
Abstract
Abstract
Purpose:
While adult bowel anastomoses are typically performed with staplers, neonatal small bowel anastomoses have traditionally been performed in a hand-sewn manner due to the large size of surgical staplers. The purpose of this study was to compare stapled anastomosis using a newly available, 5-mm laparoscopic stapler to a hand-sewn anastomosis in an open animal model.
Methods:
Twenty anastomoses were performed by two general surgery residents (10 stapled and 10 hand-sewn) in an adult New Zealand white rabbit. The small bowel was divided with a scalpel. Surgical technique was alternated between single-layer hand-sewn and stapled anastomoses. Each anastomosis was resected for ex vivo testing. Measurements collected were outer diameter of the bowel before division, time to perform the anastomosis, anastomosis inner diameter (ID), and leak test. IDs were measured by cutting the anastomosis in cross-section, taking a photograph, and measuring the diameter by computer software. In addition, the surgeons qualitatively evaluated the anastomoses for hemostasis and overall quality. Statistical significance was determined using the Student's t-test.
Results:
There were statistically significant differences between stapled and hand-sewn anastomosis, respectively, for average operative time (4 minutes 2 seconds versus 16 minutes 6 seconds, P < .01) and anastomosis ID (8.2 versus 3.7 mm, P < .01). There was one leak in the stapled group, which occurred at overlapping staple lines closing the enterotomy. A second stapled anastomosis required suture reinforcement, again at the enterotomy closure, due to operator error. Starting diameter, leak rate, hemostasis, and anastomosis quality were not statistically significant.
Conclusion:
In a neonatal open animal model, a 5-mm stapled anastomosis is an acceptable alternative to hand-sewn small bowel anastomosis. The stapler is faster and creates a larger diameter anastomosis, however, there was one leak when closing the enterotomy in the stapled group and overlapping staple lines should be avoided.
Introduction
T
One such recently available product has the potential to overcome this impediment. The JustRight 5-mm linear endoscopic stapler (JustRight Surgical, Boulder, CO) has a 5-mm shaft diameter and 2-mm staple height. Most significantly, the stapler jaws are markedly smaller than those found on both open and endoscopic staplers currently available.
This study used a rabbit animal model to compare gastrointestinal anastomoses formed using the JustRight stapler with those constructed using single layer hand-sewn technique in terms of speed, quality, hemostasis, and resultant anastomosis size. The goal was to demonstrate that the 5-mm stapler is an appropriate alternative to hand-sewn anastomosis even in the smallest of neonatal bowels. Furthermore, the stapler was anticipated to form faster and wider anastomoses. The results of this study are expected to encourage widespread adoption of the stapled gastrointestinal anastomoses in neonates and infants.
Materials and Methods
The experimental model utilized the New Zealand white rabbit (Oryctolagus cuniculus). Institutional Animal Care and Use Committee (IACUC) approval was obtained and an adult female rabbit with a mass of 3.63 kg was selected for the study. The rabbit was preoperatively medicated with glycopyrrolate, ketamine, and midazolam followed by anesthesia induction with propofol. Anesthesia was maintained with isoflurane and continuous fentanyl infusion. The rabbit was subsequently placed in the supine position and the abdomen was shaved and draped. A midline laparotomy was performed.
Beginning with the distal small bowel and moving proximally, the bowel outer diameter was measured before complete transection with a scalpel. The anastomosis was created and subsequently evaluated and scored (Tables 1–3). Finally, the segment of bowel containing the anastomosis was resected for ex vivo testing. The anastomosis type alternated between stapled and sutured. A total of 20 anastomoses were performed, 10 each of stapled and hand-sewn. Two general surgery residents performed the operations, alternating between anastomoses who was the operating and assisting surgeon. Each surgeon performed five of each type of anastomosis.
The stapled anastomoses were performed using the aforementioned 5-mm stapler in a side-to-side, functional end-to-end manner. For each anastomosis, the stapler was fired a single time in a longitudinal manner, with one jaw of the stapler in the proximal bowel limb and the other jaw in the distal bowel limb. Then, two fires of the stapler (perpendicular to the first staple line) were required to close the remaining enterotomy (Fig. 1A, B). For the second firing of the stapler across the enterotomy, the stapler was lined up in the same direction that it was fired before such that the crotch of the staple line was in contact with the crotch of the stapler (Fig. 1B). No suture was used in the formation of the stapled anastomosis. Specifically, the staple lines were not oversewn and there was no closure of the mesenteric defect.
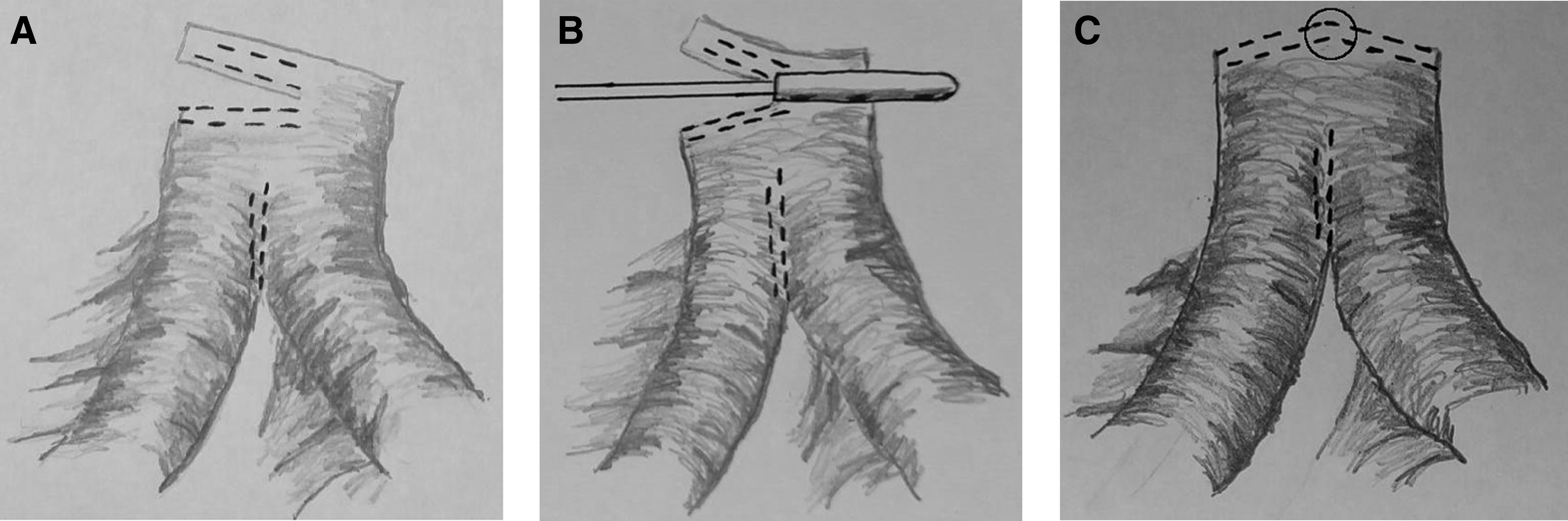
Demonstration of sequential firing of the stapler used to close the enterotomy.
The hand-sewn anastomoses were performed using 4-0 Vicryl suture (Ethicon, Somerville, NJ) in a simple, interrupted manner.
For each anastomosis, the time to complete the anastomosis was measured. In addition, the surgeon performing the anastomosis gave a numerical assessment of staple/suture line quality and hemostasis quality. Tables 1–3 detail the quality evaluation systems used.
The segment of bowel containing the anastomosis was resected and the anastomotic inner diameter (ID) was measured using a Hegar dilator. Next, a leak test was performed by clamping the proximal and distal ends of the bowel segment with hemostats. An 18-gauge needle was inserted 2–3 cm from the anastomosis and the bowel lumen was partially filled with a blue dye solution and observed for 15 seconds. The results of the leak test were categorized as “fail” if blue dye was seen to leak from the anastomosis, and otherwise was considered a “pass.”
Finally, each anastomosis was trimmed of excess bowel and was photographed (Fig. 2). Using Leica Application Suite measurement software (v. 4.7; Leica Microsystems, Wetzlar, Germany), these images were analyzed to digitally measure the bowel ID and calculate the cross-sectional area. As the area calculations relied upon the ID, this value was measured thrice in different locations and the average of the three values was used to calculate the cross-sectional area.
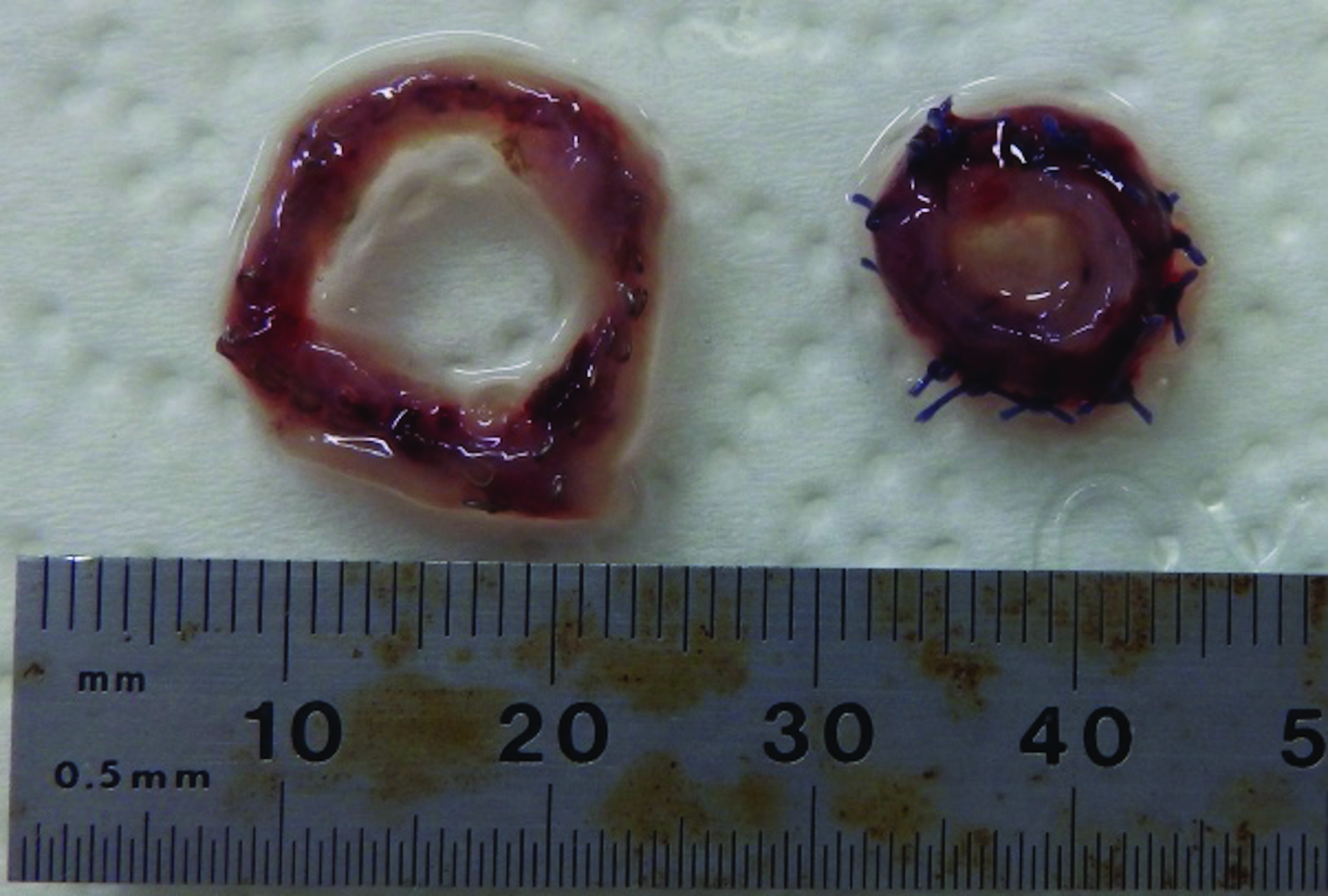
Comparison of stapled (left) and hand-sewn (right) anastomosis specimens. Note how the cross-sectional area of the stapled anastomosis is significantly larger.
As per the study protocol, the rabbit was euthanized at the conclusion of the study.
Statistical analysis using the two-sample, two-tail Student's t-test was performed using the Data Analysis tool in Excel (Microsoft, Redmond, WA). Where applicable (discussed in detail in Discussion section), the t-test was performed for unequal variances.
Results
Ten hand-sewn and 10 stapled small bowel anastomoses were performed, for a total of 20 anastomoses. The results of the study are summarized in Table 4.
σ, standard deviation; initial OD, outer diameter of bowel segment before transection time, time required to perform anastomosis; ID-Hegar, inner diameter as measured using Hegar dilator; ID-optical, inner diameter as measured using photograph and software; area, cross-sectional area calculated using photograph and software; anastomotic OD, outer diameter of bowel at anastomosis; hemostasis, hemostasis quality; quality, anastomosis quality; leak test, leak test result.
For calculations involving the leak test, “1” was used for pass and “0” for fail.
There was one leak in the stapled group, which occurred at overlapping staple lines closing the enterotomy (Fig. 1C). In addition, another stapled anastomosis required suture reinforcement at the same location (where two staple lines converged), as indicated in Figure 1C. The time for suture reinforcement of the stapled enterotomy closure was included in the anastomosis creation time.
There were statistically significant differences between stapled and hand-sewn anastomosis, respectively, for average operative time (4 minutes 2 seconds versus 16 minutes 6 seconds, P < .01), anastomosis ID measured using the Hegar dilator (10.2 versus 9.4 mm, P < .01), anastomosis ID measured using the optical technique (8.2 versus 3.7 mm, P < .01), outer diameter of the bowel at the anastomosis site (22.0 versus 13.3 mm, P < .01), and anastomosis cross-sectional area (54.7 versus 11.2 mm2, P < .01).
Starting diameter, leak rate, hemostasis, and anastomosis quality were not statistically significant (P = .36, .33, .39, and .33, respectively).
Subanalysis of the two surgeons did not demonstrate a statistical difference between the two in time to perform either type of anastomosis. Furthermore, when each individual surgeon's stapled and hand-sewn anastomoses were compared, there was still a statistical difference demonstrating a shorter time to stapled anastomosis creation.
Discussion
This study compared stapled and hand-sewn gastrointestinal anastomoses in a neonatal animal model. The stapler was not only easy to use, but also, the results demonstrated that the stapler created a larger anastomosis in a more rapid manner. The existence of a 5-mm laparoscopic stapler allows for laparoscopic creation of gastrointestinal anastomoses in neonates.
The adult New Zealand white rabbit was selected primarily for its similarity in size to the neonate. However, other important factors included prior author experience with rabbits,6,7 affordability, ease of handling and procurement, and the existence of previous rabbit surgical models to simulate pediatric gastrointestinal tract surgery.8,9 The rabbit small bowel outer diameter ranged from 10 to 15 mm, which is comparable to that of a neonate. Furthermore, the handling of the bowel was also similar compared to neonatal small bowel.
While not statistically significant, there was a trend toward improved hemostasis in the hand-sewn group. The difference in hemostasis quality is attributed to the greater time required for formation of the sutured anastomosis, which provided greater time for hemostasis to occur.
Regarding anastomosis creation time, the t-test was also performed for unequal population variance to potentially account for any potential differences between the two surgeons. However, in both cases (equal and unequal population variance), the P value was much smaller than .01.
While the diameter of the anastomoses was initially measured using Hegar dilators, this was felt to be somewhat subjective. However, all measurements were performed by one individual to reduce variability. Thus, the optical method of measuring diameter and cross-sectional area was adopted for greater accuracy.
One leak occurred in the stapled anastomosis group. This was attributed to the overlapping of the staple lines. After performing the longitudinal fire of the staple, the stapler was fired transversely across the bowel to close the enterotomy (Fig. 2). As shown in Figure 3, the stapler did not reach entirely across the enterotomy and an additional fire of the stapler, performed in the same direction, was deemed necessary (Fig. 3B). This leak was felt to be the result of failure of overlapping staple lines. Our recommendation would be not to perform sequential fires of the stapler to close the enterotomy. If a single fire of the 5-mm laparoscopic stapler is not sufficient, then an alternative technique, such as a thoracoabdominal stapler or hand-sewing the remnant enterotomy, is recommended.
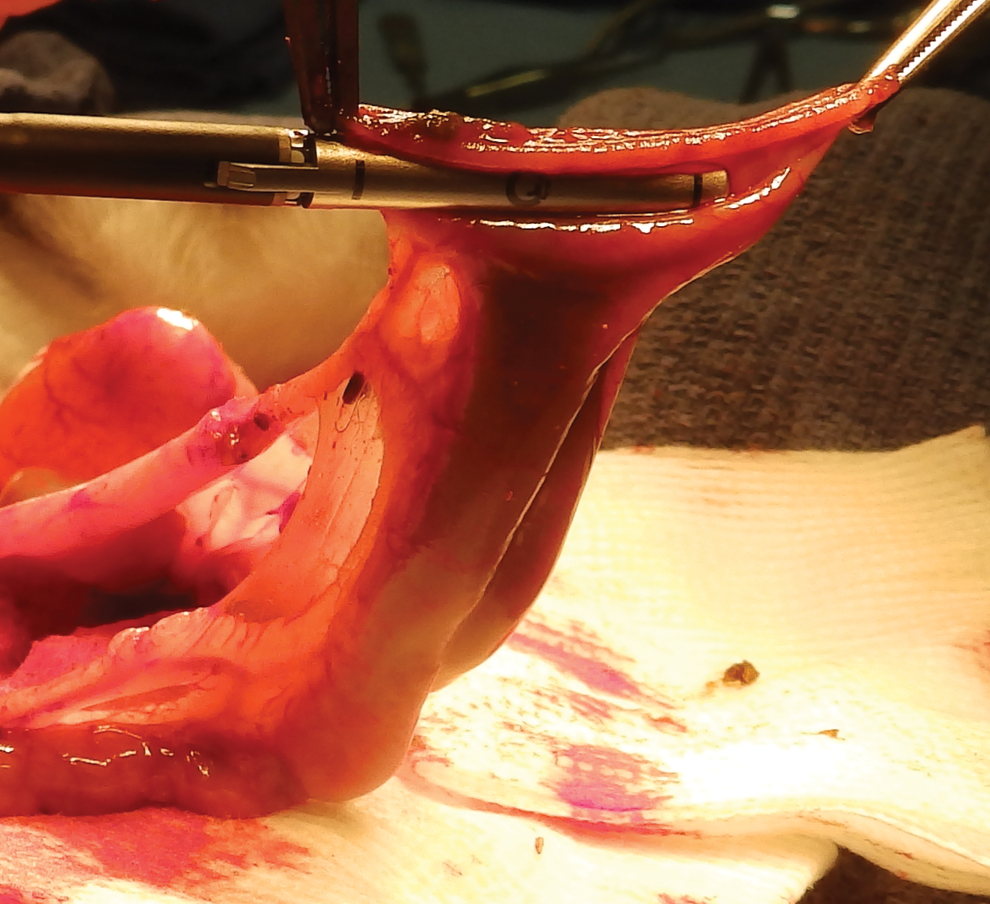
The stapler is fired transversely across the bowel to close the enterotomy remaining after the stapler has been fired longitudinally.
At present, there is no published data on long-term complications of stapled anastomoses in neonatal surgery, such as stricture formation or feeding difficulties. Further research in this area is required. Of interest, Kozlov et al. demonstrated that stapled anastomoses have comparable time to tolerance of full enteral feeds. 5
In a neonatal animal model, an open 5-mm stapled anastomosis is an acceptable alternative to hand-sewn small bowel anastomosis. The stapler is faster and creates a larger diameter anastomosis (Fig. 4).
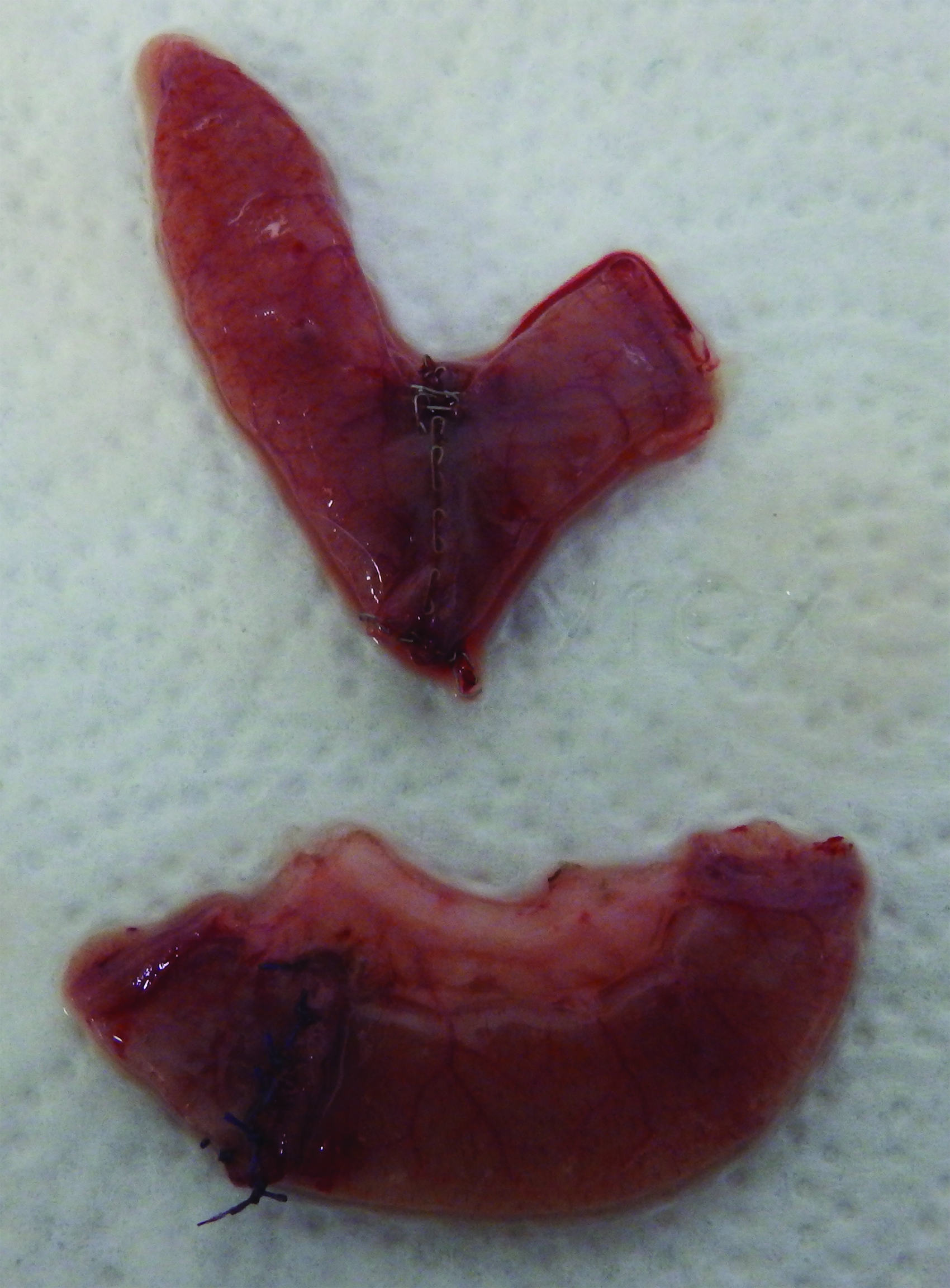
Comparison of segments of bowel with stapled anastomosis (top) and hand-sewn anastomosis (bottom).
Footnotes
Acknowledgments
This work was supported by JustRight Surgical (Boulder, CO). Special thanks to Victor C. Glenn, DDS for the illustrations.
Disclosure Statement
Dr. Glenn and Dr. Bruns have nothing to disclose. Dr. Ponsky is the cofounder and chief medical officer of GlobalCastMD.