needle in exact reverse plain without tenting thus preventing a large tear may be helpful in managing a localized hematoma by the help of abdominal insufflation pressure. The observed complication risks decreased in time with increasing experience, much similar to operating times.
The overall experience obtained from this relatively small series shows that laparoscopic repair is a reliable approach regardless of the chosen technique. Although mentioned benefits, laparoscopic repair has potential risks attributable to surgeon's experience and variations in the chosen technique. Percutaneous repair seems to be a less invasive method with shorter operative time, but it is not free of complications. It is an important ethical duty for us to present the odds and evens and discuss the potential risks of each surgical approach with the family and have their consent during the decision making process.
Footnotes
Disclosure Statement
No competing financial interests exist.