
Abstract
Abstract
Laparoscopic donor nephrectomy has been broadly recognized as the gold standard for kidney procurement used in kidney transplantation where it is not uncommon for donors to experience discomfort and aesthetic dissatisfaction over larger incision site. Natural orifice transluminal endoscopic surgery is a surgical approach that allows scarless intraabdominal operations through natural orifices, such as the vagina. In this case report, we describe the first case of transvaginal retrieval of donor's kidney at the National University Hospital, Singapore. A 51-year-old Malay lady with no significant medical history volunteered to a living-related kidney donor. Perioperative antibiotics were administered. A 12 mm Excel port was placed over the left iliac fossa with camera insertion. Two additional ports were inserted over the left rectus sheath edge and left costal margin under direct vision. An additional 5 mm port at the left loin was placed for lateral retraction. A vaginal probe was then inserted to facilitate posterior colpotomy and transection of the left uterosacral ligament. Pneumoperitoneum was subsequently maintained with a LiNA McCartney® Tube. A 15 mm Endocatch® bag was inserted for retrieval of the kidney. The left kidney was placed in the Endocatch bag after transection of the hilar vessels where the kidney was retrieved vaginally with ease. Colpotomy was closed vaginally using Vicryl-0 continuous suture. Total blood loss was noted as 50 mL with warm ischemia time being 7 minutes and the entire retrieval taking totally 20 minutes. Postoperative recovery was uneventful and the donor was discharged stable 3 days postoperation. The transplanted kidney retained normal graft function. Colpotomy retrieval for donor nephrectomy presents an innovative method for specimen retrieval with minimal disruption of donor anatomy. Doing away with laparotomy for kidney retrieval has indeed shown a reduction in recovery time, reduced postoperative pain, and better cosmetic outcome.
Introduction
L
Natural orifice transluminal endoscopic surgery (NOTES) is a surgical approach that allows scarless intraabdominal operations through natural orifices, such as the vagina. Not only does it provide better cosmetic results, but numerous studies have also shown that the use of naturally occurring orifice has resulted in significantly less pain in the early postoperative period, leading to significantly shorter hospital stay.1,2
Bulian DR et al. into the long-term effects of NOTES reports no significant difference in postoperative sexual function, menorrhea, or vaginal discharge. 3
In this case report, we describe the first case of transvaginal retrieval of donor's kidney within Singapore, performed in our hospital.
Case Report
A 51-year-old Malay lady (Parity = 5) of body mass index 24.2 with no significant medical history volunteered to a living related kidney donor for her 25-year-old son. The donor was assessed as per standard pretransplant workup and deemed a suitable candidate for kidney donation.
The donor had no previous abdominal surgery and her five previous pregnancies were delivered vaginally. Cardiac assessment placed the patient under low perioperative cardiac risk with left ventricular ejection fracture (LVEF) at 55% under stress testing. Ultrasound breast and mammogram showed focal asymmetry with no signs of malignancy. Computed tomography angiography of renal arteries and kidneys showed perfusion of both kidneys through single arteries and veins with early take off of an upper pole branch on the left main renal artery. Dimercaptosuccinic acid (DMSA) scans show left kidney contributing to 47% of total kidney function with the remaining 53% attributed to the right kidney.
The donor was tested negative for HIV, diabetes, Hep-B, Hep-C, and cytomegalovirus (CMV). Full blood count (FBC), renal panel, and liver functions were also all normal. Twenty-four hours urine clearance was at 110 mL/min and 24 hours protein clearance was at 0.18 g/day. Electrocardiogram, chest X-ray, and Pap smears were also negative/normal. Psychiatric assessment deemed the patient fit to give informed consent.
The patient was reviewed a week before the surgery. Transvaginal retrieval of donor kidney was explained to the patient during the consultation. Speculum and vaginal examination was performed to ascertain the adequacy of the pelvic space. Vaginal douching was done and a week course of flagystatin® pessary was prescribed for the patient.
Operative Summary
The patient was placed under general anesthesia. A 14F indwelling catheter was inserted, cleaned, and draped in oblique position with both legs supported in a closed lithotomy position with all pressure points carefully padded and secured. Perioperative IV Rocephine and Flagyl were administered. Pneumoperitoneum was created using Veress needle. A 12 mm Excel port was placed over the left iliac fossa with camera insertion. Two additional ports (12 and 5 mm) were inserted over the left rectus sheath edge and left costal margin under direct vision. An additional 5 mm port at the left loin was placed for lateral retraction. Left ureter and gonadal packet were isolated and retracted laterally. Left renal artery and vein were defined and carefully dissected. Left adrenal and lumbar vein branches of the renal vein were dissected, ligated, and divided with Ligasure® Maryland. A single renal artery was noted with early upper pole branching to capsular vessels. Upper pole branch was noted to be 1 mm. A large gonadal and adrenal veins with separate inferior phrenic vein were noted.
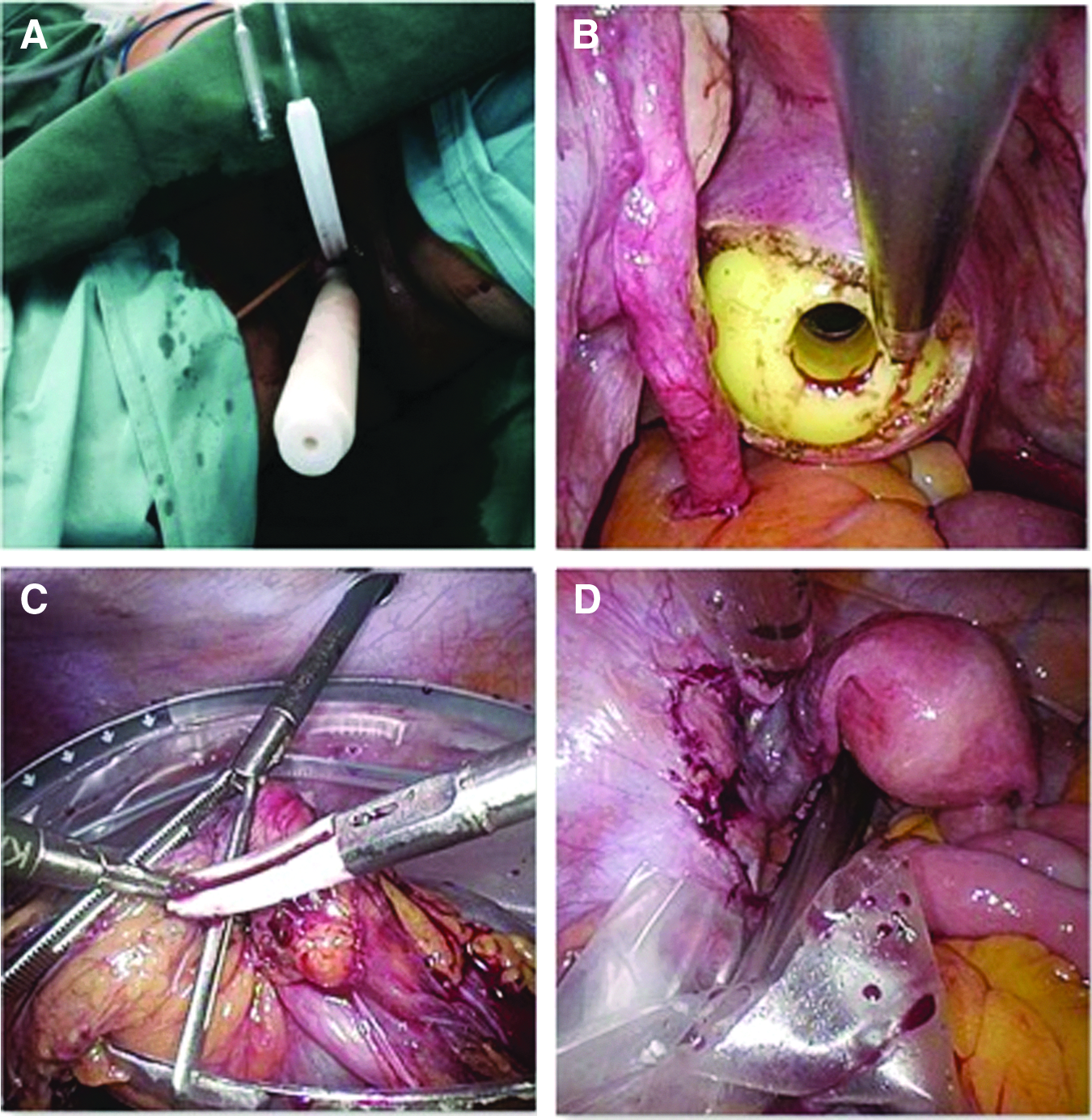
At this point, during the surgery, gynecological minimally invasive surgical assistance was sought. Vagina was douched thoroughly with iodine and chlorhexidine. Cervix was dilated to Hegar #8, Zinnati Uterine Manipulator Injector (ZUMI) was inserted (Fig. 1). The sigmoid colon was released laparocopically from the left pelvic side wall. A vaginal probe was then inserted to facilitate posterior colpotomy and transection of the left uterosacral ligament. Pneumoperitoneum was subsequently maintained with a LiNA McCartney® Tube. A 15 mm Endocatch® bag was inserted for retrieval of the kidney. The left kidney was placed in the Endocatch bag after transection of the hilar vessels by our urology colleagues. The Endocatch bag was closed and the kidney was retrieved vaginally with ease. Colpotomy was closed vaginally using Vicryl-0 continuous suture.
Post-Operation
The patient was transferred to a surgical high-dependency unit postoperatively. Postoperative VAS pain score 3/10 was managed with 8 hourly oral tramadol 50 mg and 6 hourly oral paracetamol 1 mg. TED™ stockings and Flowtrons® were used for DVT prophylaxis. IV Rocephine 1g 12 hourly was given as postoperative antibiotic cover for 3 days. Postoperative rehabilitation commenced with incentive spirometry and chest physiotherapy. IV dextrose 5% in sodium chloride 0.9% was given as fluid maintenance. Postoperative recovery was uneventful. The donor was discharged stable 3 days postoperation.
However, the patient was readmitted again a week after the surgery for subacute intestinal obstruction, likely secondary to postoperative inflammation. Fortunately, the obstruction resolved with conservative treatment. She recovered completely after this episode. Figure 2 shows the minimal abdominal scars 1 week after surgery. The outcome of the transplanted kidney retained normal graft function and her son recovered well.

View of donor's scars postnephrectomy at week 1.
Total blood loss noted: 50 mL
Gynecological surgery component: 20 minutes
Retrieval time: 2 minutes
Warm ischemic time: 7 minutes
Ephedrine required intraoperatively: yes
Discussion
NOTES presents an innovative method for organ and specimen retrieval without disrupting normal donor anatomy, eliminating any possible surgical implications. This helps to improve postoperative recovery time as well as increase overall patient satisfaction. In our case, wound dressings were completely removed at postoperative day 3 and she was discharged home with only oral analgesia. She was able to reintegrate back to her preoperative lifestyle quickly, not affecting her activities of daily living.
Bulian DR et al. compared 50 cases of NOTES transvaginal/transumbilical cholecystectomy (TVC) to 50 cases of traditional laparoscopic cholecystectomy. This study reported no significant difference between the conventional laparoscopic approach and NOTES in postoperative sexual function, change in menorrhea, vaginal discharge, or postoperative abdominal pain. Patients operated through NOTES were able to resume everyday life significantly earlier, experienced greater aesthetic and overall patient satisfaction. A survey revealed that significant proportion of patients who underwent TVC would recommend the applied surgical technique to friends and family. 3
The use of NOTES in other centers has been well documented with good results. In 2009, Alcaraz A et al. published a retrospective study, in which transvaginal NOTES-assisted laparoscopic nephrectomy was performed in 14 female patients for renal cancer or renal atrophy in the hospital clinic of Barcelona, Spain. None of these patients required blood transfusion (n = 0). Minimal analgesia was used with the mean hospital stay reported to be only 4 days. They experienced a single case of complicated bowel injury. This study demonstrates NOTES to be a feasible and safe alternative for specimen retrieval.4,5
Although laparoscopic surgery and NOTES do have advantages, they are not without disadvantages. In 2009, Sotelo and colleagues reported four cases of transvaginal NOTES procedures in two different institutions. Three of which had to be converted to laparotomy due to rectal injury during vaginal entry with failure to progress and gradual bleeding during dissection after transvaginal hilar control, respectively. Although the fourth case was successful, this shows the complexity, difficulty, and scope for injury in the NOTES approach. 5 Greater number of cases would be needed to further assess the safety, reliability, and reproducibility of NOTES in our center.
Experienced mentoring and further refinement of technique will be essential to ensure NOTES transitions into a safe, reliable, and reproducible method of specimen retrieval.
We believe that transvaginal retrieval of the donor's kidney is safe and feasible, it facilitates faster recovery and improved patient satisfaction. Nevertheless, the potential risk of vaginal infection control and damage to the kidney during the retrieval warrants due attention. With that in mind, we employed preoperative intravaginal metronidazole pessaries along with vaginal douching. In addition, the donor's kidneys were placed in a laparoscopic bag during retrieval to minimize the risk of infection. For future surgeries, we propose the transection of the left uterosacral ligament to widen the colpotomy to facilitate safe retrieval and to eliminate any risk of damage to the left ureter. For this case, we are pleased to report that the transplanted kidney retained normal graft function.
Conclusion
NOTES combined with laparoscopic approaches represents a breakthrough, allowing for large sized specimen handling and retrieval without open surgery. The avoidance of a laparotomy wound removes a whole host of complications from the postoperative recovery phase, leading to reduced recovery times. Coupled with better cosmetic outcomes, the NOTES approach will certainly lead to improved overall patient satisfaction. With this novel surgical approach that minimizes the adverse effects of surgery, we hope to encourage more potential kidney donors.
In conclusion, laparoscopic donor nephrectomy with transvaginal retrieval of donor's kidney represents a safe, simple, and reproducible method of organ retrieval for future kidney donors.
Footnotes
Disclosure Statement
No competing financial interests exist.