
Abstract
Abstract
Introduction:
Blood loss is associated with postoperative morbidity and mortality. Outflow control could be used concomitantly with inflow control for maximum reduction in blood loss during parenchymal transection. However, in left hepatectomy (LH) and left lateral sectionectomy (LLS), extrahepatic control of the left hepatic vein (LHV) is still less commonly used. Some authors reported extrahepatic LHV control technique using ligamentum venosum (LV) in open or laparoscopic surgery, but no reports of this technique in robotic surgery have been found.
Materials and Methods:
The dissection of LV from the liver was performed, followed by clipping and transecting LV. The cephalad LV stump was retracted to the left inferior direction and then the dissection of the posterior part of LHV was performed until the opening space was connected to the anterior part of LHV. The LHV was encircled with the tape and vascular stapler was inserted to manage LHV stump. From 2013 to 2015, LHV was successfully encircled by using this technique in 7 out of 11 cases. The mean operative time was 244 minutes, the mean estimated blood loss was 300 mL, and the mean length of hospital stay was 4.8 days. Neither injury to LHV, nor complications related to the liver were found.
Discussion and Conclusion:
From our experiences, LHV was routinely controlled in robotic LH or LLS and the success rate was 60%. However, this technique is not recommended for the tumor that compresses or abuts LHV/LV, and in cirrhotic liver with associated hypertrophic left lateral segment.
Introduction
I
Materials and Methods
Operative details
The robotic liver resection in our hospital was performed by applying the da Vinci Surgical System® (Intuitive Surgical, Sunnyvale, CA). Videos of patients who underwent robotic LH between 2013 and 2015 were reviewed. The patients were placed in a supine position and five trocars were placed as shown in Figure 1: two 12-mm ports and three 8-mm robotic arm ports. Pneumoperitoneum was created by Veress needle insertion at the left subcostal area. Camera port was inserted at the subumbilicus and a 30° robotic camera was used. The first and the second robotic arm ports were placed in left and right upper quadrant areas, respectively. The third robotic arm port was placed in the left upper quadrant at the anterior axillary line. The assistant port was placed at the right lower quadrant between the camera and the first robotic arm port. We used monopolar curved scissors on the first robotic arm and the Gyrus PK bipolar forceps on the second. The robot was docked over the patient's head. The left lobe of the liver was mobilized by dividing round ligament, falciform ligament, left triangular ligament, and left coronary ligament with cautery scissor. The loose connective tissue surrounding the anterior surface of LHV and MHV was carefully dissected until MHV, LHV, or CT were exposed as much as possible. Left Glissonian pedicle was dissected, encircled, secured by Hem-o-lok clip and divided. LV was exposed by elevating left lateral section and dividing gastrohepatic ligament (Fig. 2). Then, the dissection and detachment of LV from the liver was performed (Fig. 3), followed by clipping and transecting LV close to LHV. The cephalad LV stump was retracted to the left inferior direction that counteracted with left lateral section and LHV resulting in opening up dissecting space between LHV and inferior vena cava (IVC) (Fig. 4). This could avoid injury to the posterior part of the LHV during dissection. After dissecting the posterior part of LHV, this space could be connected to the anterior part of the dissected LHV. A tape was placed around the LHV and created ∼1 cm space that was enough to divide and manage LHV stump by inserting vascular stapler (Fig. 5). The division of LHV was always done after left Glissonian pedicle was divided so as to prevent left lobe of liver congestion. Finally, parenchymal transection was performed along the MHV root down to its distal by robotic arm crushing. The robotic Gyrus PK bipolar forceps were used to treat minor bleeding. A drain was inserted and the specimen was removed through a suprapubic incision by using retrieval bag.

Schematic diagram of trocar placement. C, camera; A, assistance; 1st A, 1st robotic arm; 2nd A, 2nd robotic arm; 3rd A, 3rd robotic arm.
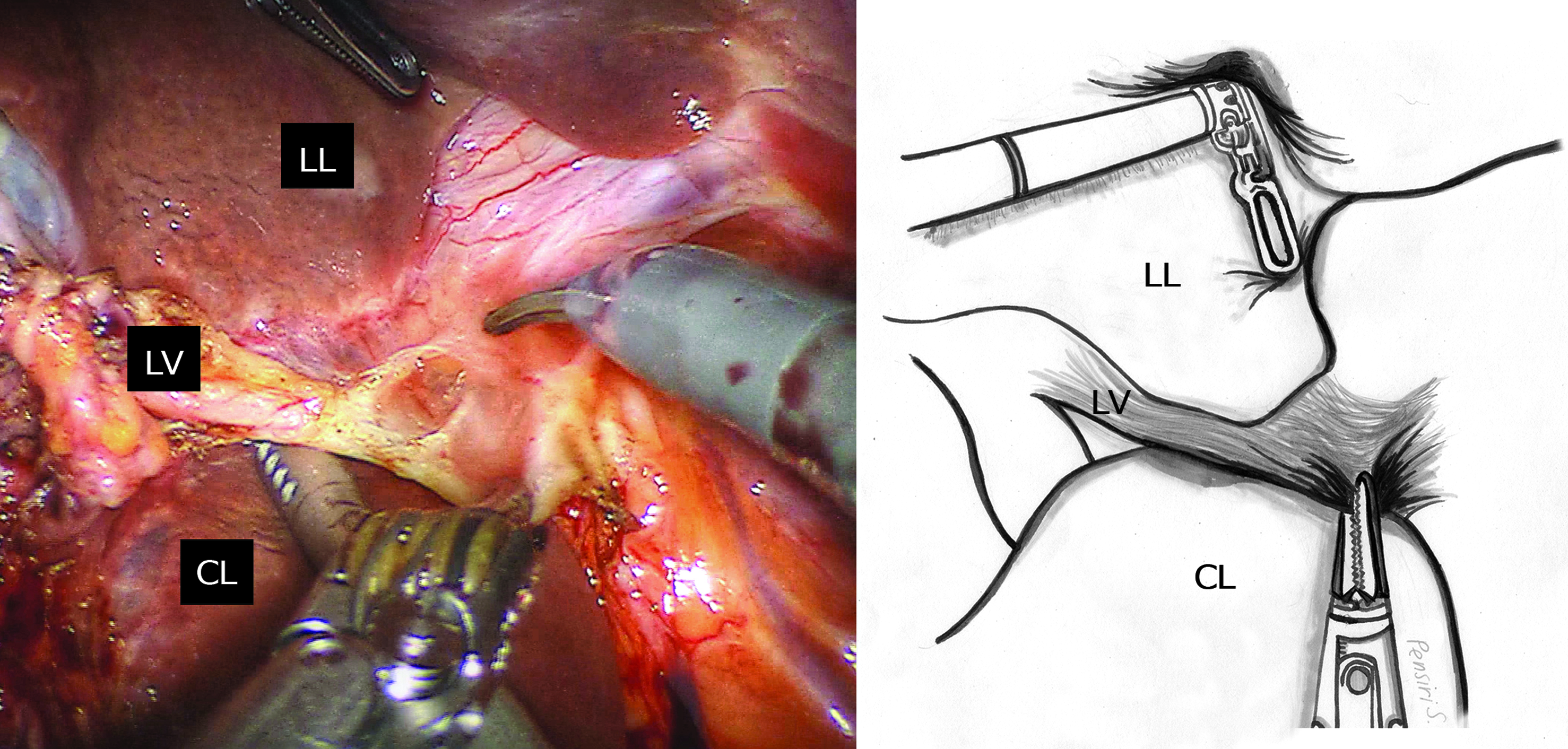
Exposing LV by elevating left lateral section of liver. CL, caudate lobe; LL, left lobe of liver; LV, ligamentum venosum.
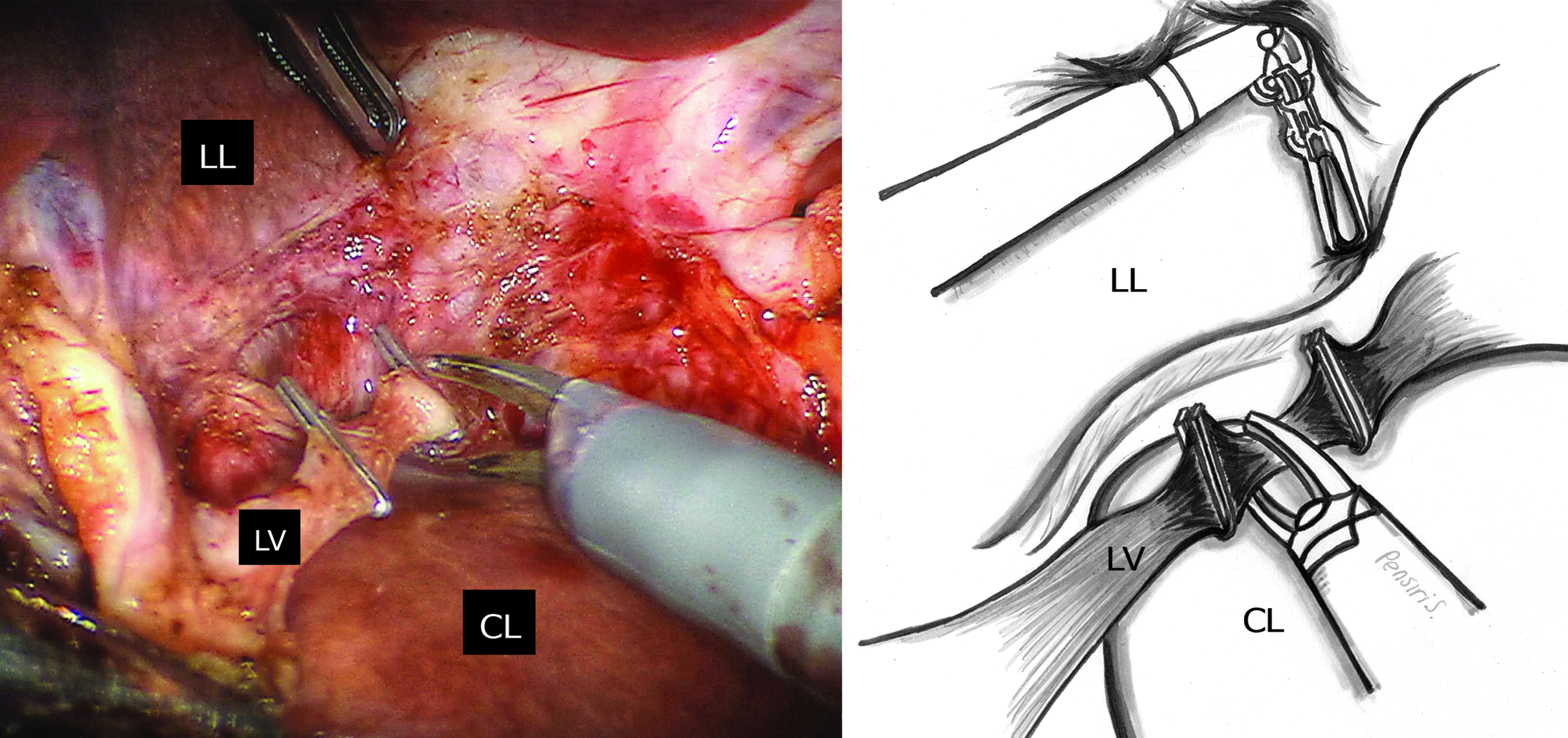
Detachment of LV from liver before clipping and transecting LV close to LHV. CL, caudate lobe; LHV, left hepatic vein; LL, left lobe of liver.
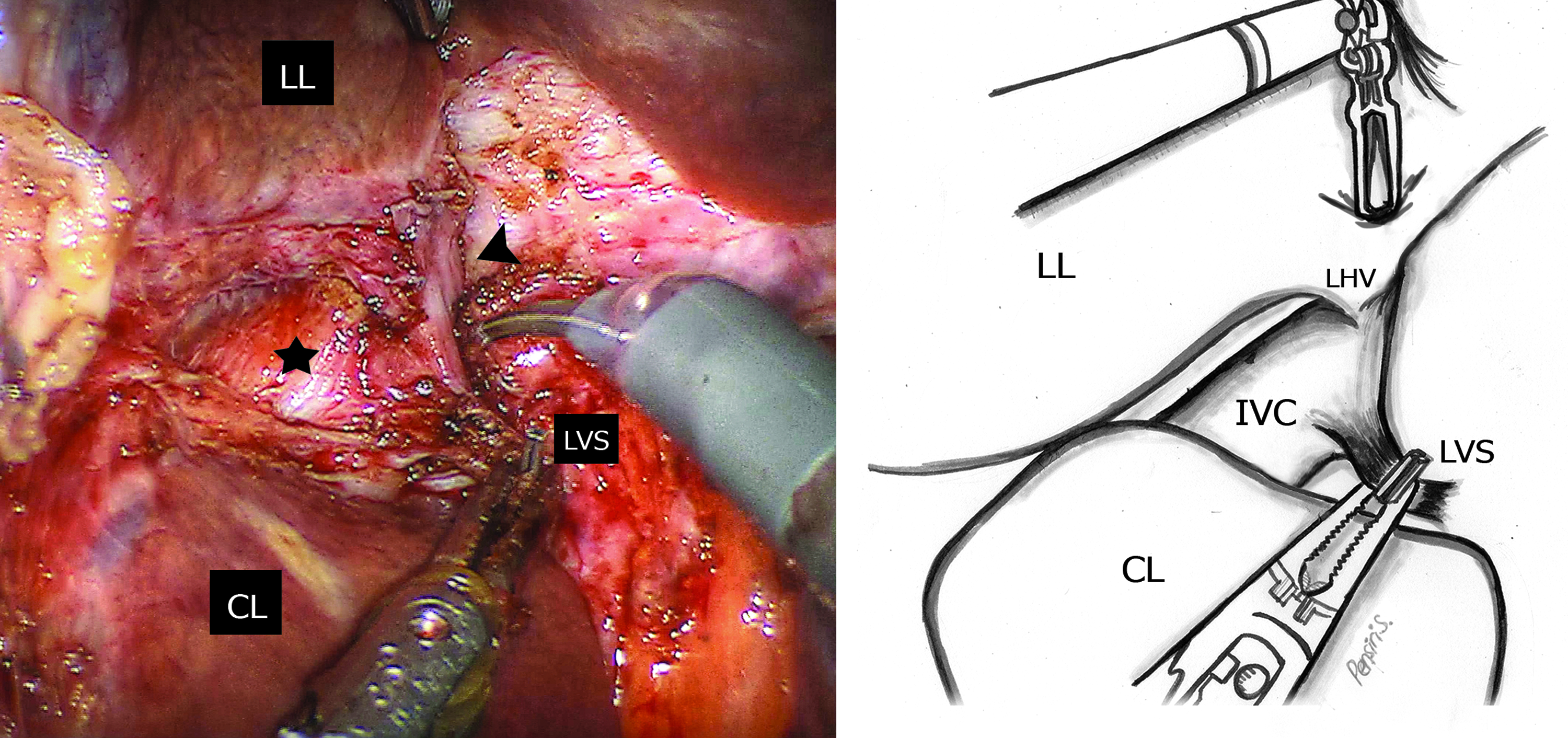
The space between LHV and IVC was opened to facilitate dissection of LHV by retracting LV stump to the left inferior direction. Arrow head, left hepatic vein; Asterisk, inferior vena cava; IVC, inferior vena cava; LL, left lobe of liver; LVS, ligamentum venosum stump.
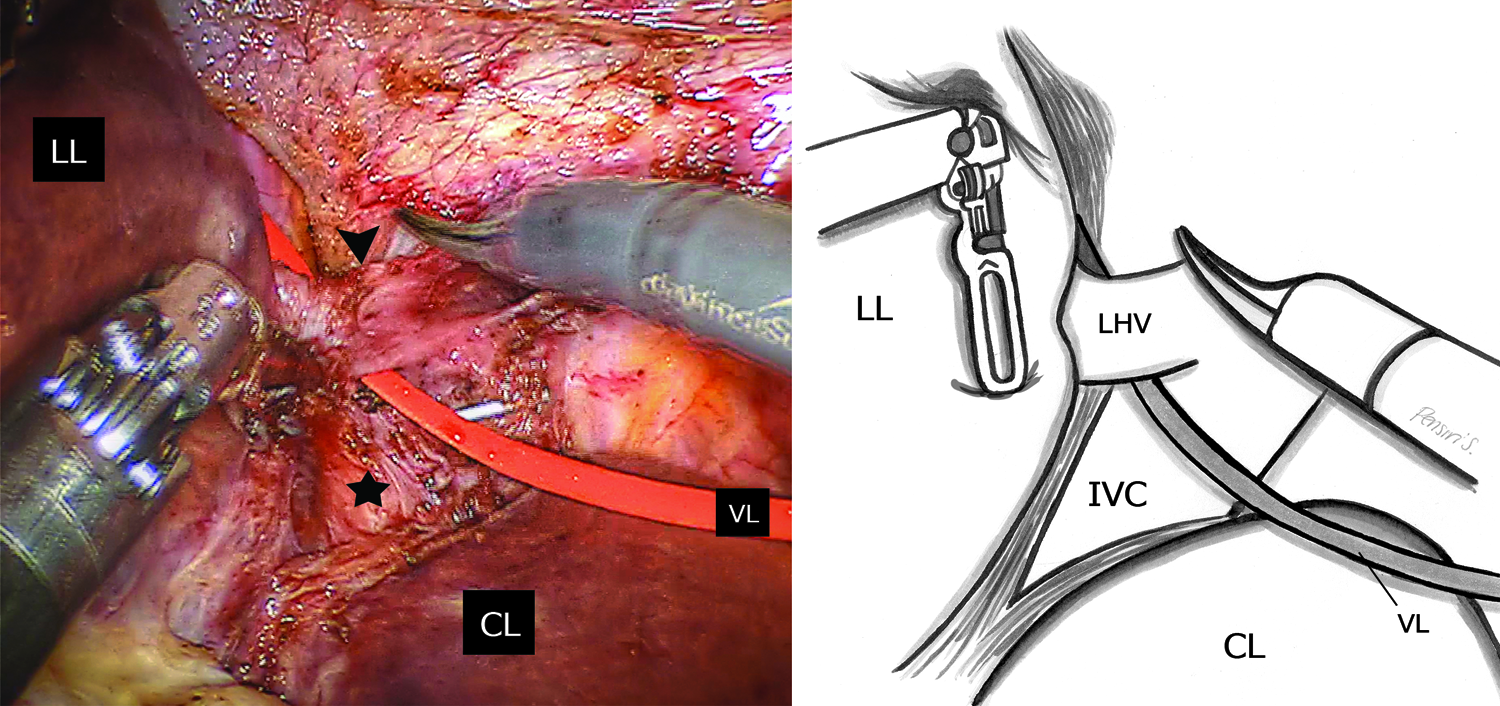
Inserting the tape through LHV. Arrow head, left hepatic vein; Asterisk, inferior vena cava; CL, caudate lobe; LL, left lobe of liver; VL, vessel loop.
Outcomes and results
From 2013 to 2015, 11 patients who underwent robotic LH and robotic LLS were reviewed. There were five cases of LH and six cases of LLS. LHV was successfully encircled by using this technique in seven cases, but encircling of LHV was not performed in the group of four cases. For the group of patients with LHV being encircled, the mean operative time was 244 minutes, the mean estimated blood loss was 300 mL, and the mean length of hospital stay was 4.8 days. Neither injury to LHV, MHV, and IVC, nor complications related to the liver were found.
Discussion and Conclusion
A vascular exclusion technique was used to diminish intraoperative blood loss. Extrahepatic inflow occlusion and hepatic vein occlusion known as selective hepatic vascular exclusion (SHVE) can provide bloodless field and be safer when compared with total hepatic vascular exclusion (THVE) because SHVE can avoid the hemodynamic drawbacks of THVE. 7 Not only providing bloodless field, but SHVE can also prevent venous air embolism from hepatic vein injury during parenchymal transection. 1 Moreover, the advantage of isolating and taping the LHV is useful to prepare for left lobe splitting living donor transplantation. 8 Right hepatic vein is easily dissected and encircled extrahepatically after the mobilization of the right lobe from IVC. 9 Conversely, LHV extrahepatic isolation is challenging because in 70%–96% of cases, the middle and LHVs formed a CT causing the short length of LHV.2–4 Normally, the extrahepatic portion of the LHV is not long, between 4 and 13 mm long depending on the presence or absence of a CT, 2 and selective extrahepatic clamping of the LHV is possible when the extrahepatic portion was at 10 mm long. 4 LHV controlled by blind clamping or blind ligating suturing is not recommended because the MHV may be damaged and be the cause of major bleeding. Majno et al. reported that the technique using LV approach to control LHV in open surgery could increase the success rate. 6 Therefore, we looked back on embryology and anatomy of LV (Arantius' ligament), a fibrous cord which is obliterated in 96% of the cases. Originating from ductus venous during the embryologic development (Fig. 6), it runs from left portal vein (LPV) and terminates in the CT for 61% and in the LHV for 39%.4,10 It can be used as a bridge to LHV by dividing LV and dissecting cephalad or a bridge to LPV by dissecting caudad. 11 LV, not only serving as a bridge to LHV and LPV, but also by retracting the cephalad stump to left inferior direction that counteracts with left lateral section of the liver, also provides the increasing angle between the plane of the IVC and CT or LHV. This allows creating more space for dissecting to posterior part of LHV, which is a key for success in encircling LHV safely. In one case, we could not identify LV intraoperatively corresponding with the previous cadaveric studies, reporting 2.4% had coronally flat and thin LV that was too difficult to identify. 10 In cirrhotic liver, this approach is still beneficial, but the dissection around IVC and hepatic vein should be performed meticulously due to the thickening and stiffness of surrounding tissues and the hypertrophy of caudate lobe particularly in the patients who underwent chemoembolization.2,12 This technique provided a success rate of 96% to encircle LHV for open liver surgery 6 and 40% in laparoscopic surgery. 5 Although this technique increased the success rate to control LHV in open surgery, the success rate in laparoscopic surgery was low in spite of its better field of view. The rigidity of the instrument that caused limited degrees of freedom during dissecting resulted in lower success rate in laparoscopic surgery.
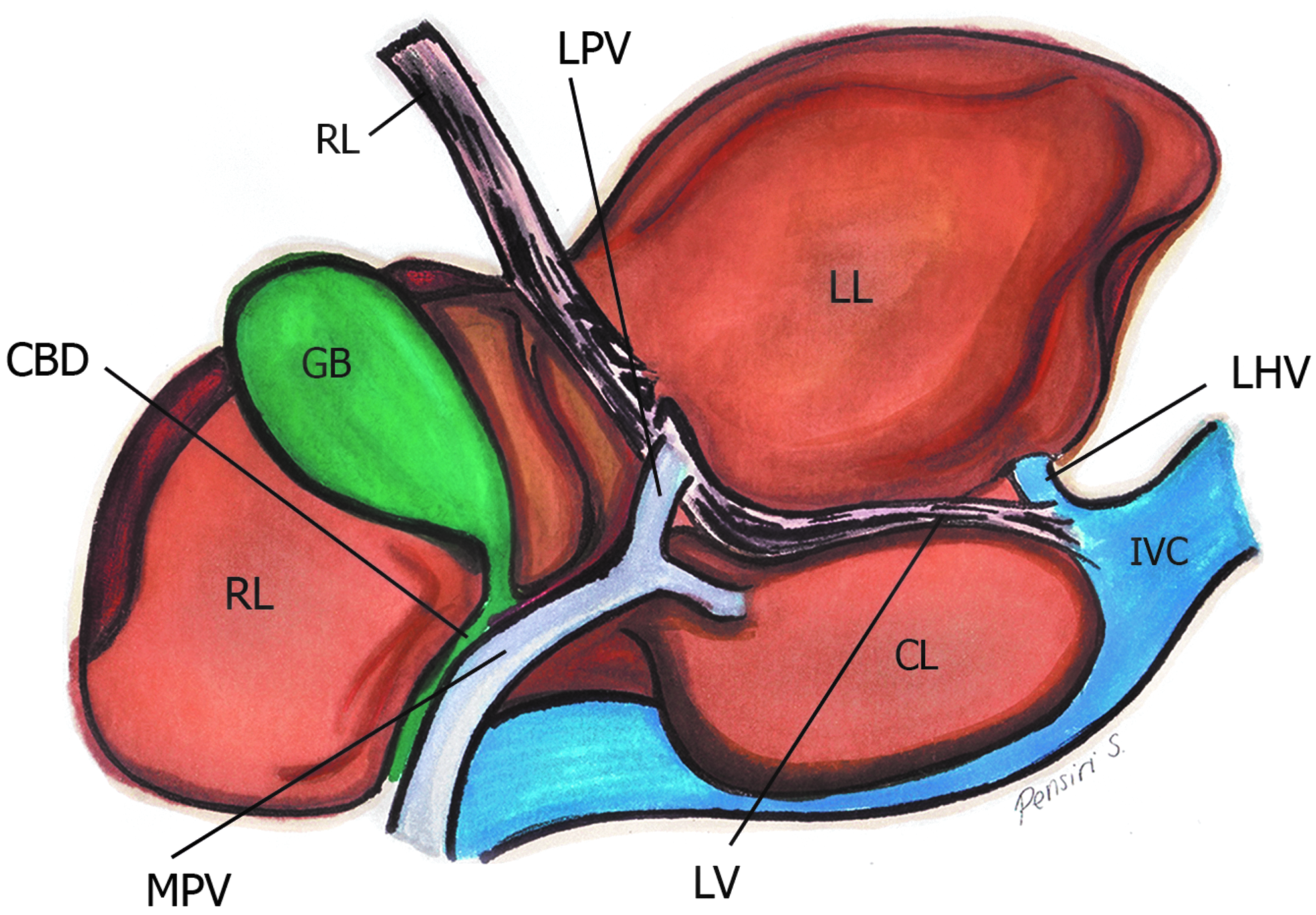
Schematic diagram of anatomical position of LV from robotic view point. CBD, common bile duct; CL, caudate lobe; GB, gallbladder; IVC, inferior vena cava; LHV, left hepatic vein; LL, left lobe of liver; LPV, left portal vein; LV, ligamentum venosum; MPV, main portal vein; RL, right lobe of liver; RL, round ligament.
From our robotic surgery experience, LHV was routinely controlled by the technique mentioned in robotic LH and LLS. It took 15–25 minutes after completing liver mobilization. Compared to the laparoscopic approach, the robotic surgical system allows for safer dissection and control of the hepatic vein because of its dexterity-enhanced endowrist, three-dimensional magnified imaging, tremor filtering, and motion scaling technology.13,14 The success rate from our experience was 60%. We were not successful in dissecting LV or encircling LHV in four cases. Of these, 3 patients had tumors compressing on LV and one with hypertrophic left lateral segment from cirrhosis obscuring the LV. Therefore, when any of the above conditions is encountered, we strongly recommend against using this technique.
Footnotes
Disclosure Statement
No competing financial interests exist.