
Abstract
Abstract
Background:
Laparoscopic antireflux surgery (LARS) is an excellent option for patients with symptoms refractory to medical treatment, for patients who have complications secondary to the use of proton pump inhibitors, and for those who do not want to take medications for a long period of time.
Hypothesis:
We hypothesized that (1) LARS has excellent outcomes if a complete preoperative workup and proper patient selection are performed and (2) recurrent symptoms often are not due to failure of the fundoplication to control the pathologic reflux.
Patients and Methods:
Every patient referred for antireflux surgery underwent a detailed symptomatic evaluation, barium swallow, esophagogastroduodenoscopy (EGD), high-resolution manometry (HRM), and pH monitoring. A fundoplication was performed in all of them. Data were analyzed to determine outcomes across 8 years.
Results:
From 2008 to 2016, 176 patients with gastroesophageal reflux disease (GERD) underwent LARS. One hundred and thirty-four patients (76.1%) had a total fundoplication, 31 (17.6%) had an anterior partial fundoplication, and 11 (6.3%) had a posterior partial fundoplication. Thirty-nine patients (22.2%) referred persistent or recurrent symptoms after the procedure and underwent EGD, HRM, and pH monitoring. Abnormal reflux was documented in 5 patients (2.8%). Among these failures, 3 patients had a body mass index (BMI) ≥30 and 2 had ≥35.
Conclusions:
The results of this study showed that (1) laparoscopic fundoplication is an effective procedure for GERD; (2) patient's BMI can affect the outcome of a fundoplication; and (3) pH monitoring is important to establish if recurrent symptoms are secondary to failure of the operation.
Introduction
G
Laparoscopic antireflux surgery (LARS) is an excellent option for patients who only have partial control of symptoms, for patients who do not want to be on long-term medical treatment, or when complications of PPI treatment occur. Today, however, even though the incidence of GERD continues to increase, patients and referring physicians are often reluctant to consider a fundoplication because of the fear of complications or poor results. As for other operations, a disparity in operative results between high-volume experts and low-volume providers has been documented. 1
With our study, we want to stress the importance of an accurate workup and proper patient selection for the outcome of LARS.
Patients and Methods
We performed a retrospective review of data from a prospectively maintained database at the University of Chicago Medical Center. Between 2008 and 2016, 336 patients with foregut symptoms who were thought to have GERD were referred for evaluation to the Center for Esophageal Diseases. They all underwent a careful symptomatic evaluation, barium swallow, esophagogastroduodenoscopy (EGD), high-resolution manometry (HRM), and pH monitoring.
Esophageal manometry
Medications that interfere with esophageal and gastric motility were discontinued 3 days before the study. The manometric protocol included an initial period of adaptation to allow individuals to adjust to the presence of the transnasal catheter, followed by a 30-second period for landmark recording and 10 wet swallows at 30-second intervals. Acquisition and data analysis were obtained with dedicated software.
Esophageal pH monitoring with dual-channel catheter
During the study, the patients consumed an unrestricted diet. Acid-reducing medications were discontinued 3 (H2 blocking agents) to 10 days (PPIs) before the study. Ambulatory pH monitoring was performed by placing a dual-channel pH catheter with two sensors located 15 cm apart, with the distal sensor positioned 5 cm above the upper border of the lower esophageal sphincter (LES). Ineffective esophageal motility was defined as amplitude of peristalsis in the distal esophagus of <30 mmHg or more than 30% simultaneous waves.
Esophageal pH monitoring with Bravo capsule
The capsule contains a pH electrode that samples esophageal pH every 6 seconds and data are transmitted to a receiver unit. The pH sensor was positioned 5 cm above the squamous columnar junction. No medications affecting gastrointestinal function were allowed during the monitored period. H2 blockers and PPIs were discontinued 3 and 10 days, respectively, before the test. Patients maintained a diary of events, including symptoms, meals, and sleep. They returned at the end of the recording period, 48 hours later, and the data were analyzed using a commercially available software program.
The data from dual-channel catheter and Bravo capsule were incorporated into a composite score (DeMeester score), and values <14.7 were considered normal.
Technical elements of the fundoplication
(1) Fundic mobilization by dividing the short gastric vessels, (2) identification of both anterior and posterior vagus nerves, (3) accurate dissection of the posterior mediastinum to bring the gastroesophageal junction 3 cm or more below the hiatus, (4) approximation of the right and left pillar of the crus with nonabsorbable suture, (5) use of a bougie at 56 Fr, and (6) use of the fundus to create a 360°, a posterior 240°, or an anterior 180° fundoplication. 2
This study was approved by the IRB of the University of Chicago.
Results
Of the 336 patients, 9 patients (2%) with documented reflux were excluded because their body mass index (BMI) was >40 and were referred to the bariatric clinic. One hundred and fifty-one patients (45%) were excluded because of a normal workup (normal EGD and pH monitoring). One hundred and seventy-six patients with proven GERD underwent antireflux surgery. Eighty-seven patients (49.4%) were male, and the mean age was 52 years. The mean BMI was 29: in 111 patients (63.1%), the BMI was <30 with a median of 26.5 (20–29); in 47 patients (26.7%), the BMI was ≥30 and <35 with a median of 31 (30–34); and 18 patients (10.2%) had a BMI ≥35, with a median of 36 (35–39).
Patients had been symptomatic for an average of 112 months (Fig. 1): 164 patients (93.2%) complained of heartburn, 155 (88.1%) of regurgitation, 74 (42.1%) of dysphagia, 21 (12%) of noncardiac chest pain, 130 (73.9%) of cough, and 91 (51.7%) of hoarseness. Symptoms were classified as a simple yes/no, and GERD-HRQL (Health Related Quality of Life) scores were not used pre- and postoperatively.
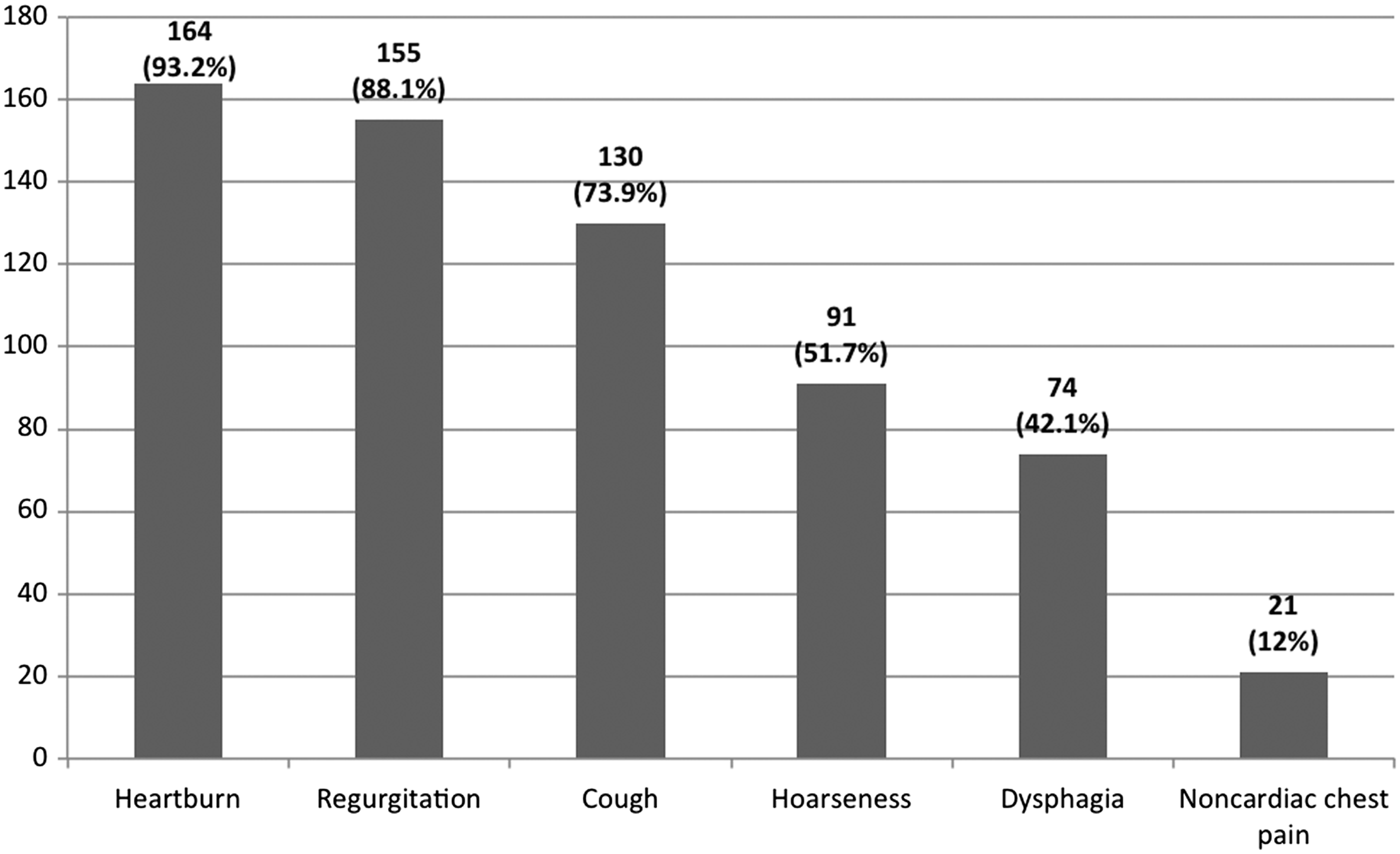
Prevalence of symptoms in 176 patients with GERD who underwent LARS. GERD, gastroesophageal reflux disease; LARS, laparoscopic antireflux surgery.
All patients had been treated with twice a day PPI for a mean duration of 107 months. One hundred and fifty-nine patients (90.3%) had partial response to medical treatment, while 17 patients (9.7%) had complete relief of symptoms. Among these 17 patients, 9 did not want to be on long-term medications, 4 had Barrett's esophagus (BE), 3 had osteoporosis, and 1 had recurrent cardiac arrhythmias secondary to hypomagnesemia.
The barium swallow showed normal anatomy in 43 patients (24.4%), while a hiatal hernia was present in 133 patients (75.6%).
The EGD was normal in 72 patients (40.9%). Esophagitis was present in 67 patients (38.1%). Thirty-seven patients had BE: metaplasia in 35 patients (19.9%) and low-grade dysplasia in 2 patients (1.1%).
HRM showed that the LES was hypotensive in 56 patients (32%). Peristalsis was normal in 95 patients (54%); 25 patients (14%) had ineffective esophageal motility; and in 16 patients (9%), esophageal peristalsis was absent. In 1 patient (0.6%) with BE, esophageal manometry was not performed because of an insurance-related issue.
A pH monitoring with dual-channel catheter was performed in 169 patients (96%). This technique allows us to measure the proximal extent of reflux (20 cm above LES) and to correlate extraesophageal symptoms such as cough with proximal reflux. Seven patients (4%) who did not tolerate the pH catheter had the Bravo pH capsule placed at the time of endoscopy.
The mean DeMeester score was 52.
One hundred and thirty-four patients (76.1%) had a total fundoplication, 31 (17.6%) had and anterior partial fundoplication, and 11 (6.3%) had a posterior partial fundoplication. A partial fundoplication was chosen when patients complained of preoperatively of dysphagia and esophageal manometry showed ineffective esophageal motility. An esophageal lengthening procedure was not performed in any patient.
Mean estimated blood loss was 18.5 mL. One patient (0.6%) required a laparotomy because of severe adhesions and bleeding. The median length of hospitalization was 24 hours.
Mortality and morbidity
The mortality rate was 0%. In 1 patient (0.6%), a laparotomy was performed for control of bleeding. Two patients (1.1%) had a trocar site infection. One patient (0.6%) had an incisional hernia at the midline trocar site.
Thirty-nine patients (22.2%) referred recurrence of symptoms (Fig. 2). They were evaluated by barium swallow, EGD, HRM, and pH monitoring. Abnormal reflux was documented in 5/39 patients (13%) after either a total fundoplication (3 patients) or an anterior partial fundoplication (2 patients). EGD showed esophagitis in 2 patients. HRM postoperatively confirmed the absence of esophageal peristalsis in 1 patient with scleroderma and showed normal motility in the other 4 patients. The barium swallow revealed a patulous esophagus without contractility in the patient with scleroderma and a slipped fundoplication was found in the other 4 patients. An alternative cause for the heartburn was found in 7 patients only (3, cholelithiasis; 2 depression; 2 gastritis). We do not have an explanation for the remaining patients. Interestingly, 8 patients were happy that the pH monitoring was normal and decided to stop the PPI medications.
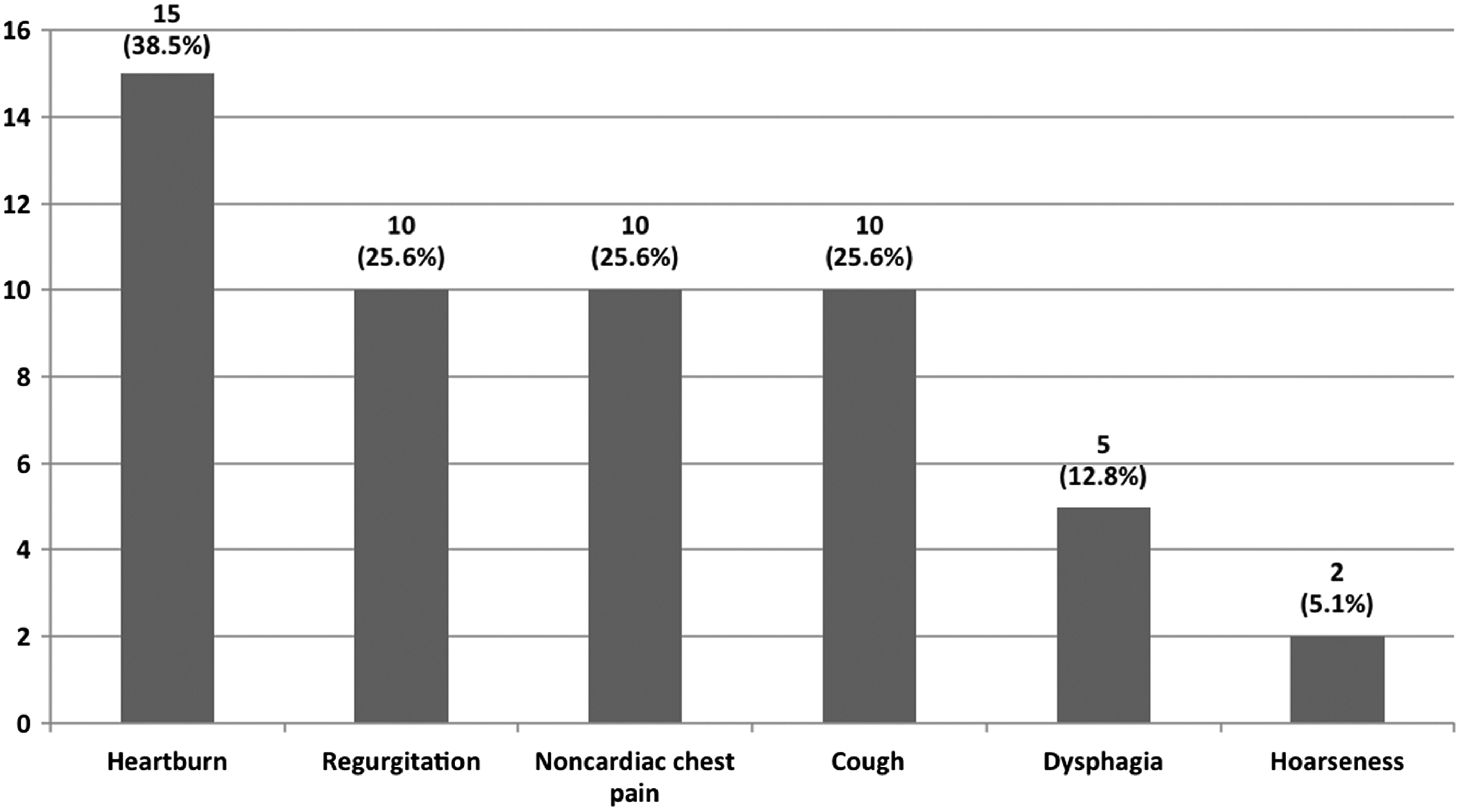
Recurrence of symptoms in 39 patients after LARS.
Of these 5 patients, 3 had a BMI ≥30 and 2 had ≥35 (Table 1). At a median follow-up of 17 months, the overall failure rate was 2.8%.
BMI, body mass index.
Discussion
The results of this study showed that (1) laparoscopic fundoplication is a safe and effective treatment for GERD; (2) a complete preoperative workup and patient's selection are essential for the success of the operation; (3) patient's BMI can affect negatively the outcome of a fundoplication; and (4) only a minority of patients who complain of recurrent symptoms have pathologic reflux.
GERD is a common disorder that affects almost 20% of the population in the United States. Medications are the first line of treatment, and PPIs are the most frequently prescribed drugs. A study from Shaheen et al., analyzing the healthcare costs in gastroenterology, reported that in 2004, the sales of PPIs in the United States reached 10 billion dollars. 3 A reason for this is that the majority of patients with GERD do well just with lifestyle modification and medical treatment. However PPIs are not always effective and safe. In a small percentage of patients, symptoms (particularly regurgitation) are not controlled by medications. In addition, some patients experience complications of PPI therapy. Several studies have shown that long-term treatment with PPIs is associated with side effects such as Clostridium difficile infection, community-acquired pneumonia, hip fracture, vitamin B12 deficiency, and hypomagnesemia. 4 Recently, their use has also been associated with an increased risk of myocardial infarction (in the general population, in patients with unstable coronary syndromes, and in patients with clopidogrel treatment)5–8 and chronic kidney disease. 9 Therefore, today a fundoplication is indicated for patients who present with refractory symptoms or experience complications due to PPIs.
A complete preoperative workup and patient selection are of key importance for the success of the operation. As shown in our study, only half of patients presenting with GERD symptoms had abnormal reflux and some had a very high BMI (more than 40), for which a bariatric procedure was indicated. 10 The Esophageal Diagnostic Advisory Panel achieved a consensus on the optimal preoperative evaluation for patients with reflux. This experience and evidence-based consensus indicated that upper endoscopy, barium esophagram, esophageal manometry, and pH monitoring are required before surgery. 11 Endoscopy is often the first test requested to confirm GERD, but due to its low sensitivity and specificity, its main utility is to determine if BE is present and rule out gastric and duodenal pathology.12,13 The barium swallow has a great value in the planning of the operation as it provides important anatomic information such as the presence, size, and type of a hiatal hernia. Esophageal manometry is important to rule out esophageal motility disorders such as achalasia, to detect the absence of peristalsis in patients with connective tissue disorders, and for properly positioning the pH probe.14–16 Ambulatory pH monitoring is the gold standard for the diagnosis of GERD. In addition, it gives important information regarding the correlation between episodes of reflux and symptoms.
Overall, it has been shown that an inadequate preoperative workup is one of the factors that frequently cause failure of LARS.17–19
Some studies have also shown a link between obesity and GERD. This relationship has been attributed to an increased transdiaphragmatic pressure gradient (more positive intragastric pressure and more negative intrathoracic pressure). For this reason, a Roux-en-Y gastric bypass, rather than a fundoplication, should be offered to patients with a BMI >35, particularly if central obesity is present.20,21 In our study, we found a significant increase of failures directly proportionate to patient's BMI (Table 1). We do recognize that this recommendation may not be practical for some patients who either do not want to have bariatric surgery or who do not have the operation approved by their insurance. We do ask these patients to lose weight and we refer them to a nutritionist for counseling. Otherwise, we eventually perform the fundoplication after a clear discussion about the alternatives, the benefits, and the risks, stressing in particular the risk of recurrence of a hiatal hernia and of pathologic reflux.
The management of patients who fail antireflux surgery is complex, but before assuming that the operation has failed, it is important to perform a careful evaluation. 22 Among the 39 patients (22%) coming back with symptoms (Fig. 2), we found that only 5 of 39 (13%) still had a pathologic amount of reflux. This finding stresses the fact that a symptom-based diagnosis is not accurate and that esophageal function tests (HRM and pH monitoring) are essential in the evaluation of these patients.
Study limitations
We do acknowledge that some limitations in this study are present:
• It is retrospective. • We only measured acid reflux, while an impedance pH monitoring would have allowed the recording of nonacid episodes of reflux. • Heartburn was classified as yes/no. GERD-HRQL scores were not available pre- and postoperatively for our patients. The study had a relatively short follow-up (17 months).
Conclusions
The results of this study showed that (1) laparoscopic fundoplication is a safe and effective procedure for GERD when a complete workup and proper patient selection are performed; (2) patient's BMI affects the outcome of a fundoplication; and (3) postoperatively, esophageal function tests are essential to establish if recurrence of symptoms is indeed due to reflux.
Footnotes
Disclosure Statement
No competing financial interests exist.