
Abstract
Abstract
Background:
Despite the obvious technical advantages, the value of robotic surgery is highly debated and its cost-effectiveness has been questioned. The aim of this article is to provide an evaluation of the outcomes of robotic surgery in comparison to conventional laparoscopy.
Methods:
A decision analysis based on the Bayes' theorem and the decision tree was used. The robotic approach was compared with the laparoscopic approach for each of the pathologies discussed in this study. The data on robotic surgeries were obtained from a retrospective study conducted between January 2008, when the da Vinci system became available in our institution, and December 2014. During this period, 343 consecutive robotic operations were performed by a single surgical team.
Results:
There were statistically significant differences in the likelihood of an optimal patient outcome when the robotic approach was used for hysterectomies to remove malignant tumors, difficult splenectomies, gastrectomies, and rectal resections. The results did not show important differences between the two techniques for easy splenectomies and hysterectomies for benign cases.
Conclusions:
The results of our study confirm the value of robotic surgery, as an alternative and complex surgical tool, for hysterectomies to remove malignant tumors, difficult splenectomies, gastrectomies, and rectal resections. Laparoscopy was preferred for easy splenectomies and hysterectomies for benign cases, because of the lack of improved outcome with robotic surgery and the high cost of robotic surgery.
Introduction
R
The aim of this article is to provide an evaluation of this expensive technology and to evaluate the outcomes of robotic surgery in comparison with conventional laparoscopy. What we are proposing is the analysis of the wide experience in robotic interventions of a single surgical team. Studies based on the experiences of a single surgical team consist of a less heterogeneous population and avoid the effect of the learning curve that can cause difficulties in interpreting clinical studies. However, it should be noted that there are also disadvantages to a study based on the work of a single surgical team. Those disadvantages are as follows: (1) a smaller number of cases and (2) a preference for using the approach with which the surgical team has achieved better results and had fewer complications, or for which the surgical team has been specialized. As in every domain of medicine, the decision to select a particular surgical approach is based on two principal sources: data from the literature and data from personal experience.
To establish which patients may benefit from the robotic approach, it is necessary to integrate the results of multiple previous studies (representing the current state of knowledge), with the analysis of our clinical experience. The concept of updating of beliefs or evidence is the essence of Bayesian method. 3
According to these considerations, our goal is to make a decision about the real usefulness of the robotic approach using the Bayesian statistical analysis.
Materials and Methods
Systematic literature review
The potential eligible articles were evaluated by two of the authors independently, using the following inclusion criteria (1) the article was published in the past 10 years; (2) the patient outcome data after an abdominal robotic surgery were compared with those of conventional laparoscopy and open surgery; and (3) the patient outcome data were reported in detail (intraoperative trauma and complications, postoperative complications, biological effects, oncological results, and clinical benefits after surgery). When studies from the same institutions or based on the same populations were identified, only the most recent articles with the most up-to-date data were included, to avoid duplication. PubMed was searched for relevant studies published up to November 2015 as the primary source. Initially, using the terms “robotic surgery” + “10 years,” 8370 articles were identified. Next, the search was refined using more specific key words, and 3059 articles were identified (Table 1).
From these articles, 2955 were excluded, because of irrelevance or duplication. Out of the remaining 104, 58 were excluded because of lack of eligibility criteria. Finally, only 46 articles were taken into consideration to establish the prior probabilities.4–49 Articles were eligible for inclusion in the analysis when clear enough information on patient perioperative outcome was available. The subjective selection of the literature described above was weighted with the level of evidence of each article (Fig. 1) (Oxford Centre for Evidence–Based Medicine. Levels of Evidence Working Group. “The Oxford 2011 Levels of Evidence”).
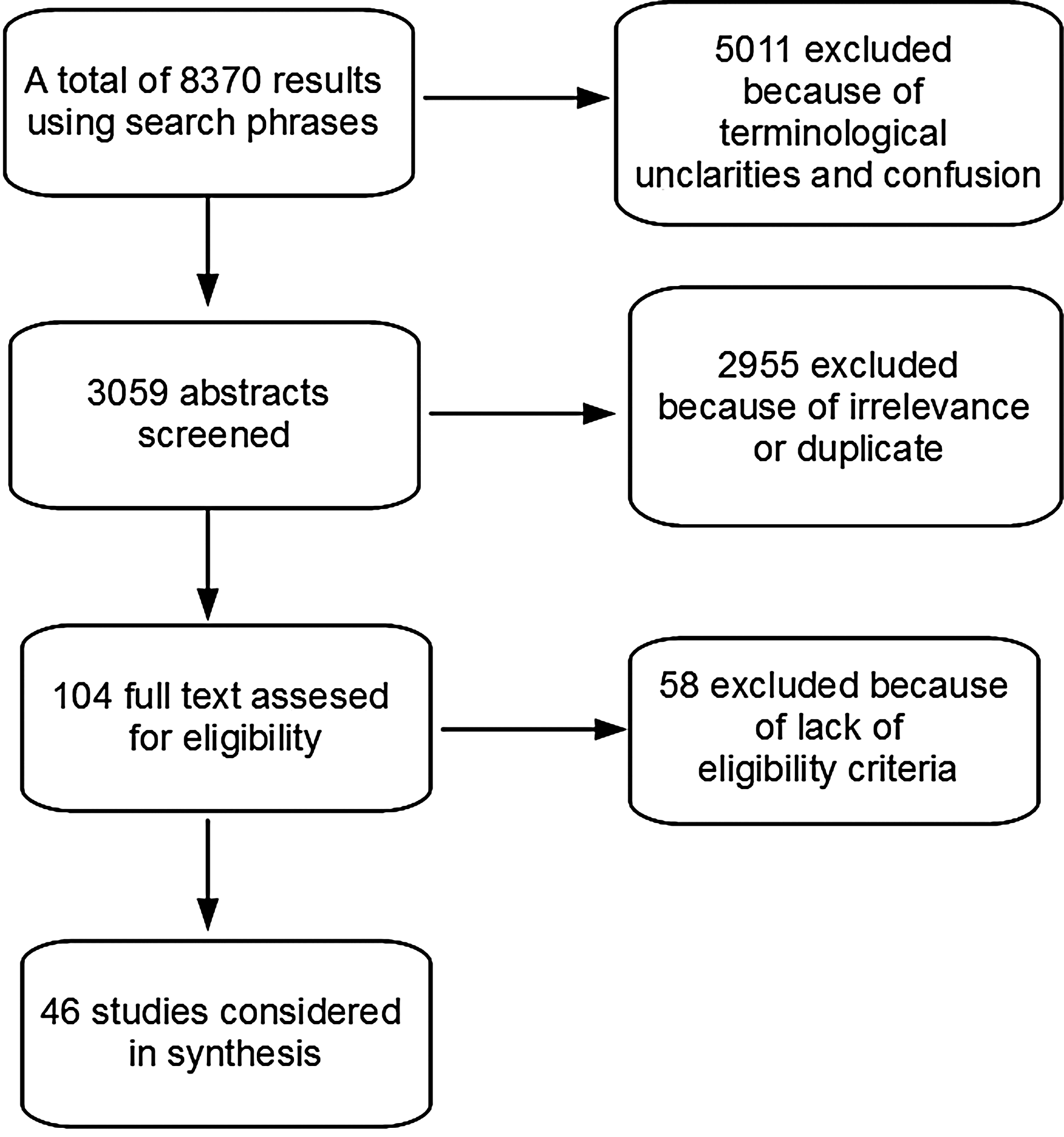
Systematic literature review—flowchart diagram.
Analysis of our clinical experience
The study also includes data from our own surgical experience. The laparoscopic surgery data are taken from our patient databases. The robotic surgery data were gained from our retrospective study conducted between January 2008 and December 2014, when the da Vinci system was available in our institution. During this period, 343 consecutive robotic operations were performed by a single surgical team.
Bayesian analysis
A decision analysis based on the Bayes' theorem and the decision tree method was used herein. To build decision trees we integrated probabilities estimated from the systematic review of speciality literature with the analysis of our own surgical data, represented as optimal patient outcome and nonoptimal patient outcome. These data were prior probabilities, according to Bayesian statistical method. The robotic approach is compared to the laparoscopic approach for each of the pathologies discussed in this study. The “optimal outcome” criterion refers to a minimal intraoperative trauma, a minimal number of postoperative complications, and a maximal clinical and biological benefit for patient (Fig. 2). The result of the method is considered posterior probability or posterior distribution and is represented in our study as the chance for an optimal or nonoptimal patient outcome when using a certain surgical approach, namely laparoscopic or robotic (Fig. 3).
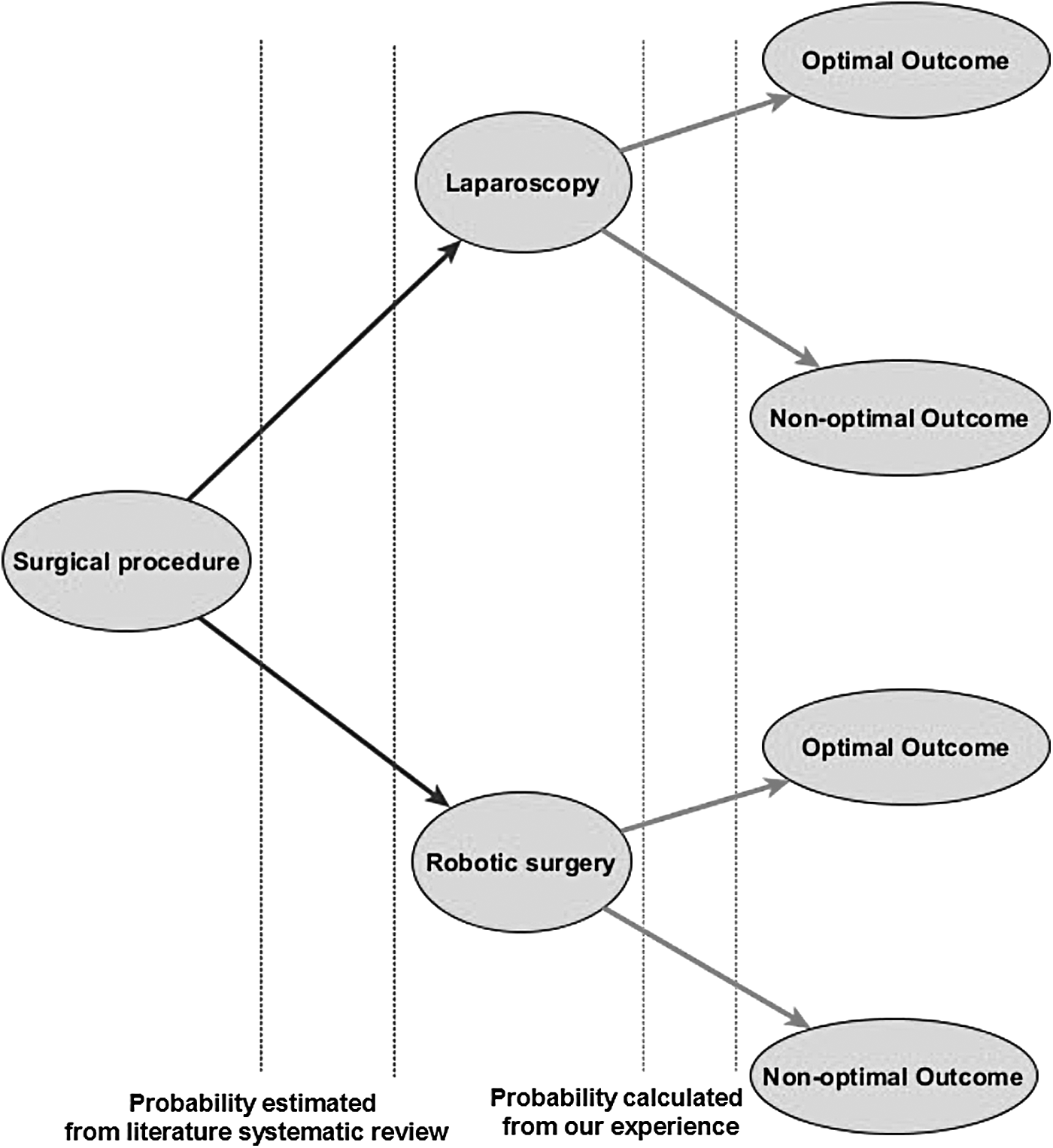
Representation of the structure of a Bayesian decision tree.
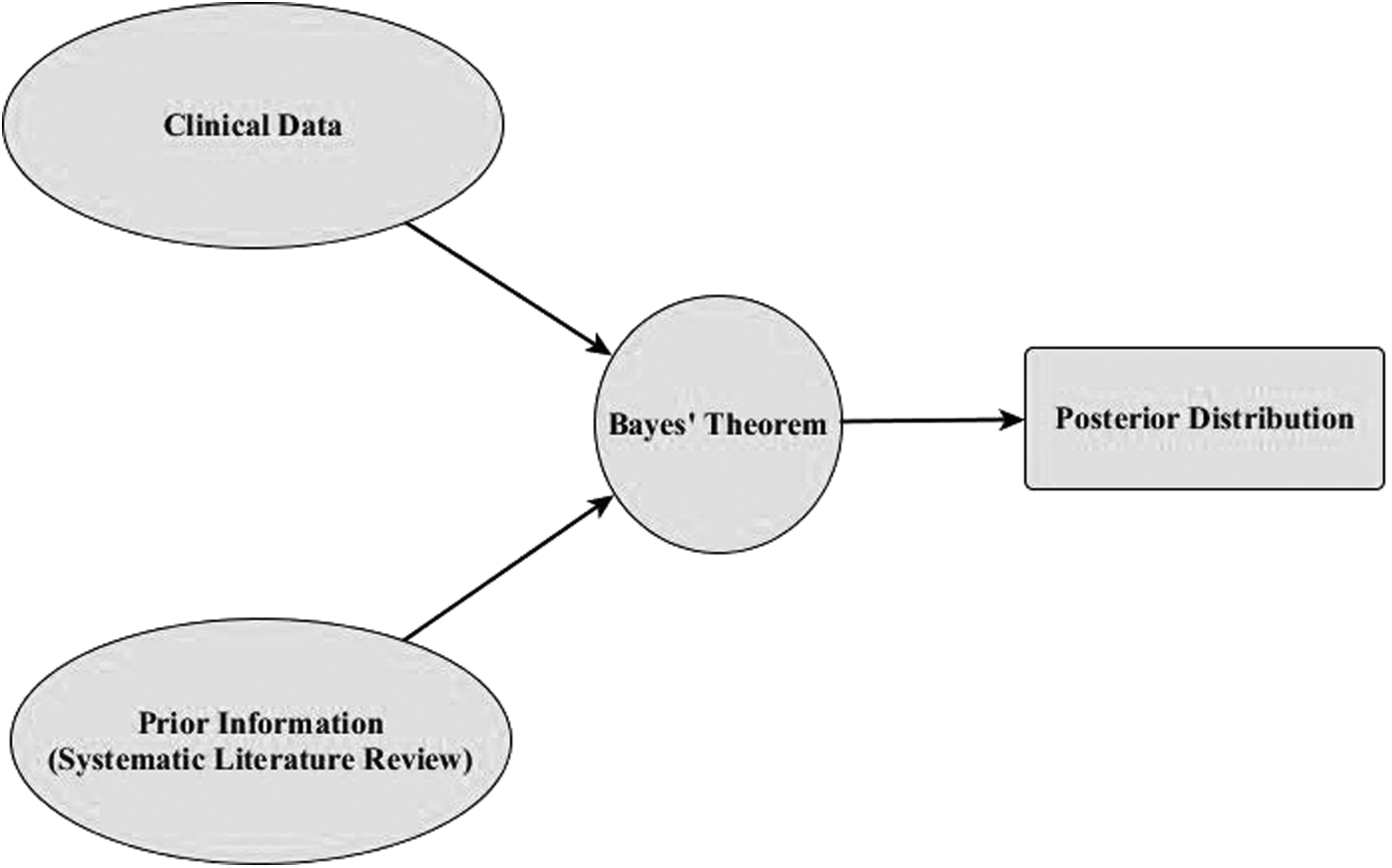
Bayesian analysis incorporates prior information in addition to the sample data, to provide posterior probability distributions.
Results
Systematic literature review
The prior probabilities for each of the indications are presented in Table 2. The prior probability is the unconditional probability that is assigned before any relevant evidence is taken into account. It can be determined from past information, such as previous studies, like in our case. A prior probability is the key part of Bayesian inference and represents the information about an uncertain parameter that is combined with the probability distribution of new data to yield the posterior distribution, which in turn is used for future inferences and decision involving that of prior probability.
Analysis of our clinical experience
The clinical data used in our analysis are derived from the surgical team experience. For example, in the case of hysterectomies due to malignant indication, our previous studies indicate that ∼3% of patients experienced major perioperative complications (nonoptimal outcome) when the robotic approach was used. In contrast, patients undergoing laparoscopic procedures for this same medical condition had an 8% incidence of nonoptimal outcomes. The remaining patients obtained an optimal perioperative outcome. A total of 132 robotic operations were performed for various gynecologic pathologies, including 103 total hysterectomies for uterine cervical neoplasm, endometrial neoplasm, and/or uterine fibroids; 15 were pelvic exenterations; 7 were anexectomies and 7 represented ablation of pelvic endometriosis nodules; ablation of genital neoplastic recurrences in the pelvic region, or final lymphadenectomy after operated genital neoplasm. This accrued experience with robotic operations led to improved performance in terms of length of the surgery (which became comparable to that of laparoscopic or open surgery), minimal intraoperative blood loss and intraoperative complications, precision in performing the dissections, lymphadenectomy and sutures, and small number of postoperative complications. 50
A total of 84 robotic surgeries were splenectomies, out of which 55 were total splenectomies, 26 were subtotal splenectomies, and 6 were partial splenectomies. The indications were as follows: hereditary microspherocytosis, idiopathic thrombocytopenic purpura, non-Hodgkin lymphoma with splenic involvement, autoimmune hemolytic anemia, splenic cysts, important splenomegaly with hypersplenism of unspecified cause, and splenomegaly due to cirrhosis. In case of splenectomies, only difficult cases were referred to robotic surgery. The most difficult cases are as follows: partial splenectomy, splenectomy in liver cirrhosis, splenic tumors, or malignant hemopathies, all requiring better dissection of the splenic vessels and precise and time-efficient intracorporeal maneuvers. 51
Our team performed a total of 54 robotic gastrectomies as follows: 23 total gastrectomies, 18 subtotal gastrectomies, and 13 other types of gastric procedures for different gastric pathologies, represented by gastric polyps, giant ulcer of small gastric curvature, neuroendocrine tumors, etc.
For the pathology of rectum, 40 robotic operations were performed, out of which 28 were Dixon rectosigmoid resections, 4 were Hartmann rectosigmoid resections, and 8 were abdominoperineal resections.
Regarding the pathology of the esogastric junction, 5 robotic operations were performed for hiatal hernia and 16 operations for achalasia, and for the pathology of the pancreas,1 distal pancreatectomy and 2 total pancreatectomies. Eight additional robotic surgeries were conducted for other pathologies, including double ligature of splenic artery for splenic artery aneurysm; enucleation of adrenal tumor; pseudocyst-gastric anastomosis for pancreatic pseudocyst, left nephrectomy for left hydronephrosis degree V; ablation of interrectosacral tumor; left adrenalectomy; duodenojejunal angle resection; and an anastomosis between ductus choledocus and duodenum. The number of these procedures is too small, to be statistically relevant.
Bayesian analysis
Using the Bayes' theorem, the posterior probability of each surgical approach, robotic or laparoscopic, was appreciated considering the chance to produce optimal or nonoptimal outcome for the patient. After the tree structure representation, the expected feasibility of each surgical approach was calculated to discriminate between an optimal or nonoptimal outcome of the procedure. The capacity of each of these data to discriminate between a case with an optimal outcome and one with a nonoptimal outcome, when using a certain surgical approach, laparoscopic or robotic, was appreciated considering the differences between the two probabilities.
Hysterectomies for malignant indication
When using the robotic approach, the chance for an optimal outcome is 72%, and when using the laparoscopic approach is 23%, and this is a significant difference (Fig. 4). We observed that the robotic system shows the greatest advantage over laparoscopy during lymphadenectomies. The 7 degrees of freedom of the EndoWrist® instruments allow easier and more accurate removal of the nodes in the proximity of large vessels. The extended para-aortic lymphadenectomy is facilitated in the case of obese patients, without any major blood vessel injuries. Most of the patients that underwent operations for cervical neoplasm presented with stages IB, IIA, and IIB, for which they underwent neoadjuvant radiotherapy and brachytherapy. These therapies led to development of pelvic fibrosis and retracted tissue. This increased the difficulty of intraoperative differentiation of the fibrosed tissue from the malignant tissue. The high precision of the robotic instruments and the improved ergonomics provided to the console surgeon allowed a precise and safe anatomic dissection. The incidence of intraoperative hemorrhage and postoperative complications, such as vesicovaginal or rectovaginal fistulas, was reduced with the robotic instruments.
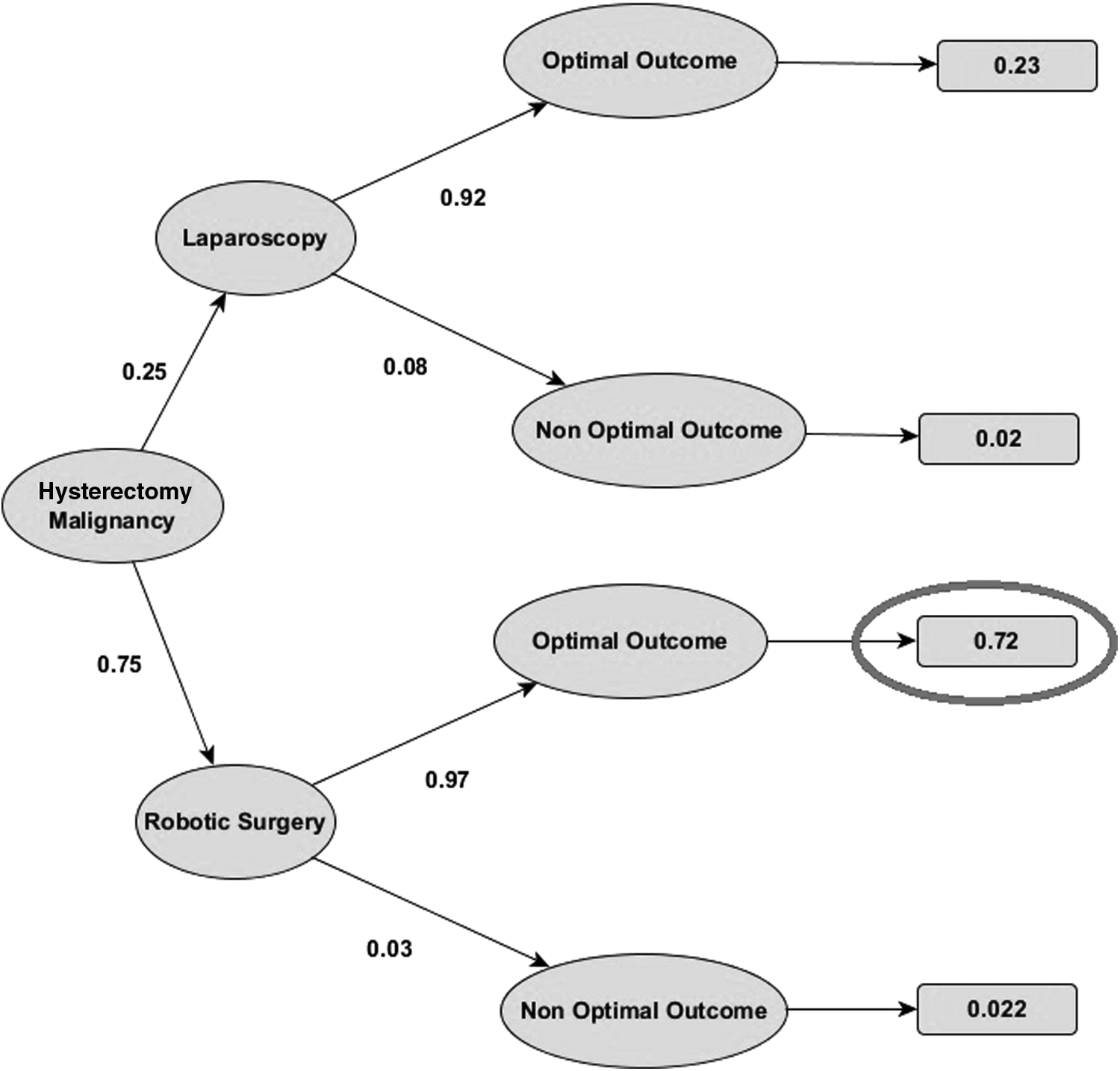
Bayesian decision tree representing the result of the Bayes analysis for hysterectomy for malign indication.
Difficult splenectomies
The probability of achieving an optimal outcome using a robotic approach is 59% and by laparoscopy is 37%, which is a significant difference (Fig. 5). From experience, in the case of massive splenomegaly or thrombocytopenia with great risk of bleeding, laparoscopic resection is difficult because of the limited workspace and the spleen's adherence to adjacent organs. In cases of liver cirrhosis with splenomegaly, robotic surgery has clearly shown a decreased risk of intraoperative hemorrhagic complications and blood loss. In cases of splenic tumors, unlike with laparoscopy, the robotic system allows one to maintain the integrity of the capsule and to minimize the tumor dissemination.

Bayesian decision tree representing the result of the Bayes analysis for splenectomy in difficult cases.
Gastrectomies
According to Bayes' theorem, the probability to achieve an optimal outcome is 57% when using the da Vinci robot for gastrectomies and 34% when using the laparoscopic approach, as shown in Figure 6. There are statistical differences between robotic-assisted gastrectomy (RAG) and laparoscopic-assisted gastrectomy (LAG) in terms of optimal outcomes.46,52 Tremor filtration and stereoscopic vision supplied by the robotic system allow the surgeon to precisely dissect tumors and lymph nodes along the celiac trunk, the left gastric artery, and the hepatic pedicle, thus reducing blood loss during surgery. 53 We can appreciate that the differences between the two techniques mainly come from these criteria. LAG has the disadvantage of the restricted range of instrument movement and hand tremor amplification and those features burden the precise lymph node dissection or hemostasis.

Bayesian decision tree representing the result of the Bayes analysis for gastrectomy.
Rectal cancer resection
According to Bayes' theorem, the probability to achieve an optimal outcome when using the robotic surgery is 57% and when using the laparoscopic surgery is 34%, as shown in Figure 7. Like in the case of gynecological pathology, the robotic system shows a clear advantage in comparison with the laparoscopic procedure. It is difficult to approach the pelvis with rigid instruments and because of the anatomical particularities of the area. Thus, all rectum cancers can be addressed robotically, except for the T4 stage cancers, which involve a multiorgan resection. Laparoscopy may not be suitable in cases where there has been previous abdominal surgery, as there might be adhesions that complicate the visual field and prevent the laparoscopic access without releasing such adhesions. Using the robotic approach for such interventions, we encountered a lower number of urinary and sexual complications, due to easier dissection and conservation of hypogastric nerves.54–57

Bayesian decision tree representing the result of the Bayes analysis for rectal resection.
Easy splenectomies and hysterectomies for benign indication
In case of easy splenectomies (Fig. 8) and hysterectomies for benign indication (Fig. 9), the results did not show important differences between the two techniques. We observe that the laparoscopic procedure is feasible in terms of optimal patient outcome and the robotic approach did not bring any important improvements. According to these observations, in these cases, we consider that the utilization of this expensive tool is not justified.

Bayesian decision tree representing the result of the Bayes analysis for splenectomy in easy cases.

Bayesian decision tree representing the result of the Bayes analysis for hysterectomy for benign indication.
Discussions
Bayesian analysis is a method of statistical inference in which Bayes' theorem is used to update the probability for a hypothesis as more evidence or information becomes available. The hypothesis of this study is that the robotic system is a breakthrough in comparison to traditional surgery and laparoscopic surgery, presenting multiple advantages for the patient and for the surgeon. Bayesian inference derives the posterior probability as a consequence of two antecedents, a prior probability, and a “likelihood function” derived from a statistical model for the observed data. The effect of the prior probability (existing evidence based on previously published clinical trials) on the posterior probability (ultimate analysis considering also the results of our own clinical experience) is considerable because “the posterior is proportional to the likelihood multiplied by the prior”. 58 Therefore, a systematic review is an appropriate tool for the evaluation of the previous research that can be condensed into an a priori probability. For systematic reviews, a clear set of rules is used to search for studies. All decisions regarding which studies will be included or excluded from the analysis are clearly specified, and the mechanisms are transparent, objective, and replicable. 59 One limitation of this approach is that it is subjective, that is, the analysis can manipulate the prior distributions to obtain a desired result. To avoid this manipulation, the authors were careful to develop probability distributions that were justifiable and understandable; hence we propose the Bayesian analysis as a method of integrating multiple data. 60 According to our results, the use of robotic approach is fully justified for the indications discussed below.
In case of robotic hysterectomies, three of the technical steps of the procedure are easier to be performed using robotic surgery, compared with laparoscopic, a fact that fully justifies its use in gynecological cancers. These are: the pelvic lymphadenectomy, the division of the parametrium, paracolpos, and uterosacral ligaments, and the dissection of the uterine artery.50,61 Regarding the pelvic lymphadenectomy, some authors 62 report the removal of statistically significant more lymph nodes in robotic surgery than in laparoscopic or open surgery (31.8 versus 25.9 versus 27.7, P < .001). Other authors report the removal of 17.5 nodes, 63 18 nodes, 64 and 25.9 nodes. 65 These results are comparable to our average of 22.23 nodes (17–25).50,61 Most of the authors recommend the use of minimal surgery in cervical cancer stages IA2–IB2, until a maximum of IIA.50,61 Most of the patients included in our database and operated for cervical neoplasm presented stages IB, IIA, and IIB, for which they underwent neoadjuvant radiotherapy and brachytherapy. These therapies led to increased operative difficulty due to pelvic fibrosis. The difficulty was overcome using the robot, which allows a precise and safe anatomic dissection, with no intraoperative complications.50,61 There are few reports of robotic-assisted anterior pelvic exenteration and one report of robotic-assisted total pelvic exenteration with ileal loop urinary diversion followed by end colostomy for treatment of recurrent cervical cancer. We performed a number of 15 robotic pelvic exenterations and achieved satisfactory oncological results due to the accurate and precise dissection and the extension of lymphadenectomy in the narrow space of the deep pelvis similar to robotic prostatectomy and total mesorectal excision. 66
Certain studies proved a statistical difference in favor of robotic splenectomy, regarding blood loss, vascular dissection duration, and splenic remnant size. Using a parameter, such as vascular dissection, could seem speculative, but it points out the advantages of robotic surgery.7,49,67 In 2012, our surgical team published a study, comparing the outcomes of laparoscopic versus robotic subtotal splenectomy, regarding the duration of the procedure (95 minutes versus 107.5 minutes, but with no statistical significance), blood loss (90 mL versus 35 mL, P < .05), vascular dissection duration (20 minutes versus 15 minutes, P < .05), and splenic remnant size (10.57 cm3 versus 8.16 cm3, P < .05). 49
Regarding robotic gastrectomies, a meta-analysis of seven studies revealed that the number of harvested lymph nodes did not differ significantly between RAG and LAG. In a recent study of our surgical team, we found out that the number of retrieved lymph nodes was not statistically different between the two procedures (P = .108) and neither was the rate of postoperative complications (P = .294), so the conclusion is that robotic gastrectomy is a safe procedure, with satisfactory short- and long-term outcomes in locally advanced gastric cancer. However studies on a larger number of patients are necessary to confirm if an immediate benefit in survival exists in case of robotic surgery. Like in other studies, we observed that the hospital stay for patients with open gastrectomy was longer than for those with robotic or laparoscopic gastrectomy, but there are no significant differences between the latter.53,68 Other studies reported no significant differences between the two techniques in terms of conversion rate, mortality, surgical complications, and oncological adequacy.46,52 Furthermore, a meta-analysis in 2014, which evaluated whether RAG is comparable to LAG, confirms our observations. The meta-analysis indicated that there is less blood loss in the RAG group than in the LAG group. With acceptable complication rates and radical resection, RAG is a promising approach that is superior to LAG or open gastrectomy. However, because of the lack of long-term studies, it is too early to draw a final conclusion. Long-term clinical outcomes should be further evaluated.53,69,70 Laparoscopic approach for gastric cancer is known to be complex and time consuming, so the robotic approach has a great potential for development. The robotic system seems to facilitate a proper lymphadenectomy in difficult to reach areas and a hand-sewn anastomosis, particularly after total gastrectomy. 71
In case of the rectal cancer, like in other studies, we found that the robotic surgery conversion rate was significantly lower than that for laparoscopic surgery, showing that robotic surgery provides better management of complex procedures and allowing more patients to benefit from minimally invasive surgery. The reasons for conversion to open surgery included obesity with heavy mesentery dissection, inability to identify important vascular structures, vascular injuries, adhesions, and narrow areas of operation. The conversion rate for laparoscopic rectal cancer surgery is usually high (34% of the rectal cancer operations were converted into open surgery in the MRC CLASICC trial).54–57
Another indication was the benign pathology of esogastric junction. A total of 21 interventions of this kind have been performed, out of which 5 for transhiatal gastric hernia and 16 for achalasia. Robotic surgery is the preferred choice in these cases, especially in large hernias, because the mobile instruments allow easy dissection of a large hernia sac.72,73 Our study shows that the robotic approach has similar outcomes to the laparoscopic approach in terms of complication rate, total surgical time, and hospital stay. There were no recurrences after the robotic procedures.
Conclusions
The results of our study confirm the value of robotic surgery, as an alternative and complex surgical tool, for certain cases addressed by general surgery.
Robotic surgery was best suited for procedures limited to the narrow region of the pelvis, namely for gynecological or colorectal indications and for those requiring fine dissection, microsuturing, and reconstruction, as in the case of difficult or subtotal splenectomies and gastrectomies.
In case of easy splenectomies and hysterectomies for benign indication, there are no important statistical differences between the two techniques. Hence, in these cases we preferred laparoscopy, to avoid the high cost of the robotic surgery.
Robotics offers many potential technical advantages to overcome the well-known limitations of conventional laparoscopic procedure and even of the open surgery. Because the benefit of robotic systems for general surgery is still a matter of debate, it is important to obtain an effective cost–benefit ratio. Consequently, a rigorous selection of the pathology and patients is mandatory.
Footnotes
Acknowledgments
This study was supported, in part, by CNCS-UEFISCDI project number 22 from August 28, 2013 (PN-II-IDPCE-2012-4-0018). The authors thank Prof. Leslie Cizmas and Prof. Paul Cizmas for reviewing the article.
Disclosure Statement
No competing financial interests exist.