
Abstract
Abstract
Background:
Dysphagia and regurgitation are considered typical symptoms of achalasia. However, there is mounting evidence that some achalasia patients may also experience respiratory symptoms such as cough, wheezing, and hoarseness.
Aims:
The aims of this study were to determine: (1) what percentage of achalasia patients experience respiratory symptoms and (2) the effect of a laparoscopic Heller myotomy and Dor fundoplication on the typical and respiratory symptoms of achalasia.
Patients and Methods:
Between May 2008 and December 2015, 165 patients with achalasia were referred for treatment to the Center for Esophageal Diseases of the University of Chicago. Patients had preoperatively a barium swallow, endoscopy, and esophageal manometry. All patients underwent a Heller myotomy and Dor fundoplication.
Results:
Based on the presence of respiratory symptoms, patients were divided into two groups: group A, 98 patients (59%) without respiratory symptoms and group B, 67 patients (41%) with respiratory symptoms. The preoperative Eckardt score was similar in the two groups (6.5 ± 2.1 versus 6.4 ± 2.0). The mean esophageal diameter was 27.7 ± 10.8 mm in group A and 42.6 ± 20.1 mm in group B (P < .05). The operation consisted of a myotomy that extended for 5 cm on the esophagus and 2.5 cm onto the gastric wall. At a median postoperative follow-up of 17 months, the Eckardt score improved significantly and similarly in the two groups (0.3 ± 0.8 versus 0.3 ± 1.0). Respiratory symptoms improved or resolved in 62 patients (92.5%).
Conclusions:
The results of this study showed that: (1) respiratory symptoms were present in 41% of patients; (2) patients with respiratory symptoms had a more dilated esophagus; and (3) surgical treatment resolved or improved respiratory symptoms in 92.5% of patients. This study underlines the importance of investigating the presence of respiratory symptoms along with the more common symptoms of achalasia and of early treatment before lung damage occurs.
Introduction
E
The goal of our study was to determine: (1) what percentage of achalasia patients experience respiratory symptoms; (2) what factors play a role in the genesis of these symptoms; and (3) the effect of Heller myotomy on dysphagia, regurgitation, and respiratory symptoms.
Patients and Methods
All patients with achalasia who were referred to the Center for Esophageal Diseases of the University of Chicago and underwent Heller myotomy were identified from a prospectively established database. Each patient was questioned for the presence of typical esophageal symptoms (dysphagia, regurgitation, heartburn, and chest discomfort) and of respiratory symptoms such as cough, wheezing, choking, hoarseness, aspiration, and history of pneumonia. Workup consisted of chest X-ray, barium swallow, endoscopy, and esophageal manometry. An ambulatory pH monitoring was also performed in 65 patients (39.4%) who had been treated with proton pump inhibitors on the assumption that the heartburn was due to abnormal gastroesophageal reflux. 2 All patients underwent a Heller myotomy and Dor fundoplication as previously described. 15
Statistical analysis
Continuous variables were expressed as mean or median and were compared using a nonparametric test (Mann–Whitney U test and unpaired t-test). Categorical variables were expressed as percentages and were compared using the Fisher's exact test. A P value < .05 was used for statistical significance.
This study was approved by the University of Chicago Institutional Review Board.
Results
Between May 2008 and December 2015, 165 patients with achalasia were referred for treatment to the Center for Esophageal Diseases of the University of Chicago. There were 88 men and 77 women, and the mean age was 48 years. Patients had been symptomatic for an average of 65 months. One hundred sixty-five patients (100%) complained of dysphagia and 161 (97.6%) of regurgitation. Respiratory symptoms were present in 67 patients (41%) (Fig. 1).
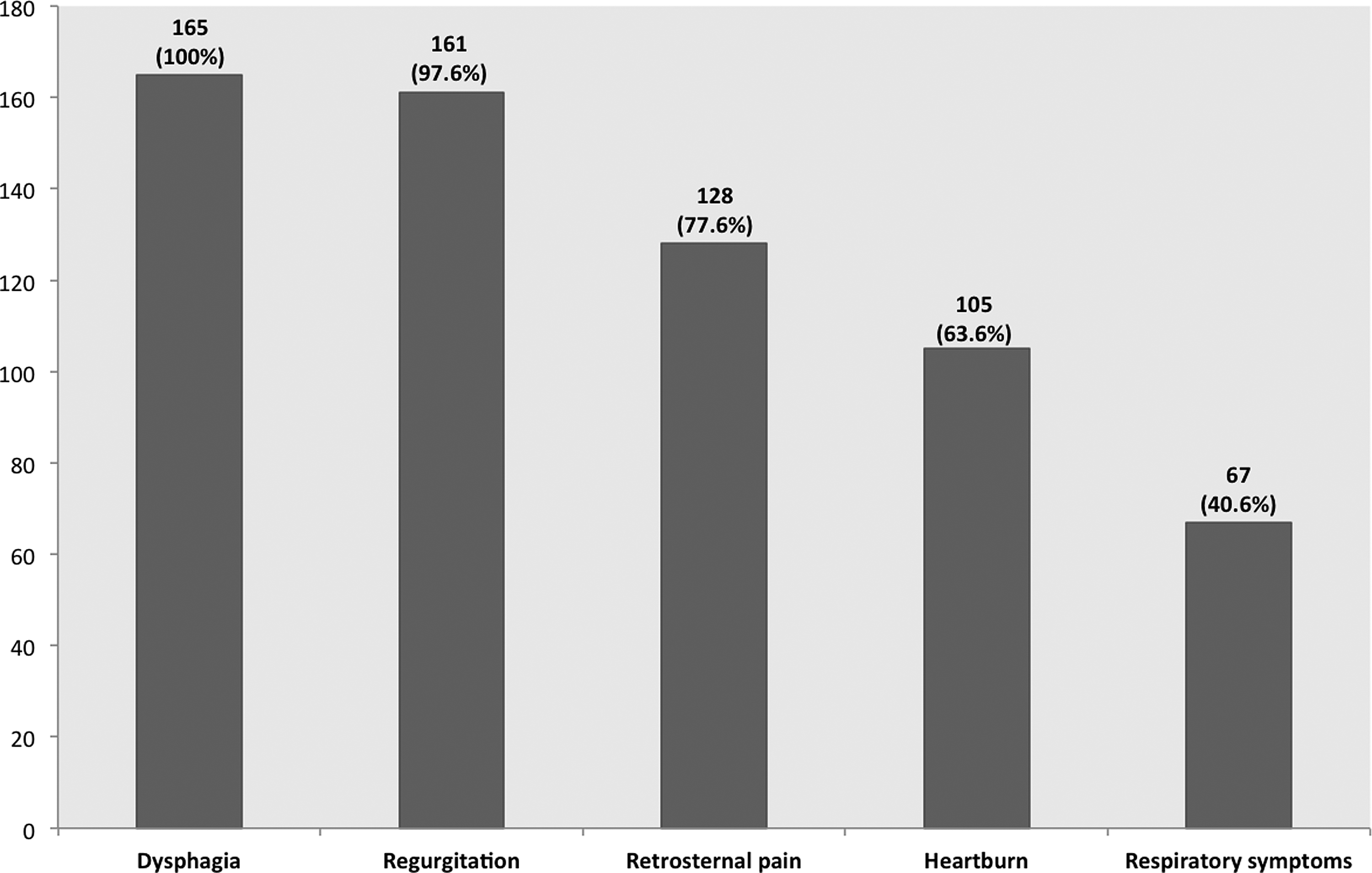
Prevalence of symptoms among 165 patients with esophageal achalasia.
Based on the presence of respiratory symptoms, patients were divided into two groups: group A, 98 patients (59%), no respiratory symptoms; and group B, 67 patients (41%) with respiratory symptoms (Table 1). Figure 2 illustrates the prevalence of respiratory symptoms among group B patients. Respiratory symptoms usually developed about 1 year after the patients experienced dysphagia for the first time.
BMI, body mass index; HRM, high-resolution manometry; LES, lower esophageal sphincter; NS, not significant; UES, upper esophageal sphincter.
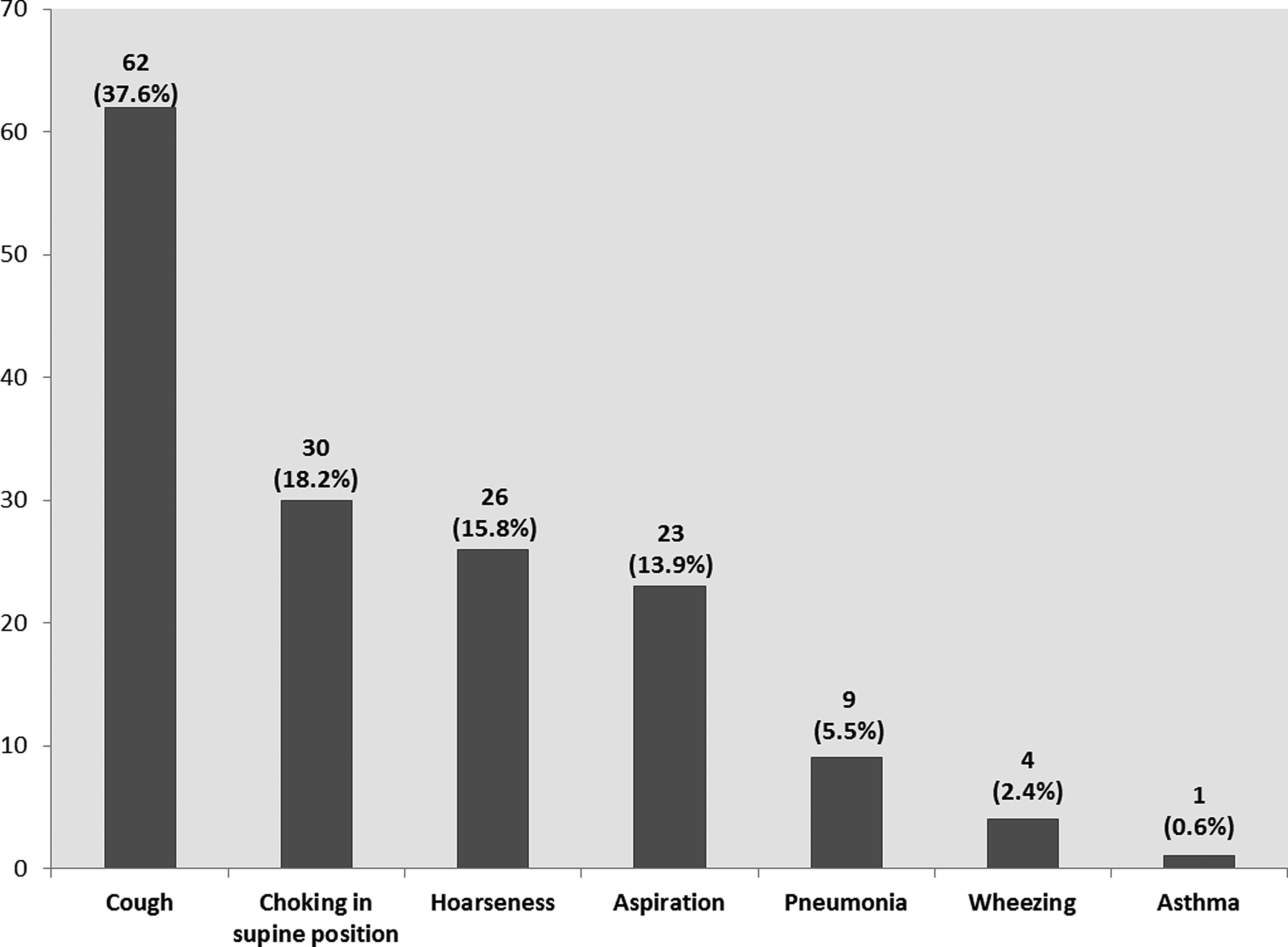
Prevalence of respiratory symptoms among group B patients.
The chest X-ray was abnormal in 3 group B patients because of the presence of peribronchial thickening and subtle ground glass opacities. The barium swallow showed that the esophagus was more dilated in group B patients (mean esophageal diameter: group A 27.7 ± 10.8 mm and group B 42.6 ± 20.1 mm; P < .05). A chest CT scan was performed in 4 patients and ruled out the presence of tracheal compression by a dilated esophagus. Conventional manometry was performed in 37% of patients and high-resolution manometry was performed in 63%. While there was no difference in the LES profile, the upper esophageal sphincter (UES) was more frequently hypotensive (UES basal pressure <42 mmHg 16 in patients with respiratory symptoms (Table 1). The ambulatory pH monitoring showed absence of abnormal gastroesophageal reflux. The Heller myotomy and Dor fundoplication were completed laparoscopically in 163 patients. In 2 patients, a laparotomy was necessary because of severe intra-abdominal adhesions and bleeding.
At a median follow-up of 17 months, 145 patients (88%) had excellent result with an ES of 0.1 (down from 6.5). Twenty patients (12%) had recurrence of dysphagia and required endoscopic treatment. Of these patients, 16 improved with an ES of 0.8; 3 patients had an esophagectomy and did well, and 1 refused additional treatment. Overall, combined treatment was successful in 97.6% of patients.
Respiratory symptoms resolved or improved in 62 (92.5%) of the 67 patients (Table 2). Most patients noted an improvement within 1 week. They stressed that they did not experience regurgitation any longer and could sleep without experiencing episodes of choking and cough. A similar improvement of respiratory symptoms was noted regardless of the type of achalasia.
Among the remaining 5 patients, 1 improved after pneumatic dilatation, 1 continued to have asthma, 1 developed bronchiectasis, and 1 had persistent laryngitis. One additional patient with a BMI of 38 had persistent cough and hoarseness secondary to pathologic reflux. This patient had been advised to have a combined myotomy and Roux-en-Y gastric bypass, but he chose to have the myotomy only.
There was often improvement in both retrosternal chest discomfort and respiratory symptoms, although we do not think that these symptoms are related.
Discussion
The results of this study showed that: (1) respiratory symptoms were present in 41% of patients; (2) patients with respiratory symptoms had a more dilated esophagus and a lower resting pressure of the UES; and (3) surgical treatment resolved or improved respiratory symptoms in 92.5% of patients.
Achalasia and respiratory symptoms
Both patients and physicians tend to focus their attention on dysphagia, clearly the most frequent and troublesome symptom of achalasia, and the effectiveness of different treatment modalities is mostly based on their ability to relieve this symptom. While in the past it was thought that respiratory symptoms were rarely associated with achalasia, today it is evident that 40%–50% of patients may also experience cough, dyspnea, asthma, hoarseness, aspiration, and pneumonia.3,4,12–14 Recently, Makharia et al. studied with pulmonary function tests and high-resolution computed tomography (HRCT) 30 patients with esophageal achalasia. 4 Seventeen patients had dry cough (56.6%). They found that 16 patients (53.3%) had either anatomical changes on HRCT or functional changes on pulmonary function tests. While direct compression of the trachea by a dilated esophagus was detected in 8 patients, 10 patients had parenchymal lung disease such as nodular opacities, consolidation, and bronchiectasis. 4 Five patients were found to have pulmonary fibrosis. Among these patients, regurgitation was common and severe, suggesting that episodes of microaspiration played a role in the lung changes. Today, there is evidence that aspiration of gastric and esophageal contents can cause a wide spectrum of respiratory disorders, from cough to lung fibrosis.17,18 Among 110 patients with achalasia, Sinan et al. reported the occurrence of at least one daily respiratory symptom in 51 of them (40%). 3
Regurgitation was present in 100% of our patients with respiratory symptoms, with choking in the supine position in 45%, suggesting that aspiration played a role in the pathogenesis of these symptoms. When we compared patients with and without respiratory symptoms, we noted that in the latter group, the esophagus was more dilated and the UES was more frequently hypotensive (Table 1). We believe that both the size of the esophagus and the pressure of the UES played an important role: a dilated esophagus allows more food to accumulate in its lumen, with a higher risk of aspiration when in the supine position and a hypotensive UES could favor aspiration, considering that this sphincter is the last barrier to aspiration. 16 We measured the UES resting pressure during a regular high-resolution manometry (10 swallows at 30 second intervals). We do not have information about episodes of UES hypotension. It is of note that in our patients, respiratory symptoms developed about 1 year after the dysphagia, suggesting that respiratory problems develop over time with the worsening of the disease. Gupta et al. also found that among 38 patients with achalasia and respiratory symptoms, dysphagia had been present for an average of 36 months, but respiratory symptoms for an average of 12 months only. 12 A similar improvement of respiratory symptoms was noted regardless of the type of achalasia. We do not believe that pan-esophageal pressurization protects against the development of respiratory symptoms.
Effect of Heller myotomy on the respiratory symptoms of achalasia
There are two possible mechanisms that may explain the development of respiratory symptoms in achalasia. The first is direct airway compression by a dilated esophagus. 19 This mechanism is quite rare, and it was ruled out by CT scan in our patients. The second mechanism is instead micro- or macroaspiration of esophageal contents into the tracheobronchial tree.3–7,11–14 If this is indeed the main cause, either pneumatic dilatation or Heller myotomy should improve or resolve these symptoms by eliminating the functional obstruction at the level of the gastroesophageal junction and improving esophageal emptying.
In our study, at a median follow-up of 17 months, respiratory symptoms resolved or improved in 62 of the 67 patients (92.5%). Specifically, none of the patients who had history of pneumonia preoperatively had a recurrent episode of pneumonia. In 2 of the 5 patients with persistent respiratory symptoms, gastroesophageal reflux developed after the operation and this was probably the cause of the symptoms.
Our findings are supported by other studies. Gupta et al. assessed the effect of pneumatic dilatation among 38 patients with achalasia and respiratory symptoms. 12 Their study included an objective evaluation of pulmonary symptoms by spirometry, chest X-ray, and HRCT scan. After treatment, symptoms improved or resolved in all patients. In addition, FEV1 improved from a median of 78% to 83% predicted and the FVC from 74% to 86% predicted. 12 Similarly, Parshad et al. treated with either pneumatic dilatation or Heller myotomy 30 patients with esophageal achalasia and noted improvement of the respiratory symptoms in 93% of patients. 13 Khandelwal et al. studied the effect of a laparoscopic Heller myotomy in 63 patients with esophageal achalasia and respiratory symptoms. The frequency and severity of all respiratory symptoms decreased significantly, and 82% of patients who reported a history of pneumonia before surgery did not experience recurrent episodes for up to 5 years after the operation. 14
Our study has some limitations. The first is its retrospective nature and the lack of long-term follow-up. The second is the lack of objective evaluation pre and after treatment of the lung function by spirometry and of the lung parenchyma by HRCT. The results, however, suggest that respiratory symptoms are frequently present and that treatment improves or resolves them in the majority of patients.
Conclusions
Forty to 50% of achalasia patients develop respiratory symptoms and can suffer severe lung damage. Because these problems present months after the onset of dysphagia, early treatment of achalasia is of paramount importance.
Footnotes
Disclosure Statement
No competing financial interests exist.