
Abstract
Abstract
The light augmentation device (LAD®) is a new disposable tool designed to improve observation by transillumination in laparoscopic surgery. It can be introduced into the abdomen through an 11–12 mm port as a supplementary light source. The miniaturized design allows the surgeon to pick up the device with an endograsper and to place it under direct vision where needed. This proof-of-concept study demonstrated safety and efficacy of the device in the animal model.
Introduction
I
Today, major technological advances such as augmented-reality and fluorescence-guided imaging are polarizing the attention of industry and surgeons. However, in common clinical practice, simply improving laparoscopic observation at an affordable cost remains an unmet and important need. High light intensity is required to obtain the correct color of the visual image, and this is often limited by the narrow caliber of the optics 4 ; therefore, in some circumstances, an additional source of light may be desirable by the surgeon.
We present a device prototype (light augmentation device [LAD®]) that is designed as a stand-alone and low-cost source of cold white light for possible use in minimal access surgery.
Materials and Methods
The LAD (patent no. N102015000043649) is made of a semirigid polymer with a radio-controlled light emitted diode inside. All the plastic housings are generated by a 3D printer using a stereolitography process. The LAD consists of two separate units, one is the light source itself (length 7 cm; diameter 10.5 mm) and the other contains one or two high-capacity alkaline batteries. On bench testing, the mean duration of the battery is 60 minutes. Main characteristics of the light are the following: temperature, 4000 K; flux, 50 lm; viewing angle, 110°. The intensity of the light can be dimmed by an Android operative system application installed on a smartphone. Bluetooth transmission is provided by means of an ultralow power microcontroller that works at 2.4 GHz by an internal 32-bit ARM Cortex M3 Processor. The device will be certified according to EN60601-1.
The LAD is waterproof, atraumatic, and has a complete thermal and electrical insulation. This instrument is disposable and can be used not only in laparoscopy but also in thoracoscopy and in open surgery. During laparoscopy, the miniaturized design allows the surgeon to drop the device in the abdomen through a port, pick it up with an endograsper, and place it under direct vision where needed. The device enters an 11 and 12 mm trocar.
Experimental preclinical testing
The LAD prototype was first tested on anesthetized animals. Female domestic pigs—sus scrofa mix large white (n = 5)—were fasted overnight. General anesthesia was induced through intravenous infusion of Midazolam followed by isofluorane delivered through facemask until the animal was suitable for endotracheal intubation. Anesthesia was then maintained with continuous isofluorane in 100% oxygen. Vital signs were continuously monitored with electrocardiography leads and pulse oximetry. After establishing the pneumoperitoneum, two 12 mm and two 11 mm trocars were inserted into the abdomen. A 10 mm/30° laparoscope was used for observation. At the end of the laparoscopic phase, laparotomy, thoracoscopy, and thoracotomy were performed for further testing. Video recording of the procedures was obtained to document the performance of the LAD.
Another set of experiments was done on unembalmed fresh-frozen male cadavers (n = 2) tested negative for infectious diseases and obtained from donors who donated their body to science (without financial compensation) and signed donor consent forms in accordance with all federal laws and the Uniform Anatomical Gift Act. Cadavers were obtained from MedCure, Portland, OR. The pneumoperitoneum was established using an open technique. Two 12 mm and two 11 mm trocars were inserted into the abdominal cavity and a 10 mm/30° laparoscope was used for observation.
Five variables describing the physical characteristics of the LAD and the ease of insertion and manipulation of the device inside the abdominal cavity were scored on a 0–10 visual analog scale (0 = worst, 10 = best) by 5 surgeons with expertise in advanced laparoscopic procedures. The safety profile of the LAD was evaluated by monitoring mechanical/thermal tissue trauma. Evaluation forms were filled out anonymously by each assessor. The protocol was reviewed and approved by the Internal Board Review of the Biotechnology Center at A.O.R.N. “A. Cardarelli” in Napoli, Italy, where all the experimental studies were performed. Raw score data were analyzed using the Kruskal–Wallis rank sum test to assess consistency of measurements among the individual surgeons.
Results
The median duration of the laparoscopic procedure was 87 minutes (range 75–120). All animals survived to the intended end point and were suppressed upon completion of the experiments. The human cadavers received cremation after the procedure. No mechanical or thermal injuries due to the LAD occurred. The estimated mean score of each considered variable ranged from 7.9 to 9 with standard deviations between 0.6 and 1.4. There was no statistical difference among the evaluations given by the surgeons (Table 1).
SD, standard deviation.
Discussion
Effective illumination of the surgical field is the main prerequisite for safe and efficient laparoscopic surgery. Besides the lack of tactile perception, the laparoscopic surgeon has to cope with a restricted two-dimensional vision and a limited workspace compared with open surgery. In addition, he/she needs to maintain dexterity and hand-eye coordination while handling the minimally invasive instruments. Often, the target area is outside the reach of the optic, or the light provided by a small (<10 mm) telescope is not adequate for a proper illumination of the operative field. This proof-of-concept study suggests that a supplementary and stand-alone light source in the abdominal cavity may be useful to improve visibility in difficult anatomical areas and to provide transillumination. Our data indicate that preclinical application of the LAD was feasible and met the expectations of a panel of expert surgeons.
The LAD has been designed to be used as an ancillary light source inside the abdominal cavity. The wireless module is ideal for the application where long battery time and a small volume device are important. The potential applications for this device are listed in Table 2. In our preclinical tests, transillumination using the disposable LAD system has been shown to be feasible, easy and quick to perform, and effective. Dimming or turning off the main laparoscopic light source facilitates viewing of the target area by translucency. The light intensity of the LAD can be modulated to correct for tissue thickness. This allows to replicate the typical transillumination maneuver that is performed during open surgical procedures on the bowel by simply moving the scialytic lamp to retroilluminate the mesentery (Figs. 1 and 2).
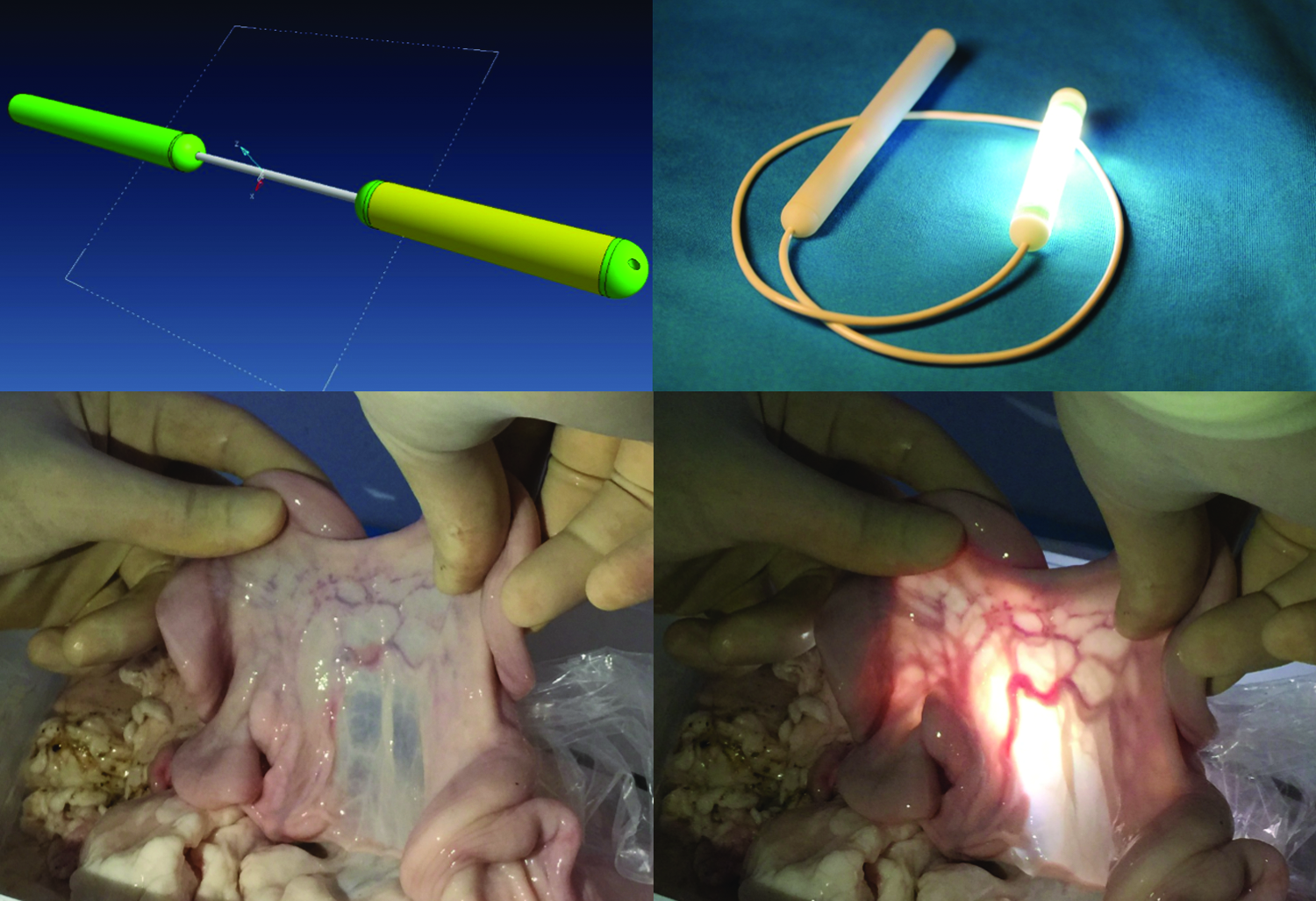
TOP: LAD: computer-aided drawing (left) and the actual prototype (right). BOTTOM: Bench testing in the dry laboratory: transillumination of the mesentery of the small bowel. LAD, light augmentation device.
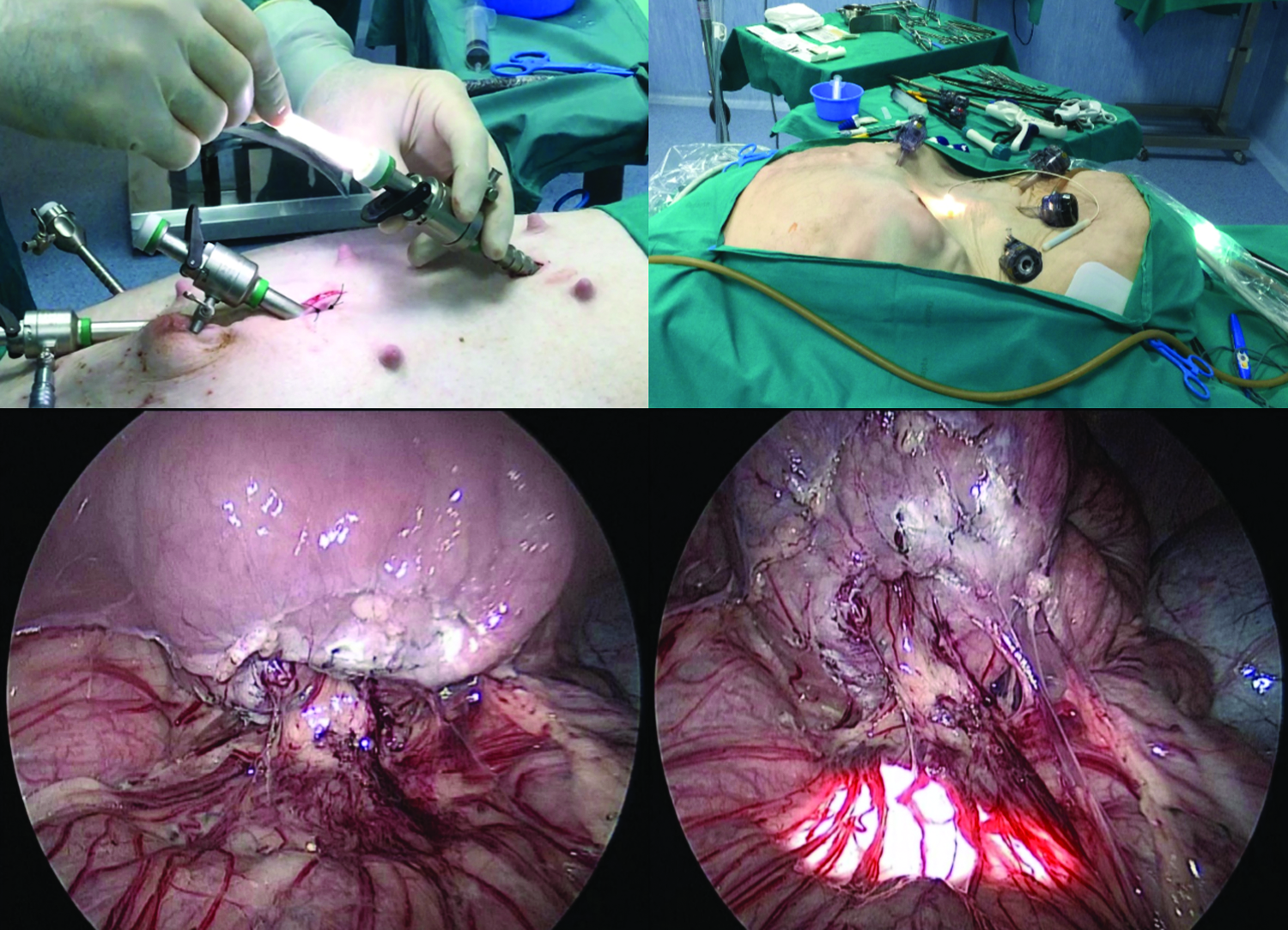
TOP: Introduction of the LAD through 11–12 mm ports in the pig (left) and human cadaver (right). BOTTOM: Transillumination of the swine mesorectum.
LAD, light augmentation device.
Conclusions
The LAD is a simple, effective, and low-cost disposable equipment. It should be considered an ancillary light source to provide transillumination or to augment white light in difficult-to-reach anatomical areas during laparoscopic or open surgical procedures. Next steps of LAD development include (a) sterilization, (b) modulation of light frequency, and (c) clinical validation. CE mark is pending. Interestingly, this technology has the potential to become an effective, stand-alone, light source device for improved laparoscopic observation.
Footnotes
Disclosure Statement
No competing financial interests exist.