
Abstract
Abstract
Background:
Multiple factors can account for surgical complexity during laparoscopic partial nephrectomy (LPN); severe adhesion of perirenal fat (PRF) is a crucial one. Consequent renal decapsulation can deem renorrhaphy a very challenging task. We propose a novel technique (synthetic renal capsule tailoring [SYRCT]) to facilitate renorrhaphy in decapsulated kidneys and suggest early decapsulation as a safe option in cases with severe PRF.
Materials and Methods:
We retrospectively analyzed perioperative results of this novel technique performed in cases with severe PRF. All cases were classified as high grade in the Mayo Adhesive Probability (MAP) score.
Results:
A total of six cases were performed with the SYRCT technique. All patients were male with a mean age of 70 years (62–76 years) and mean body mass index of 30 kg/m2 (23.66–33.86). Of the six cases, five were T1a and 1 T1b. Mean tumor size was 2.83 cm (range 1.2–6 cm). Mean operative time was 121 minutes (range 74–150 minutes); mean warm ischemia time was 17.2 minutes (range 13–25 minutes). Mean operative bleeding was 128 mL (range 50–250 mL). Mean hospital stay was 2.3 days. There were no surgical complications greater or equal to Clavien II.
Conclusion:
Performing complete renal decapsulation with subcapsular dissection and SYRCT in cases with high MAP score and severe PRF is safe and reproducible. Using this novel technique, we were able to obtain perioperative results comparable to the ones we found in LPN with normal PRF.
Introduction
M
PRF can be very deceiving. Sometimes it can be very thin and easily manipulated and other times it can present itself as an actual fibrotic shell that surrounds the kidney, making dissection tedious, difficult, and dangerous. Considering this, Davidiuk et al. described the Mayo Adhesive Probability (MAP) score as a toll to predict the quality of PRF. MAP score takes into account two variables that can easily be obtained either on a magnetic resonance imaging (MRI) or computed tomography (CT) scan.
(a) Thickness of PRF (measured posteriorly on an axial cut at the high of the renal).
(b) Degree of striation (no striation: 0, light striation: 1, and severe striation: 2).
Recent work by Davidiuk et al. has linked high MAP score to PRF.4,5 However, only Kocher et al. found a direct correlation between MAP and malignant pathology. 6 Another study by Thiel et al. proposes a direct correlation between a high MAP score and disease-free survival, assigning PRF a new and very interesting role in renal-cell carcinoma. 7
PRF adhesion to renal capsule is not to be taken lightly. In some cases, finding a plane of dissection between both is virtually impossible forcing the surgeon to decapsulate the kidney to find the tumor and perform a subcapsular dissection. Decapsulation in itself is associated with concomitant bleeding and parenchyma weakening. A decapsulated kidney is very fragile and can prove to be very hard to suture. To this respect, tensile strength has been compared between normal and decapsulated human kidneys. 8 Decapsulated kidneys resist between 43% and 63% less than normal ones deeming renorrhaphy a very challenging task with the inherent risk of severe surgical bleeding.
Herein, we propose a novel technique to facilitate renorrhaphy in decapsulated kidneys and suggest early decapsulation as a safe option in cases with severe PRF.
Materials and Methods
We retrospectively analyzed perioperative results of this novel technique performed in cases with MAP score of 4–5. Age, sex, presentation, RENAL score, MAP score, surgical approach, warm ischemia time (WIT), surgical time, blood loss, drain tube output and time to withdrawal, surgical pathology, surgical margin, complications, and length of stay were evaluated.
Surgical technique
After a standard transperitoneal LPN approach has been carried out, the renal pedicle is identified and carefully dissected.9–11 PRF is then completely incised along with the renal capsule all the way from the lower to the upper renal pole. Decapsulation of the renal parenchyma is performed until the tumor appears; in that moment, PRF and tumor capsule are circumferentially cut, avoiding tumor decapsulation and leaving tumor, renal capsule, and PRF in the same surgical specimen. Renal pedicle is clamped and traditional tumor resection is performed under WIT. The first line of suture is performed with subsequent early unclamping. At this moment, the size of the surgical defect is estimated and an equal size and shape defect is tailored from a reabsorbable mesh (NU-KNIT sheet; Ethicon Endo-Surgery™). The latter is placed overlapping the renal defect and left in place as a synthetic renal capsule that aids in final renorrhaphy. Final renorrhaphy is carried out with the usual sliding clip technique using hem-o-lok and using the mesh as a true renal capsule (Figs. 1 and 2).
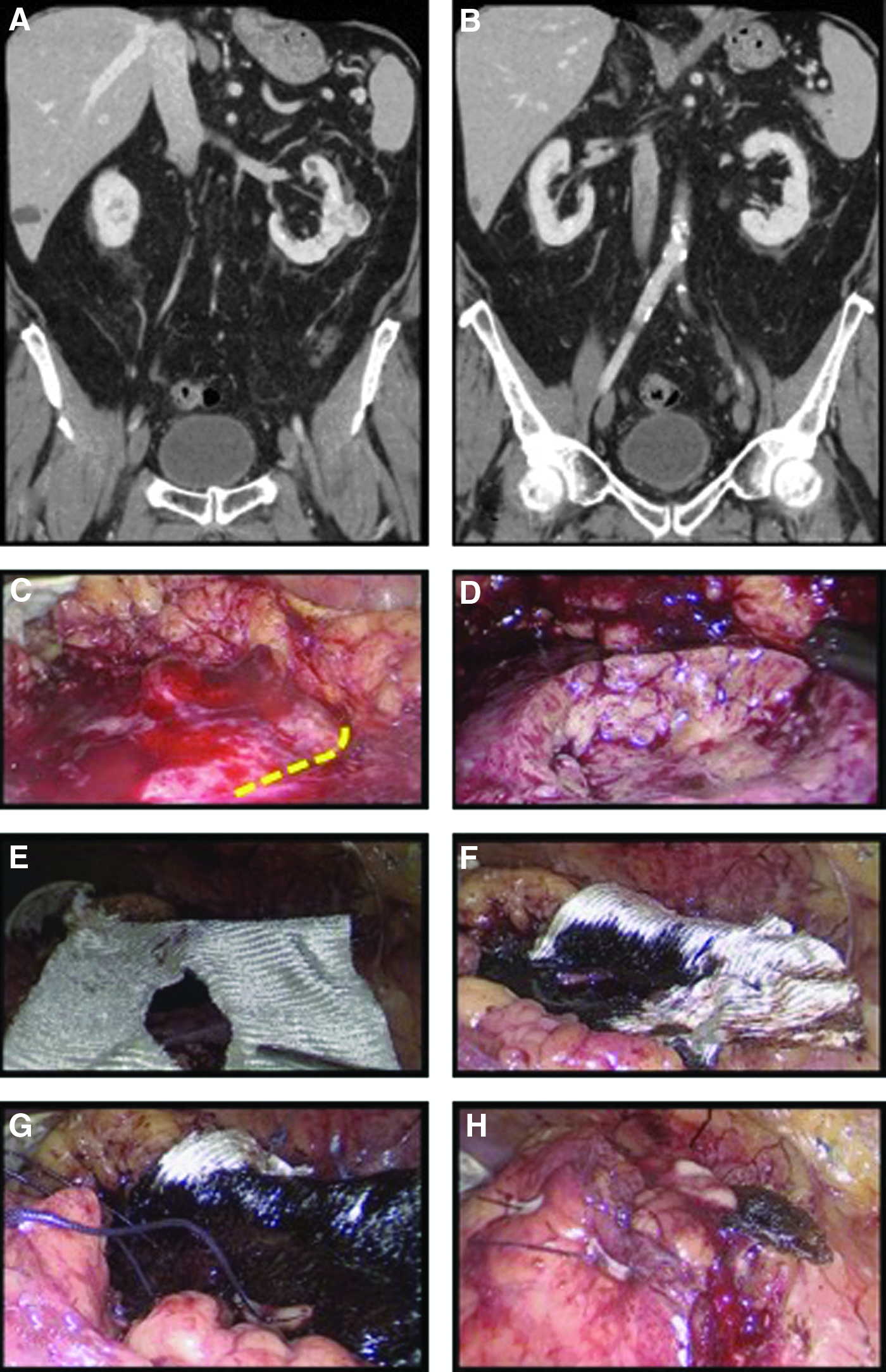
A tomographic image showing a left renal mass (T1a) with MAP score 4
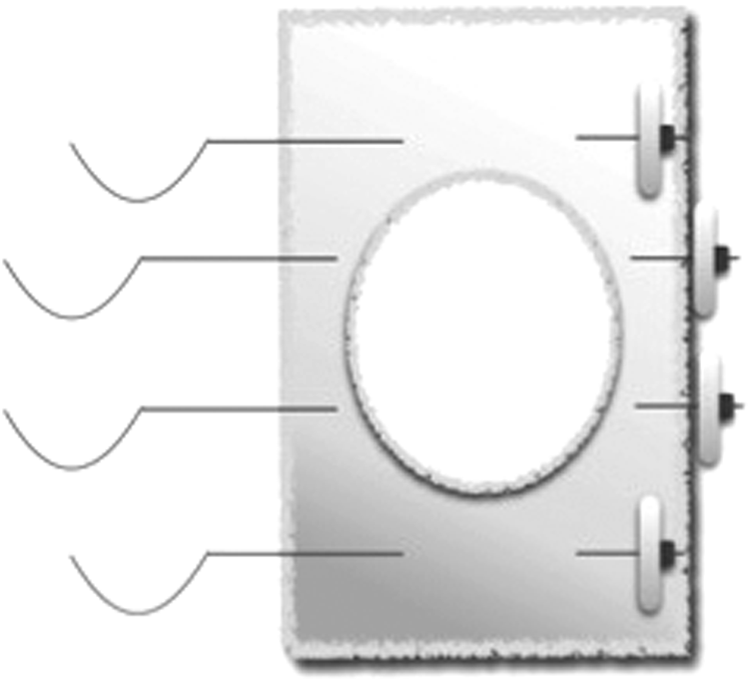
A simple diagram of renorrhaphy over the synthetic renal capsule.
We describe this novel technique in the setting of LPN. However, it can easily be extrapolated to open partial nephrectomy.
Results
A total of six cases were performed with the synthetic renal capsule tailoring (SYRCT) technique between April 2014 and February 2016. All cases were LPN and performed by the first author at our institution. All patients were male with a mean age of 70 years (range 62–76 years) and mean body mass index of 30 kg/m2 (23.66–33.86). Four cases were left and two were right. All patients had CT scans with a RENAL score of: 8a, 7p, 7x, 5x, and 5a in two cases. MAP score was 4 in four cases and 5 in the remaining two. Of the six cases, five were T1a and one T1b. Mean tumor size was 2.83 cm (range 1.2–6 cm). Mean operative time was 121 minutes (range 74–150 minutes), and mean WIT was 17.2 minutes (range 13–25 minutes). All but one patient underwent renal pedicle clamping. Only the renal artery was clamped in four cases and the whole pedicle in one case. Mean operative bleeding was 128 mL (range 50–250 mL). All patients had a drain tube in place, which was withdrawn before discharge, and mean hospital stay was 2.3 days. Mean drain tube output was 266 mL during the whole stay. There were no surgical complications greater or equal to Clavien II. Final pathological analysis revealed: clear cell renal carcinoma (CCRC) in five cases with Fuhrman 1, 2 and 3 in one, three, and one case, respectively. There was one case of oncocytoma. All margins were negative (Table 1).
BMI, body mass index; MAP, Mayo Adhesive Probability; WIT, warm ischemia time.
Discussion
Adhesive perirenal fat (APF) is a well-known factor that may jeopardize even the simplest partial nephrectomy. Renal mobilization, tumor localization, and capsular preservation may be severely impaired in cases with APF. MAP is a simple and reliable tool that was developed to predict APF and its possible consequences. High MAP scores (4 and 5) have a predictive value between 86% and 100%. 4 In our 6-patient series, all patients presented with MAP 4–5 (severe APF). Kocher et al. find a direct correlation between MAP and malignant pathology. 6 Another study by Thiel et al. proposes a direct correlation between a high MAP score and disease-free survival. 7
Retrospective evaluation of patients with APF has proven a direct association with longer operative times not only in partial nephrectomies but also in donor nephrectomies.5,12,13 We can correlate these difficulties to: (a) increase difficulty in renal dissection and mobilization and (b) increase difficulty in renorrhaphy. Severe APF may impair clear visualization of healthy renal parenchyma and increase the probability of decapsulation. Two different groups demonstrated that the absence of renal capsule at the moment of renorrhaphy severely weakens parenchyma strength, while the presence of it helps withstand pressure from the suture allowing for adequate hemostasis.8,14 In essence, capsular indemnity is vital for quality suturing.
Subcapsular dissection has been previously described for radical nephrectomy, but not in partial nephrectomies. 15 Decapsulation is described as an accidental event or as a necessity in cases with severe APF or previous surgery. We take a different aim at this common problem and suggest a completely different strategy. We prefer early and total decapsulation in cases with severe APF, avoiding collateral damage and unnecessary stress. SYRCT uses NU-KNIT (Ethicon Endo-Surgery), which is a very resistant and dense knitted absorbable hemostat, as a replacement for natural renal capsule. Even though the first author has performed over 200 LPNs, this strategy is simple and direct and the technique does not require extreme surgical proficiency to be reproduced. Even though our experience is small, it has proven to deliver excellent results in the six cases in which it was used.
Mean operative bleeding was 128 mL, mean operative time was 121 minutes, and mean hospital stay was 2.3 days with drain tube withdrawal before discharge. Our data cannot be directly compared with the results reported by Davidiuk due to the difference in surgical approach. However, when comparing them with international data, results can be considered favorable. 16
When a direct comparison is drawn between our cases with and without SYRCT, major decrease in operative time and surgical bleeding is evident. However, data are not enough to allow for a statistically significant conclusion. NU-KNIT has previously been used as replacement for anchoring the hem-o-lok in bolster sutures and also as “pledget” during running suture renorrhaphy. Nevertheless, these techniques require for an assistant to continuously monitor correct pledget position.17,18 On the contrary, SYRCT technique allows for easy NU-KNIT manipulation and placement.
NU-KNIT and Surgicel have been classically used as bolstering agents during renorrhaphy.19–27 Studies in animal models have shown no difference in surgical bleeding nor in fistula occurrence. However, more granulomas were found in the group with NU-KNIT on postoperative day 21. 28 We believe that this has no significant clinical correlation. It is noteworthy to mention that in our practice, we have abandoned the use of bolstering agents since it is our belief that they get in the way of correct visualization and suture placement with no confirmed benefit.
There are a limited number of publications regarding severe adhesive PRF during LPN. Management of this situation is controversial. We propose complete renal decapsulation with subcapsular dissection and SYRCT as a novel technique for these difficult situations. MAP score can strongly predict presence of severe adhesive PRF allowing for surgical planning. Using this novel approach, we were able to obtain results comparable to the ones we found in LPN with normal MAP scores.
Footnotes
Disclosure Statement
No competing financial interests exist.