
Abstract
Abstract
Background:
Transoral endoscopic approach is the natural orifice surgery applied in thyroidectomy to achieve an excellent cosmetic result. Recurrent laryngeal nerve (RLN) injury is the most common complication and little advancement was achieved in the previous clinical studies of transoral thyroid surgery. Herein, we introduced the method of intraoperative neuromonitoring (IONM) for transoral endoscopic thyroid surgery.
Materials and Methods:
Patients with thyroid carcinoma received transoral endoscopic thyroid surgery through vestibular approach (TOETVA) for thyroidectomy and central node dissection (CND). IONM was implemented to identify whether the RLN benefited from oral tracheal intubation. The laryngeal electromyography (EMG) response, operation time, number of CND, drainage volume, hospital duration, surgical complications, and cosmetic results were evaluated.
Results:
From August to October 2015, 10 cases were performed with TOETVA and IONM. All EMG responses were recorded intraoperatively, and no case experienced transient or permanent RLN palsy. The operation time ranged from 130 to 215 minutes in ipsilateral lobectomy with CND, whereas bilateral lobectomy with ipsilateral CND lasted 345 minutes. The number of CNDs ranged from three to eight. The average time of drainage extubation and discharge was 4 days (3–5 days) postoperatively. All patients were satisfied with the cosmetic results, and no infection was observed at lip wound or in the anterior neck region.
Conclusion:
IONM system implemented in transoral thyroid surgery was feasible and serviceable in preventing RLN injury. The method of TOETVA shows promise for thyroidectomy with CND due its ideal cosmetic results.
Introduction
B
To be minimally invasive, a surgery should be considered safe, should minimize tissue dissection, and avoid scarring. 4 However, the existing endoscopic approaches for thyroidectomy have been questioned and criticized as not being truly minimally invasive. 5 Both the bilateral axillo-breast and gasless axillary approaches require more flap dissection, extensive tissue dissection in the chest and neck, and still leave hidden scars. Many surgeons believe these existing approaches are more invasive than conventional open thyroid surgery, and thus research is recommended to explore innovative approaches in devising less invasive surgeries.
Transoral approach for thyroidectomy has been reported to overcome the limitations of previous methods because it embodies minimally invasive principles.6,7 It is considered a truly natural orifice transluminal endoscopic surgery (NOTES) and has advantages, such as close access to thyroid gland, limited tissue dissection, and no cutaneous scar or deformity. 8 However, as the vision of “up to down” is uncommon compared with conventional open or endoscopic techniques, experienced laparoscopic skills are needed to clearly represent the anatomic structure to avoid surgical complications. Therefore, it is still controversial because the transoral approach may enhance the incidence of complications, such as hematoma, pain, swallowing problems, and recurrent laryngeal nerve (RLN) palsy. 9 In addition, intraoperative neuromonitoring (IONM), which is commonly implemented in conventional open thyroid surgery and other approaches of endoscopic surgeries to explore and identify RLN, cannot be used in a transoral approach thyroid surgery due to implementing general anesthesia with nasotracheal intubation.
The aim of this study is to introduce IONM for transoral endoscopic thyroid surgery with oral tracheal intubation, evaluate the advantages and disadvantages, and discuss its feasibility compared with other conventional procedures.
Materials and Methods
From August to October 2015, 10 patients received transoral endoscopic thyroid surgery through vestibular approach (TOETVA) and IONM. These techniques were successfully implemented in our study. All operations were performed by one experienced thyroid surgeon. Patients who chose TOETVA had been given detailed introduction and signed informed consents. This study was approved by the Ethics Committee of the Second Affiliated Hospital, Zhejiang University College of Medicine, a teaching tertiary care unit of a public hospital, and has also been approved by the Joint Commission on Accreditation of Healthcare Organizations.
Preoperative preparation
Each patient was recommended to wash his or her mouth with concentrated tinidazole gargles thrice per day for more than 3 days. Preoperative evaluation was implemented carefully, and the surgical indication of our single center's experience include the following: (1) thyroid papillary carcinoma without any evidence of metastasis, (2) benign tumor, such as single or multinodular goiter, (3) follicular neoplasm, and (4) Grave's disease, which is resistant to drug therapy. All patients receiving transoral thyroid surgery needed to confirm the following two criteria: (1) the patient is keen to pursue optimal cosmetic result and (2) the diameter of thyroid gland and mass should not be larger than 8 and 2 cm, respectively.
Operative procedures
Compared with conventional TOETVA procedures, we chose oral tracheal intubation and fastened the tube to angulus oris under the state of general anesthesia (Fig. 1). The patient was in a supine position with neck extension, using a sand bag placed under the shoulder blades. Antibiotics were administered by intravenous drip preoperatively as prophylactic anti-infective therapy. The oral cavity was rinsed thoroughly, thrice with povidone–iodine (PVP-I), and several absorbent cotton pieces were applied to prevent dental injury. A 30 mL solution of 225 mg ropivacaine was diluted with 70 mL epinephrine solution (1:500,000), as an “expanded fluid.” Approximately 50 mL of expanded fluid was administered subcutaneously into the subplatysmal space until the anterior neck; the initial tunnel was performed by the usage of a traditional dissection stick (as the instruments for laparoscopic surgery).

Oral tracheal intubation was performed, and the tube was fastened to angulus oris under general anesthesia.
A 10-mm incision was made at the center of oral vestibule; each edge was sutured to prevent wound tear (Fig. 2A). With the assistance of a suspension system, including skin puncture needle, steel jacket, fixed device, and suspension chain, a subsequent space was created, passing the mandibular area to the anterior neck along an almost straight direction using a visualization stick (Fig. 2B). A threaded 10-mm trocar was inserted for 30° laparoscopy, and the CO2 insufflation pressure was controlled at 6 mmHg. Then, bilateral 5-mm incisions (prepare for 5-mm laparoscopic trocars) were localized at the junction between canine and premolar and extended into the alveolar mucosa with vascular forceps. Both sides were pointing down to the anterior neck until reaching the sternocleidomastoid, and the subcutaneous gap was expanded with electrical hook and harmonic scalpel under direct laparoscopic vision. The operating space was created as in conventional TOETVA, namely larynx was the upper border, suprasternal notch was the symbol of lower border, and sternocleidomastoid muscle was the lateral border.
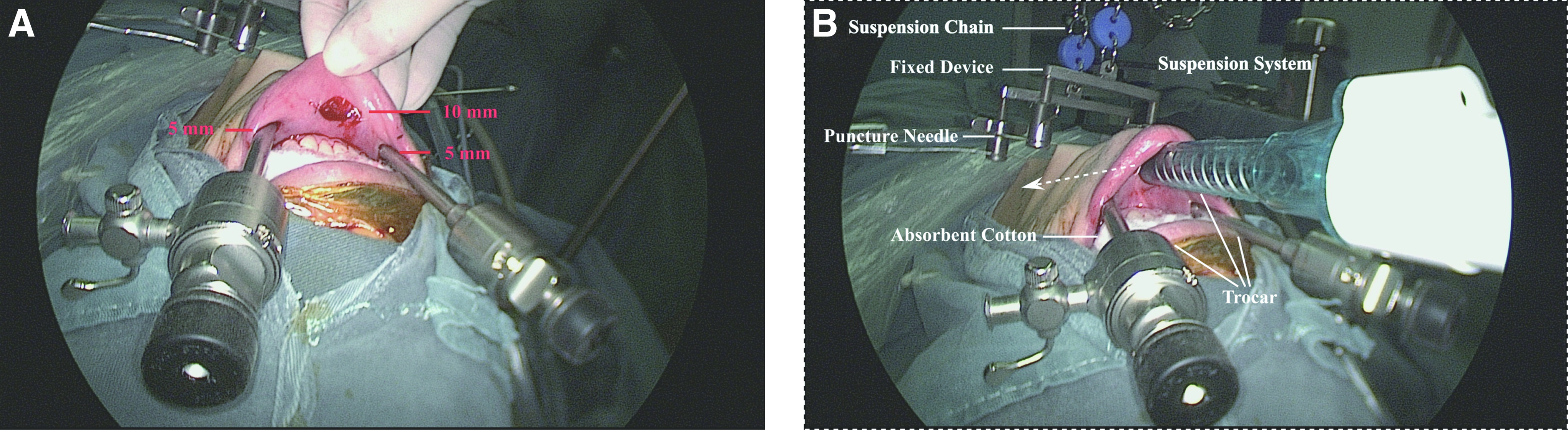
View during the technique of transoral endoscopic thyroid surgery through vestibular approach.
Along with linea alba cervicalis, the strap muscles were divided with an electric hook and retracted laterally by bilateral endoscopic retractors. The usage of endoscopic retractors had been introduced in our previous article. 10 Thyroid isthmus was divided with harmonic scalpel and then lifted medially using grasp forceps (access to the operative field through the 5-mm trocar). With the assistance of endoscopic retractors retracting ipsilateral strap muscles laterally and grasp forceps drawing the upper pole of thyroid medially, the superior thyroid vessels were identified and coagulated individually, close to the thyroid capsule using a harmonic scalpel. During this procedure, the superior parathyroid gland and its vascular pedicle were identified and preserved. Cooperating with retracting ipsilateral strap muscles laterally by assistants and lifting thyroid tissue up with grasp forceps, middle thyroid veins were identified and ligated close to the thyroid membrane using a harmonic scalpel.
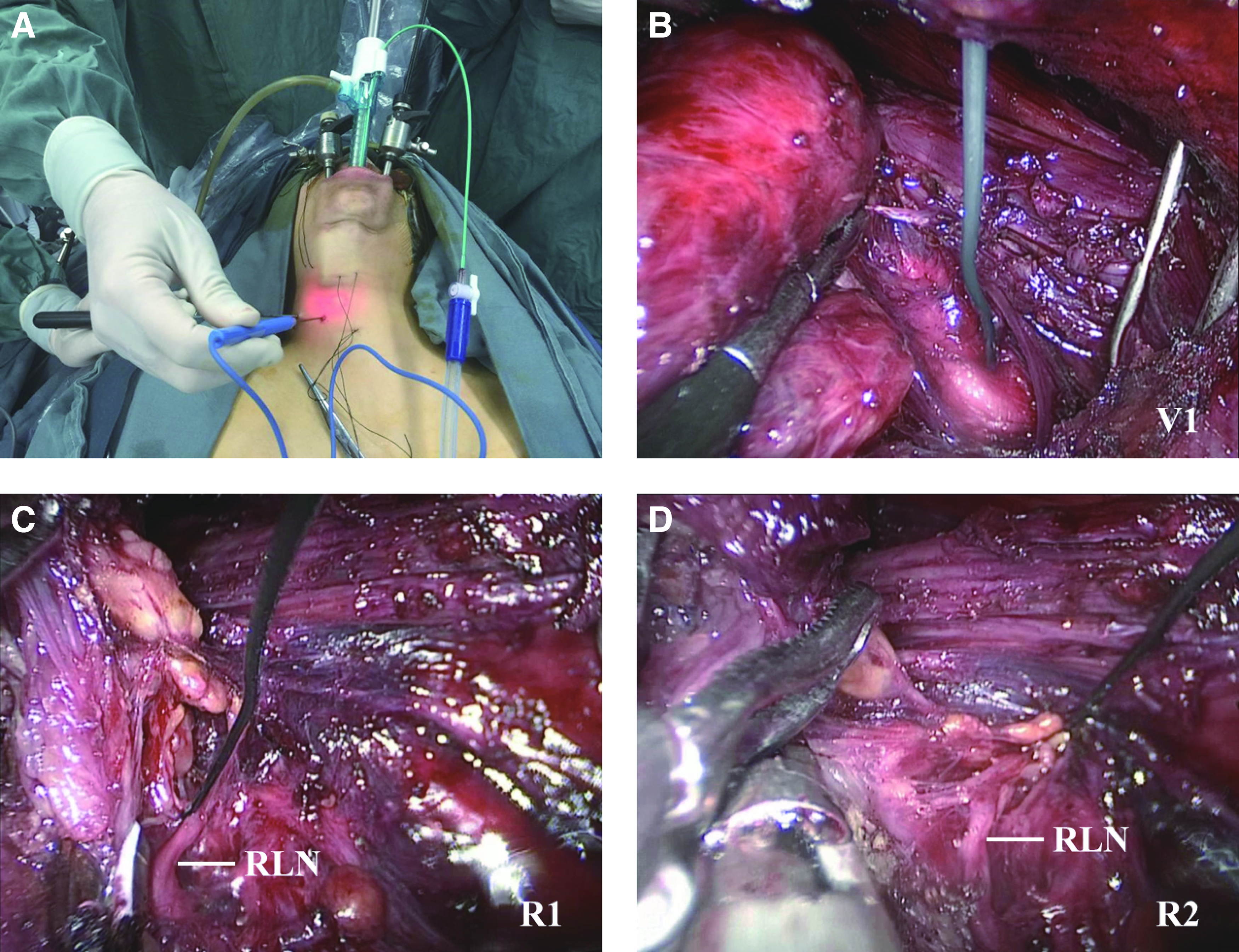
In addition, IONM was performed at a “suspicious area” before performing any surgical procedure to explore the growing direction of RLN, identify RLN reliably, and verify the functional integrity of RLN (Fig. 3A). With the guidance of IONM using stimulation level of 3 mA, the localization of RLN was evaluated, and gentle blunt dissection was performed to explore RLN at its entry point and traced inferiorly using IONM forceps (Fig. 3B). RLN was identified relying on laryngeal electromyography (EMG) responses with the stimulation level of 1 mA (Fig. 3C). A standardized procedure was performed after the nerve monitoring probe punctured the skin over the operation area in the neck (Fig. 4A). The vagus nerve was routinely tested with a current of 3 mA to ensure that the monitoring system be normal (Fig. 4B). The EMG signal of R1 was recorded by a current of 1 mA after exposure of the RLN (Fig. 4C). After the whole operation, signals of RLN and vagus nerve were obtained by probe stimulator as R2 (Fig. 4D) and V2, respectively. The different IONM stimulators were chosen according to the operative purpose; if the surgeon needs to evaluate the location of RLN, a high level (3 mA or more) would be appropriate, while if the purpose was to identify RLN or confirm its integrity, a low level (1 mA) would be better.
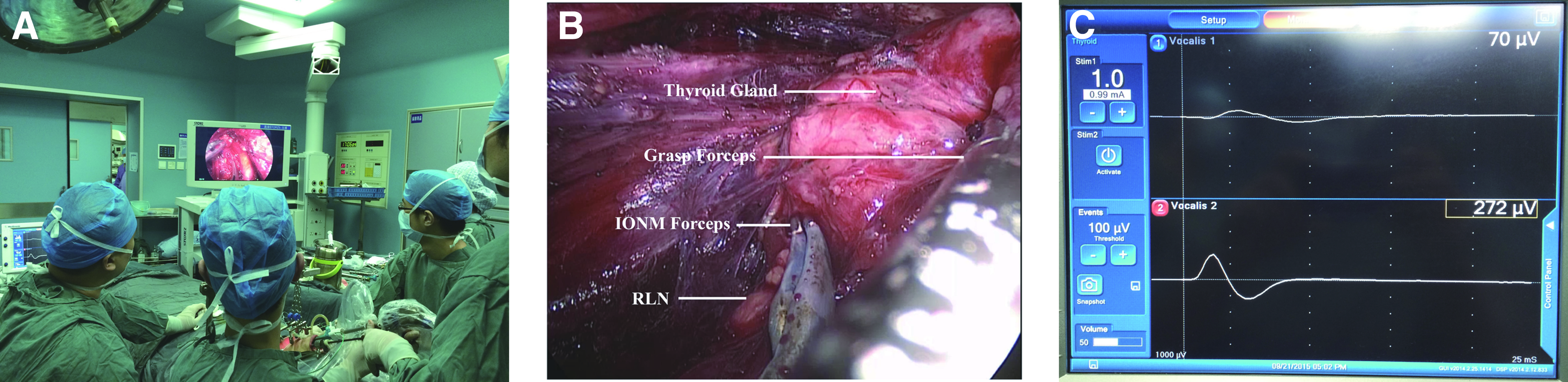
Intraoperative neuromonitoring (IONM) was implemented for transoral endoscopic thyroid surgery.
Shows the position of patient and the endoscopic view of the nerve stimulator.
Thyroid dissection was implemented by tracing the growing direction of RLN carefully with a harmonic scalpel and vascular forceps (Fig. 5A). During this procedure, the functional scalpel should be kept away from RLN all the time, preventing thermal damage to the nerves (Fig. 5B). The aim of preventing RLN injury at its entry point can be easily achieved due to the clear vision of “up to down.” After the procedure of dissecting the thyroid capsule away from RLN with vascular or IONM forceps, the Berry's ligament was identified and divided using a harmonic scalpel. During this procedure, the harmonic scalpel can be rotated at an angle to obtain a better operative vision, and the functional scalpel should be always kept away from nerves (Fig. 5C). In addition, the inferior parathyroid gland with its vascular pedicle was also identified and preserved carefully. Then after the thyroid lobe was lifted medially with a grasp forceps, the lower pole was identified and divided from perithyroidal tissues. After the procedure, strap muscles were retracted by a repositioned endoscopic retractor, and lymph nodes at the VI region were dissected thoroughly from thymic tissues until the suprasternal notch.

View during the procedure of identifying and preserving RLN at its entry point.
Postoperative procedures
The specimens were removed using an abstemious endobag through the 10-mm incision and sent for examination of frozen section and pathology. A 2-mm, no-scar formation, vacuum suction drain was inserted through the anterior neck region. The midline incision of the strap muscles was closed under endoscopic vision. Also, the oral vestibule surgical closing was implemented with collagen absorbable sutures. A chin–head bandage was applied to compress the mandible for 12 hours postoperatively. The mouth was washed with concentrated tinidazole gargles, and antibiotics were administered by intravenous drips for 3 days as prophylactic anti-infective therapy.
Results
Retrospective to October 2014, more than 50 patients have received transoral endoscopic thyroid surgery in our center. Between August and October 2015, IONM was implemented in 10 patients with papillary thyroid carcinoma (PTC), in whom a left-, right-, or bilateral lobectomy with a central node dissection (CND) was performed using the TOETVA technique. Intraoperatively, nerve monitoring was performed at “suspicious areas” before and after any surgical procedure, to estimate the growing direction of RLN, identify RLN reliably, and verify the functional integrity of RLN. The RLNs were clearly identified and preserved in all cases, and none of the patients experienced temporary or permanent vocal cord palsy. All patients were permitted water and soft diet intake beginning 6 hours postoperatively. Prophylactic antibiotics were administered in each patient preoperatively by intravascular injection and continued until 3 days postoperatively. Systemic infections did not occur in any patient, and no local infections were observed at the wound incision site or within the anterior neck region.
The mass sizes ranged from 0.5 to 1.3 cm; only case 8 had the characteristic of mulifocality. All patients received an examination of fine needle aspiration, and the cytologic results were follicular neoplasm, suspicious or malignant. Finally, all 10 cases were confirmed as PTC by pathologic examination, and 2/10 (20.0%) cases were accompanied with Hashimoto's thyroiditis.
Except for case 8, in whom bilateral lobectomy with right CND was performed and lasted 345 minutes, all other cases were implemented unilateral lobectomy plus isthmectomy with ipsilateral CND, and the operation time ranged from 130 to 215 minutes (Table 1). The lymph node yield in ipsilateral central region ranged from three to eight. Upper and lower parathyroid glands were identified and preserved carefully; only 1/10 (10.0%) patient (case 4) experienced temporary hypoparathyroidism and required vitamin D supplementation due to superior parathyroid injury. No other complications, such as hematomas, permanent hypocalcemia, mental nerve palsy, superior laryngeal nerve injury, subcutaneous emphysema, or tracheal injury, were found postoperatively.
BMI, body mass index; CND, central node dissection; F, female; FN, follicular neoplasm; I, isthmectomy; M, male; N, number; LL, left lobectomy; PTC, papillary thyroid carcinoma; RL, right lobectomy; SFN, suspicious for follicular neoplasm.
The surgical drain was removed in an average of 4 days (range 3–5 days), and 9/10 (90.0%) cases were discharged at the day of extubation. The average total drainage volume ranged from 98 to 190 mL, whereas the first day was 30–103 mL (Table 2). Although four patients complained of pain postoperatively, it was alleviated within 24 hours after the chin–head bandage was removed. Within the 1-month follow-up, the intraoral incisions were completely recovered (Fig. 6), and all patients were satisfied with the cosmetic results.

Cosmetic result of a patient 1 month postoperatively. The scars placed in the intraoral regions were nearly invisible.
Discussion
This is the first study reporting a clinical application of IONM in transoral endoscopic thyroid surgery. Since Witzel et al. 6 introduced transoral thyroidectomy in 2008, this method has been identified as a NOTES, and its feasibility has been demonstrated in animal, cadaveric, and clinical studies.5,7,11 Although several different approaches were invented during the development of transoral thyroid surgery, the method of TOETVA through three ports with or without assistant ports was believed to be an effective technique and had been demonstrated by a few clinical trials.5,11,12 However, this technique is still controversial and needs modification in preventing surgical complications, such as RLN injury. IONM, which was demonstrated to be effective and widely used in conventional open thyroid surgery, however, has never been performed in transoral surgery to identify RLN in the previous literature. In this study, we developed a vestibular approach for thyroidectomy with CND and successfully performed IONM to explore and identify RLN. Every EMG response was recorded, and no case experienced transient or permanent RLN palsy.
The major advantage of implementing IONM in transoral thyroid surgery is identifying RLN and confirming its integrity. Although visual identification of RLN is considered the gold standard in prevention of nerve injury, IONM is recommended to help in identifying nerves and preventing misidentification of any cord-like structure such as a nerve in high-risk patients during thyroid surgery. 13 In addition, RLN management through visualization alone does not afford surgeons with appropriate information about the functional status of visually intact nerves. 14 According to our institution's experience, although the method of transoral thyroid surgery is easy to obtain a satisfied operative view, it is probably at higher risk to explore and identify RLN in the vision of “up to down,” especially in the hands of low-volume surgeons. Previously, Nakajo et al. 11 reported that one of eight patients suffered permanent RLN palsy. More recently, transient RLN injury was also observed in 2 of 60 cases. 12 In this study, IONM was implemented in 10 patients with PTC who received thyroidectomy with CND using the method of TOETVA. No anomalous EMG response was recorded, and this result made surgeons more comfortable during the procedure, especially in dissection of RLN near the Berry's ligament. Therefore, IONM adjunct to routine visual identification can be safe and feasible in identifying and preserving RLN during the operation of TOETVA.
This study is also advantageous for good cosmetic results. One month postoperatively, all patients were followed up, and there were no external scars in the anterior neck. The scars placed in the intraoral regions were nearly invisible due to the high healing ability of the lip mucosa (Fig. 6). Furthermore, all patients were satisfied with the cosmetic results, and none of them complained of discomfort in the scar regions. As a result, TOETVA in this study corresponded to the concept of a truly NOTES, avoiding incisions on the body wall and probably being considered a better surgical technique compared with conventional open or endoscopic methods of thyroid surgery.
Another advantage of this study is an excellent visualization provided during the operation. A novel method was introduced that was combined with CO2 insufflation and mechanical lifting to create a working space and provide a good view during the procedure of CND. In addition, the pressure of CO2 insufflation was no more than 6 mmHg, avoiding postoperative emphysema. Obtaining a high-quality craniocaudal view, the procedure of complete CND was performed easily, and the dissection number of lymph nodes in 10 patients ranged from three to eight, which is equivalent to conventional open surgery. Therefore, with the help of CO2 insufflation and mechanical lifting, a good visualization for thyroidectomy and CND can be provided. In addition, the method of TOETVA is an adequate surgical procedure for thyroidectomy and complete endoscopic CND.
After several preclinical and clinical studies, transoral thyroid and parathyroid surgery are considered a promising technique because it combines minimal invasion and cosmetic results.4,5,12,15 In this novel study, we performed IONM in transoral thyroid surgeries, trying to decrease the high incidences of temporary or permanent RLN palsy, and the result was achieved satisfactorily. However, quite a number of limitations still remain and need to be overcome in developing this technique, such as mental nerve injury, hematoma, local streptococci infection, longer surgical time, and intraoperative bleeding where the method had to be converted to open surgery. 9
One of the remaining challenges is that lateral gingival–buccal port placement may introduce a risk of mental nerve injury. As mental foramen is commonly placed below and between the mandibular premolars, bilateral 5-mm incisions located between canine and premolar were made to avoid encountering the mental nerve in this study. No symptoms of mental nerve injury were observed, such as paresthesia or other sensory disorders between lower chin and lip. Therefore, the method developed in this study can be gradually applied to perform thyroidectomy and complete CND, which also achieves the principle of avoiding mental nerve injury through transoral approach.
The incidence of infection within the anterior neck or lip wounds may be increased while implementing the method of TOETVA because the conventional aseptic wound is contaminated due to spread oral microflora. In this study, combined procedures, including concentrated tinidazole gargles preoperatively, PVP-I rinse operatively, and prophylactic anti-infective therapy for 3 days postoperatively were performed, and no infections were observed in these 10 patients. At surgical conclusion, a drain was inserted into the surgical field through the anterior neck and connected to a vacuum suction. The diameter of drain was designed to be no more than 2 mm so as to avoid introducing additional scars. As is shown in Table 2, the average time of drain extubation and discharge was 4 days (3–5 days) postoperatively, and the drainage volume ranged from 98 to 190 mL. In the end, no patients developed infections in the lip wounds or anterior neck. These results suggest that infection can be prevented after the operation of transoral thyroid surgery by administration of meticulous nursing, excellent operative performance, and prophylactic anti-infective therapy.
The method of TOETVA for thyroid surgery may be disadvantageous by its longer surgical time than conventional open thyroid surgery. In this series, the surgical duration time of ipsilateral lobectomy with CND ranged from 130 to 215 minutes, whereas bilateral lobectomy with ipsilateral CND lasted 345 minutes. This is not a short time for thyroid surgery. However, as the study by Anuwong et al. 12 reported, the average surgical time of hemithyroidectomy was 90 minutes, whereas bilateral thyroidectomy was 135.5 minutes using the method of TOETVA. Lee et al. 5 believed the learning curve should stabilize after 20 procedures. In this study, only 10 cases were included. Therefore, more transoral thyroid surgeries are required to calculate the average time and achieve a shorter operative duration.
The vital signs monitored intraoperatively were stable in each patient. Temporary hypoparathyroidism requiring calcium and vitamin D supplementation was observed in one of the 10 cases due to superior parathyroid injury. Although 4 of 10 patients felt pain in the mandible region in the first day postoperatively and the pain score was 2, this unpleasant perception can be relieved instantly. In addition, the method of TOETVA would also have faster wound healing than other conventional open or endoscopic surgery. As other clinical trials reported, no hematomas, vocal cord hoarse, subcutaneous emphysema, or superior laryngeal nerve injuries occurred in this clinical study.5,16
In conclusion, implementation of IONM for transoral thyroid surgery can be considered serviceable and feasible with the benefit of decreasing the incidence of RLN injury, especially in the hands of low-volume surgeons. The method of TOETVA shows promise for thyroidectomy with CND due its ideal cosmetic result.
Footnotes
Acknowledgment
The research was supported by National Science Foundation of Zhejiang Province (LY14H160033).
Disclosure Statement
No competing financial interest exists.