
Abstract
Abstract
Background:
Inspired by natural orifice translumenal endoscopic surgery (NOTES), the authors launched a development of novel endoscopic irrigation and suction (I/S) catheter for “laparoscopy-like” I/S in flexible gastrointestinal (GI) endoscopy. The aims were to describe its basic research and development (R&D) process and to estimate its performance in both preclinical and clinical settings.
Methods:
In basic R&D phase, a layout of side hole at apex nozzle of endoscopic I/S (EIS) catheter were theoretically calculated and designed. Material of nozzle was selected based on the strength analysis. The performance of final prototype EIS catheter was then assessed preclinically in the porcine stomach, to compare with conventional endoscopic “tip irrigation” and “tip suction” as control. After regulatory clearance, safety and feasibility of I/S using EIS catheter were clinically assessed by endoscopists in small number of patients.
Results:
Bench tests revealed 0.4 mm in diameter, 24 holes, and 6–8 holes per circumference as most suitable layout of side holes, and polyetheretherketone as an optimal nozzle material, respectively. Time to inject 500 mL saline with the EIS catheter was significantly shorter than tip irrigation (101 ± 3.1 seconds versus 154 ± 3.1 seconds; P < .05). The EIS suction was significantly weaker than conventional endoscopic tip suction, though it remained within the practical range. No mucosal injuries were noted in the EIS suction. In clinical assessments for human use, no adverse events were observed, and high degree of satisfaction for endoscopists was obtained.
Conclusion:
The newly developed EIS catheter is safely used with satisfactory performance in flexible GI endoscopy.
Introduction
N
Currently, three types of irrigation methods are available during flexible GI endoscopy. One is a direct water injection technique using a syringe connected to a biopsy channel, the second is a method using an endoscopic instrument as washing tool, and the third is a direct water supply from the distal end of the endoscope by depressing an air/water valve for lens washing. Meanwhile, suction is performed only by depressing suction valve (tip suction). The irrigation and suction (I/S) during flexible GI endoscopy has been typically accomplished by “through the scope irrigation” followed by “tip suction.” Although water syringe injection is often selected for aggressive irrigation to polluted mucosa with mucus, it is important to give attention to precise and tender irrigation, since rough water injection potentially induces mucosal damage and bleeding. As to a suction procedure, tip suction corresponds to a “diving” of endoscope beneath the fluid, which results in temporary loss of endoscopic visualization. Therefore, careful tip suction is demanded not to make a mucosal injury and/or bleeding from the lesion. Thus, indispensable I/S procedure requires a certain level of endoscopic experiences and skills for highly qualified diagnostic accuracy, especially in image-enhanced endoscopy and magnified endoscopy.
In laparoscopic surgery using rigid endoscope and instruments, I/S procedures are fundamental and indispensable as well. A quick, diffuse, safe, sterile, and precise I/S is always necessary for cases with perforation, peritonitis, and bleeding.3–6 A conventional I/S procedure from the tip of endoscope is not applicable for these situations in the peritoneal cavity, where loss of visualization might lead to further serious complications. Unsurprisingly, a variety of dedicated I/S devices or laparoscopy have been available in the market.3,7,8
Recently, a concept of natural orifice translumenal endoscopic surgery (NOTES), in which flexible endoscope is inserted into the peritoneal space, has made both gastroenterologists and surgeons “rediscover” the differences of devices and techniques between flexible endoscopy and rigid laparoscopy.9–11 As a result, its concept has triggered the positive integration of flexible and rigid devices, which has been accelerated even now. However, the integration with regard to I/S procedures and related devices have not been fully discussed yet. Against such backgrounds, the authors have developed a new endoscopic I/S (EIS) catheter for flexible GI endoscopy, which enables “laparoscopy-like” I/S in the GI tract. The aims of this study were (1) to describe research and development (R&D) process of EIS catheter in bench test setting, and (2) to assess performance of EIS catheter in both preclinical and clinical settings. The practical usefulness of EIS catheter in daily practice, and its potential usefulness in the next generation endoscopy, was also discussed.
Materials and Methods
Basic R&D in bench test settings
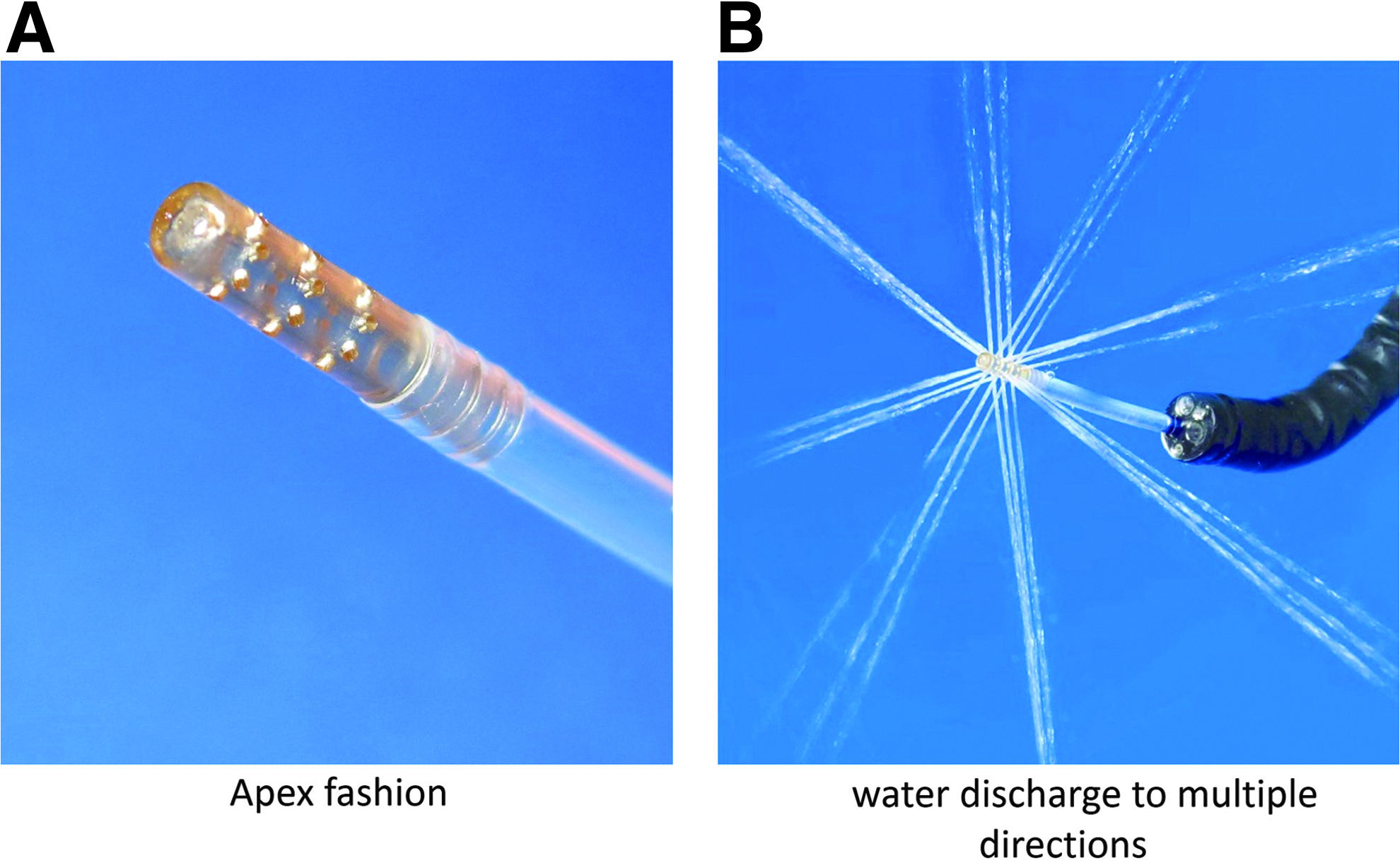
A key concept of EIS catheter is a flexible, thin, and long device passable through a working channel of standard flexible GI endoscope. For having sufficient ability of I/S and avoiding mucosal injury related to I/S, its distal portion has multiple side holes aligned in multiple directions. To develop a substantial catheter with multiple side holes, which can be unbuckled and is unbreakable, the repeated bench tests as described below were conducted. Results of these tests optimized the material and configuration of the apex of EIS catheter. The prototype of EIS catheter was processed mainly using a machining center commanded by the numerically controlled computer (XY-120; Takamatsu Machinery, Co., Ltd., Hakusan, Japan).
Bench test 1: layout of side hole at apex nozzle
The size, number, and alignment of side holes, which accomplish irrigation capability of 200 mL per minute judged as plentiful velocity, were first theoretically calculated using the following formula of Torricelli's theorem.
Correlation between scattering factor and number of side holes per circumference were also analyzed. Based on these results, the ideal size and number of side holes were determined. Fluid analysis using three-dimensional (3D) computer aided design (CAD) modeling applying to Darcy–Weisbach Equation, Bernoulli's principle, and Torricelli's theorem was performed. The specification of apex nozzle was then finalized through these repeated bench tests.
Bench test 2: material selection of apex nozzle
Based on their known physicality data (Table 1), three processable candidate materials, (1) polytetrafluoroethylene (PTFE), (2) polyoxymethylene (POM), and (3) polyetheretherketone (PEEK) were selected and served for evaluation of its rigidity, elasticity, and durability. Strength analysis showed that these materials have potential to resist the load being nearly double yield stress (data not shown).
PEEK, polyetheretherketone; POM, polyoxymethylene; PTFE, polytetrafluoroethylene.
First, catheter-like plural columnar structures, which are 2.5 mm in diameter and 40 mm in length, were manufactured using each material. Next, buckling performance was evaluated by bruising the each column. Finally, presence of deformation or breaking was checked under a pressure of 500 kPa. The most appropriate materials were determined based on these study results.
Bench test 3: assessment of degree of scatter and fluid characteristics as irrigation along with strength evaluation for preproduction prototype
A number of preproduction prototypes of EIS catheter were manufactured based on results of bench test 1 and 2. Using these prototypes, degree of scatter and fluid characteristics with regard to irrigation solution were estimated. In addition, discharge rate and pressure plus suctioning pressure were evaluated as fluid characteristics. The effects of side holes processing on strength of catheter were investigated with a tensile testing machine and compared to those of catheters without side holes (control).
Animal experiments in preclinical setting
The performance of beta prototype EIS catheter was then evaluated in porcine models following protocol approval from the Institutional Animal Care and Use Committee. The prototype catheter was connected to a commercially available laparoscopic I/S device (Strykeflow; Stryker, Kalamazoo, MI), and introduced into the porcine stomach through a standard flexible GI endoscope (GIF-Q260J; Olympus Medical Systems, Tokyo, Japan) under general anesthesia.
The time to complete I/S of 500 mL saline was measured 10 times. A conventional endoscopic “tip irrigation” using water jet pump (OFP; Olympus Medical Systems), and “tip suction” served as control.
Clinical assessments for human use
After confirmation of its fundamental performance in above preclinical settings, the EIS catheter developed in this study (Endoshower; Yamashina Seiki, Co., Ltd., Ritto, Japan) obtained authorization by Japan's Pharmaceutical Affairs Law (Fig. 1). The usability of Endoshower during esophagogastroduodenoscopy (EGD) was then clinically evaluated by the board-certified endoscopists in our university hospital. A survey was conducted immediately after EGD using three point scale questionnaires (unsatisfied, average, satisfied) with regard to (1) insertion to a biopsy channel, (2) irrigation, (3) exposure, (4) clogging at suction, (5) mucosal injury, and (6) total assessment (Fig. 2).
Endoshower:

Three point scale questionnaires for the usability of Endoshower.
Statistics
Data were expressed as mean ± standard deviation. The paired t test was used to compare the power of I/S between EIS catheter and conventional method. The analysis was carried out with JMP version 8.0 software program (SAS Institute, Inc., Cary, NC) and a two-sided P-value <.05 was considered statistically significant.
Results
Bench test 1
The calculated results using Torricelli's theorem revealed that 0.4 mm (in diameter) × 24 side holes at apex nozzle was the most appropriate layout. Figure 3 showed the correlation between scattering factor and number of side holes per circumference. No difference in scattering factor was found with more than six side holes per circumference at this analysis. The results of these bench tests demonstrated that the apex nozzle had holes 0.4 mm in diameter, 24 holes, and 6–8 holes per circumference. In addition, fluid analysis using 3D CAD modeling applying to Darcy–Weisbach Equation, Bernoulli's principle, and Torricelli's theorem showed the results similar to bench tests. The most suitable layout of side holes was determined as 0.4 mm in diameter, 24 holes, and 6–8 holes per circumference.
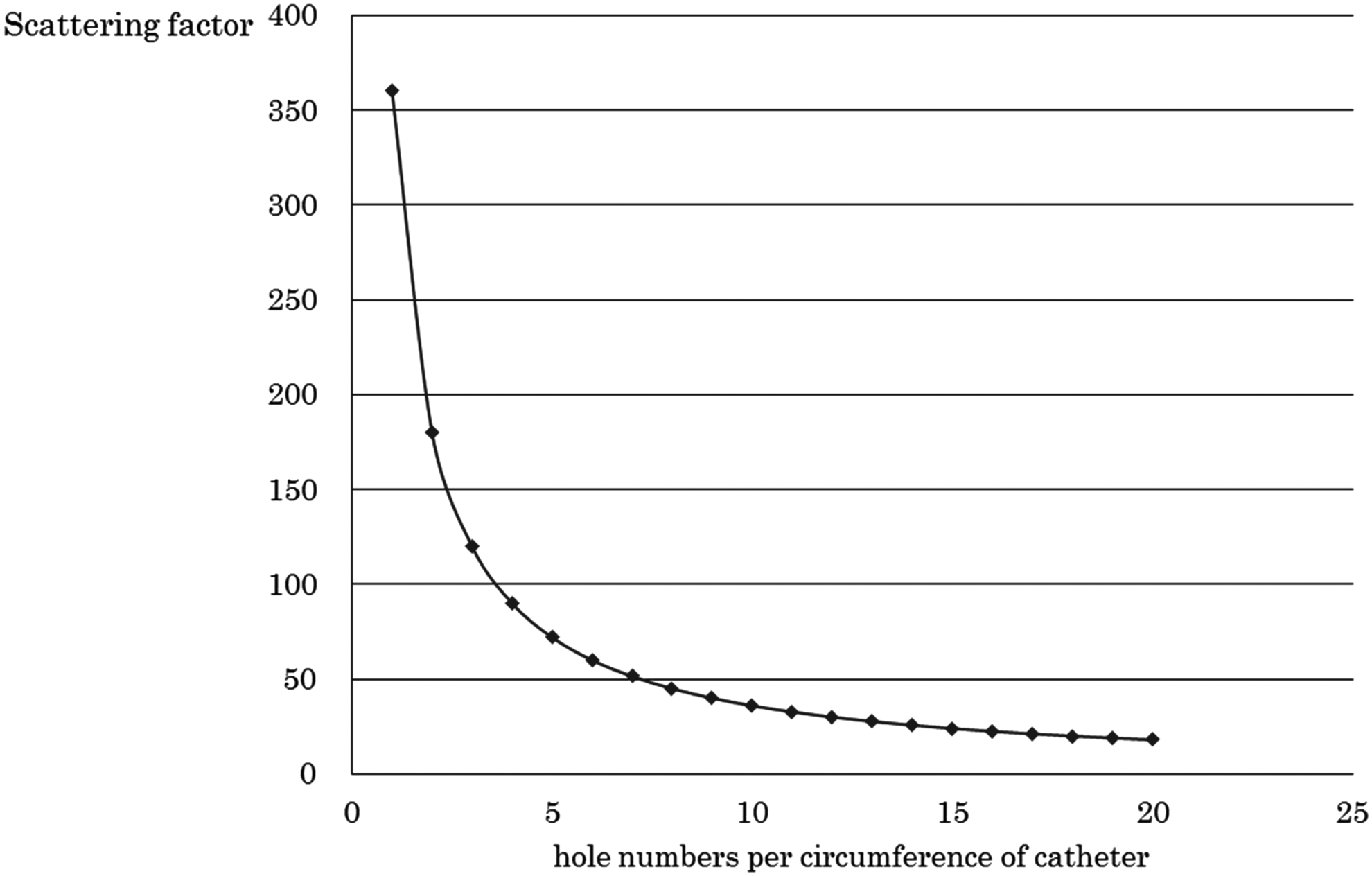
Optimization of scattering of irrigation.
Bench test 2
A column with PTFE was easy to break, whereas a PEEK showed higher buckling performance (Fig. 4). Pressure resistance test showed no deformation or breaking under a pressure of 500 kPa in each material. As per results of bench test 2, PEEK was selected for nozzle material.
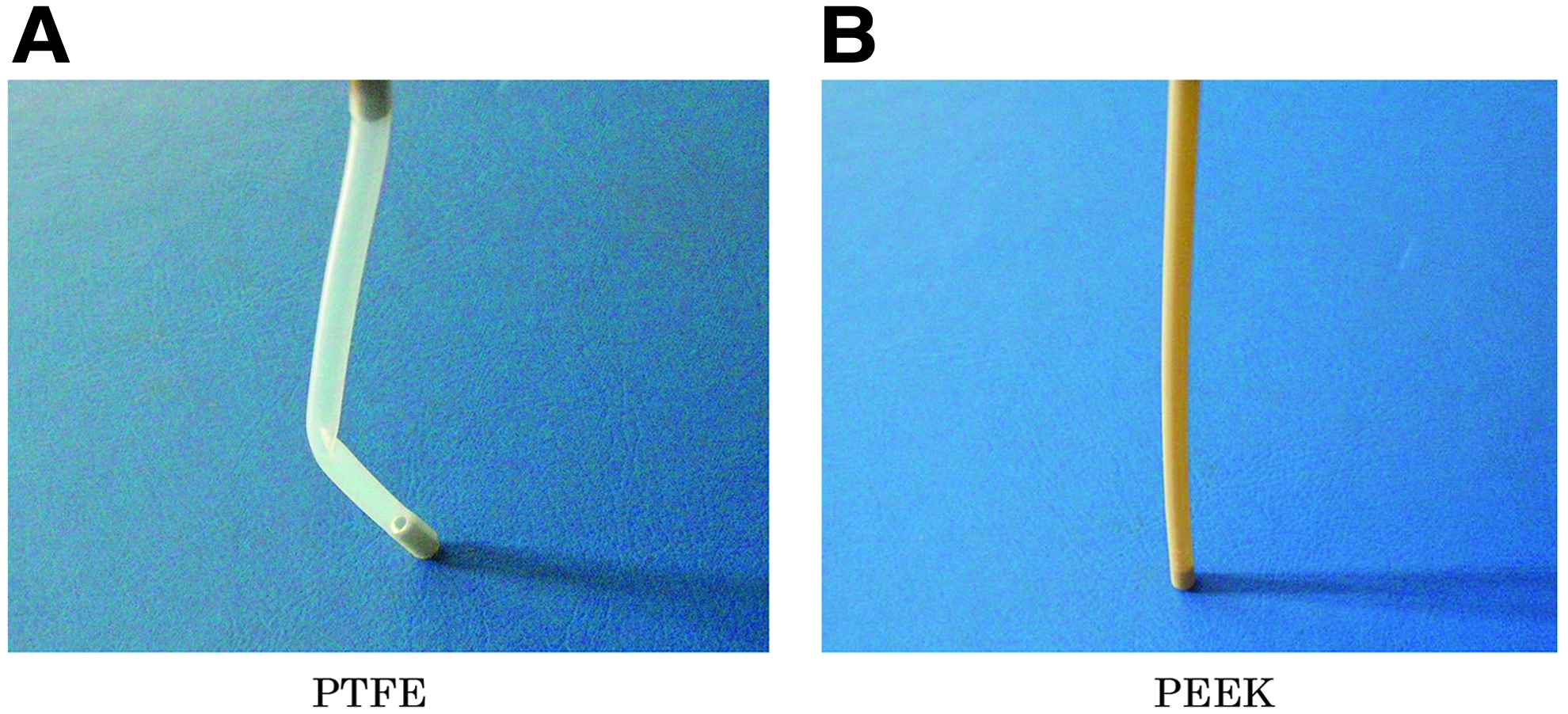
Results of buckling test:
Bench test 3
The preproduction prototypes of EIS catheter with four types of PEEK apex nozzles were manufactured (Table 2). Figure 5 showed how irrigation solution scatters in each type. Besides type 1 being comparable level of scattering to type 2, both type 1 and type 4 demonstrated favorable scattering patterns. In type 3 nozzles, columns of water from oblique holes joined together immediately after irrigation. With Type 4 nozzle offsetting the layout of irrigation angle was possible to inject multidirectionally (24 directions) although detergency decreased (data not shown). Fluid analysis with type 1 and 4 revealed that the targeted values of discharge rate 200 mL/min and suction rate 150 mL/min were accomplished by ∼35 kPa of discharge pressure and −23 kPa of suction pressure, respectively. Different layout of side holes resulted in no change on discharge rate. A tensile testing demonstrated a 23% drop in type 1 and a 36% drop in type 4 compared to a control, which could cause no serious problem in use.
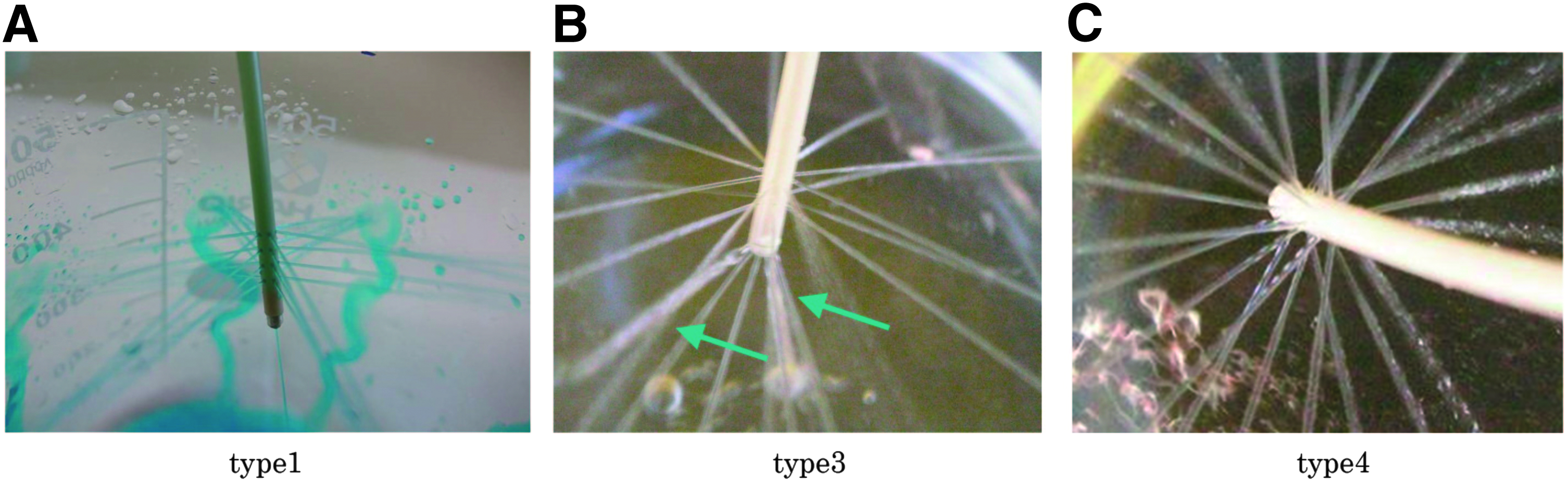
Degree of scattering from side discharge holes:
Based on above results, type 4 without an offset was considered to have excellent detergency and sufficient strength and was therefore selected as a final nozzle type of apex for the EIS catheter.
Animal experiments
I/S with beta prototype EIS catheter through flexible GI endoscope was feasible and safe in the porcine stomach. Figure 6 showed the comparison of I/S performance between the EIS catheter technique and conventional technique. Time to inject 500 mL saline solution with the EIS catheter was significantly shorter compared to tip irrigation (101 ± 3.1 seconds versus 154 ± 3.1 seconds; P < .05). On the other hand, the EIS suction was significantly weaker than conventional endoscopic tip suction, although it was still within the practical range (P < .05). In addition, no mucosal injuries were noted in the suction process using the EIS catheter. The side holes were patent throughout the I/S procedure. Diffuse and wide irrigation was possible by simply advancing/withdrawing the catheter without moving the endoscope (Fig. 7).
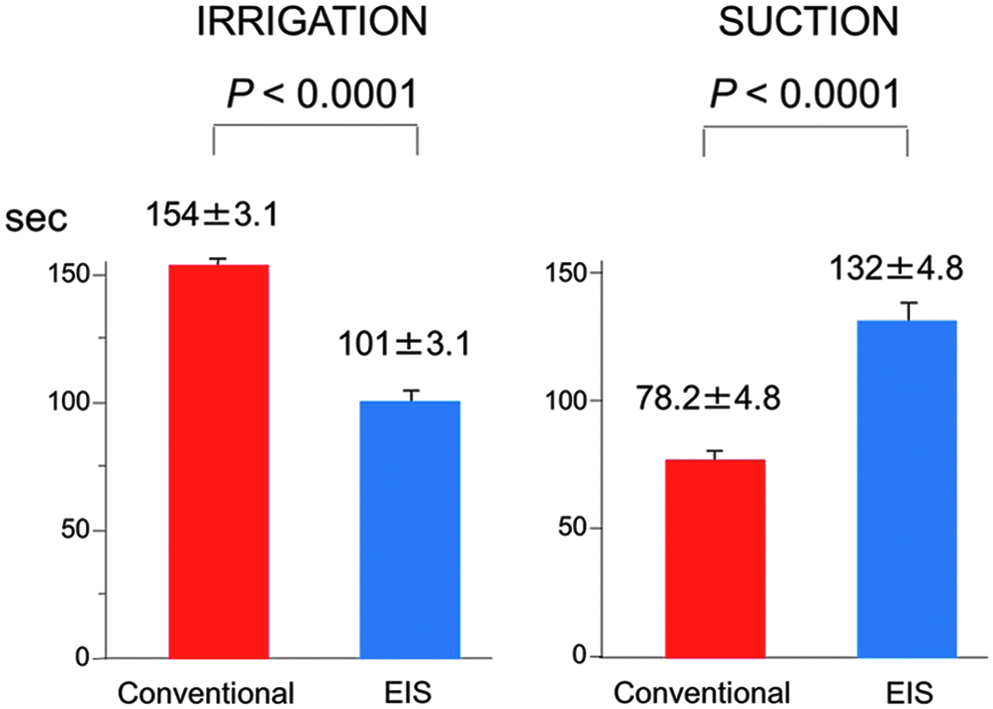
Comparison of irrigation and suction in conventional method and EIS catheter. EIS, endoscopic irrigation and suction.
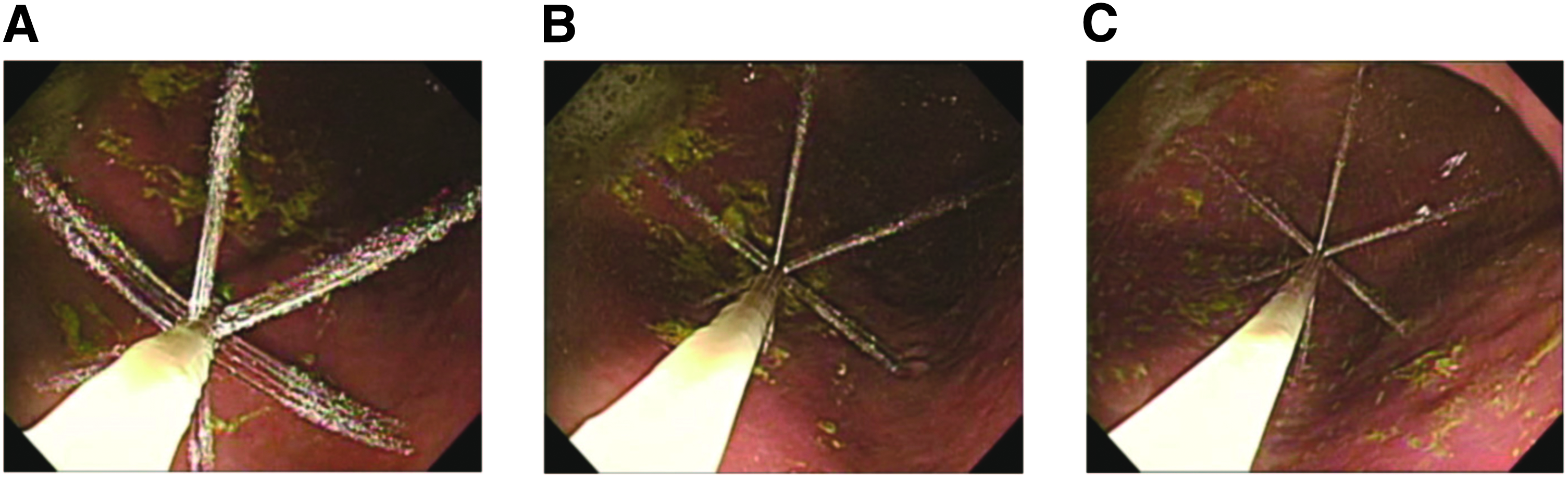
Serial photographs from
Small-scale clinical evaluation with questionnaire survey
Clinical assessments of the legally authorized EIS catheter (Endoshower) in human EGD were conducted in the form of several questionnaires for 34 board-certified endoscopists (13 gastroenterologists and 21 surgeons). EGD was performed for several different indications such as malignant diseases (n = 17), benign diseases (7), postoperative examinations (8), and GI screening (2). No adverse events related to the use of EIS catheter were encountered in this series. Figure 8 showed results of the questionnaire survey. The items evaluated as “unsatisfied” were mainly “insertion to a biopsy channel” (28%) and “clogging at suction” (13%), while other items judged as “unsatisfied” accounted for <3%. All of the reason for unsatisfied insertion was a catheter kinking at the time of initial insertion. In the total assessment, more than half of endoscopists estimated the EIS catheter as “satisfied.”

Satisfaction levels with regard to using Endoshower for endoscopists in human use.
Discussion
There exist independently evolved therapeutic systems with the different dedicated devices and peripheral equipment in both fields of flexible endoscopy and rigid laparoscopy. In general, flexible endoscopic instruments have less variations and inferior performances compared to the devices specialized for laparoscopy, since they have ordinarily long, yielding, and dainty structure to manipulate through a small biopsy channel and a thin and elongated duct line of flexible endoscope for a narrow endoluminal space. On the other hand, laparoscopic surgical instruments have wider variations and more sophisticated capability, which are not available in the GI tract through a flexible endoscope channel due to size, rigidity, and lack of length.
NOTES is a transluminal endoscopic approach without major abdominal incisions, where a current flexible GI endoscope is originally used in conjunction with dedicated endoscopic instruments.12,13 However, NOTES still remains experimental with limited clinical applications, since several studies revealed major technical challenges mainly due to lack of optimal endoscopic platform and devices. The major problems to resolve are mainly derived from the different techniques between endoscopy and laparoscopy. The introduction of NOTES has resulted in “rethinking” of current endoscopic techniques and instruments. 14 So-called NOTES revolution has thus accelerated the positive integration of endoscopy and laparoscopy into one modality. 10
A spotlight was focused on I/S in this study, which is one of the most fundamental but indispensable techniques in both GI endoscopy and laparoscopy. In flexible GI endoscopy, conventional I/S procedures have been accomplished by irrigation “through the scope” followed by “tip suction” with the endoscope being dived beneath the fluid. Such procedures lead to temporary loss of endoscopic visualization. Loss of exposure, even temporary, may cause mucosal injury, which rarely induce serious consequences in the GI tract. As to irrigation in a standard fashion, the endoscope has to move toward the target lesion, since irrigation solution is spewed from the biopsy channel at the forefront of endoscope. In contrast, several dedicated I/S devices independent from the laparoscope are available in laparoscopy, which result in robust irrigation and avoidance of false suction while maintaining the laparoscopic exposure. Based on a concept of positive integration of endoscopy and laparoscopy, we have developed a novel flexible catheter that enables “laparoscopy-like” EIS via flexible GI endoscope.
Our animal experiments demonstrated that I/S using newly developed EIS catheter was feasible and safe. The catheter was fully functioning in the endoluminal space, which facilitated rapid and diffuse irrigation and atraumatic/non-obstructing suction without moving the endoscope. In the postmarketing small-scale clinical assessments in EGD, no adverse events were observed and endoscopists obtained high degree of satisfaction. However, it was clarified that catheter was slightly easy to be kinking during insertion and several estimators controlled the endoscope during I/S procedure as usual without movement of the EIS catheter. Hence, postmarketing refinement of catheter manufacturing and learning the distinct I/S procedure with the EIS catheter would be required for amelioration and dissemination of manipulation performance.
In addition to its original usage, a “spin-off” use of the EIS catheter could be supposed in various situations. Injection of iodine or other dye staining2,15 using the EIS catheter in chromoendoscopy would provide better quality of images, since multidirectional dye spray could exert homogenous mucosa staining. All procedures consisted of I/S and dye injection in GI endoscope can be performed with only one EIS catheter and do not require a cumbersome device exchange. In the endoscopic treatment with double-channel endoscope, both of the endoscopic energy devices and the EIS catheter can be used at the same time. When smoke/mist or bleeding will occur due to mucosal incision with energy device from one channel, the EIS catheter through another channel can simultaneously evacuate smoke/mist and blood. In addition to current flexible endoscopic techniques and procedures described above, various therapeutic procedures including a flexible endoscopic robot16,17 have recently emerged from one to the next with progression of modalities, although I/S procedures are now still indispensable. After all, a novel catheter, EIS catheter, which has both I/S functions like ones in laparoscopic fields, would be required in future since present I/S procedures such as syringe injection or “tip suction” have reached the end of their tether to provide higher performances in conjunction with the newest equipment. Therefore, clinical application area of this EIS catheter is considered to be broader compared to conventional endoscopic catheters.
Costs of this new device and limitation of this study should be discussed. EIS catheter costs about 5 dollars higher than other endoscopic instruments dedicated to irrigation, although a simple comparison should not be made among these devices that have different functions. To our understanding, such a price gap could be considered as within the acceptable range, since EIS catheter has the indispensable ability of atraumatic suction, which is one of the multipurpose functions. With regard to clinical use of this EIS catheter, its true clinical efficacy has not been fully investigated in this study. A large-scale clinical assessment, ideally randomized, should be conducted by both physicians and surgeons.
In conclusion, the newly developed EIS catheter, Endoshower, is safely used with satisfactory performance in flexible GI endoscopy. Its clinical applications will be expected in various areas including next generation endoscopy including NOTES.
Footnotes
Acknowledgments
Part of this article was presented at the Euro-NOTES meeting in Rome, Italy, September 9–11, 2010. The work was supported by the grants “Strategic Foundational Technology Improvement Support Operation” (2009–2012) and “Program to Support Development of Medical Equipment and Devices to Solve Unmet Medical Needs” (2012–2013), from the Ministry of Economy, Trade, and Industry, Japan. The authors appreciate all doctors and nurses who participated in their clinical evaluation. We also thank Ms. Yumi Tsugita and Mrs. Ayumi Naito for their assistance in organizing this study.
Disclosure Statement
K.N., M.H., and N.B. received grants and payments for the development of the novel catheter. Y.M., T.T., M.Y., H.M., Y.K., S.T., M.M., and Y.D. have no competing financial interests to disclose.