
Abstract
Abstract
Background:
Herein, we evaluate the effect of pain relief after laparoscopic cholecystectomy (LC) of various intraoperative maneuvers through a prospective randomized study and identify the synergistic effects of combined maneuvers compared with a single maneuver that was shown to be useful in a previous report.
Methods:
Fifty-one patients who were scheduled for elective LC were randomly allocated to group A (26 patients, on whom were performed the combined maneuver) or group B (25 patients, no maneuvers). In group A, the patient underwent several maneuvers concomitantly during LC: injection of local anesthesia at the incision site, low-pressure pneumoperitoneum, active gas suction (AGS), and pulmonary recruitment. Pain after LC was assessed using the visual analog scale (VAS) and the measurement of analgesic consumption.
Results:
Four cases of postoperative morbidity relevant to the analgesic supplements developed (one case, 3.8%, in group A, and the others, 12%, in group B, P = .350) The mean analgesic consumption of group A was significantly lower than that of group B (48.1 ± 46.3 mg versus 106.7 ± 83.3 mg, P = .000), and VAS was also lower in group A at postoperative 6, 12, and 24 hours (3.7 ± 1.2 versus 4.8 ± 1.7, 1.5 ± 0.6 versus 3.3 ± 1.3, and 1.0 ± 0.6 versus 3.0 ± 1.7, respectively; P = .016, .000, and .000). Group A showed lower VAS than did a group in our previous study given AGS alone.
Conclusions:
Our combined maneuvers, comprising of various simple methods during LC, could be effective and feasible means of reducing the convoluted pain that occurs after LC, and also reduce the demand for analgesics.
Introduction
P
The aim of this prospective randomized study is to assess the relief of pain after LC and the decrease in demand for analgesics using the simultaneous performance of various simple maneuvers that can be implemented during the operation. Furthermore, we also identify the synergistic effect of the combined maneuvers for pain reduction through a comparison with the results of our previous study using a single maneuver, AGS, alone.
Materials and Methods
From February to May 2015, a total of 150 patients underwent elective LC for various cholecystopathies at the Seoul St. Mary's Hospital, Seoul, Korea. In the current study, the exclusion criteria included the following: (1) patients undergoing a concurrent operation on other organs, (2) patients who underwent LC to treat an acutely inflamed gallbladder, such as acute cholecystitis, gallbladder empyema, gangrenous cholecystitis, or emphysematous gallbladder, (3) patients who preoperatively underwent percutaneous transhepatic gallbladder drainage because of severe gallbladder inflammation, and (4) patients with a history of upper abdominal surgery, such as gastrectomy, small bowel resection, or right colectomy. Patients who underwent endoscopic retrograde cholangiopancreatography (ERCP) before LC for a concomitant choledocholith were also excluded because post-ERCP pancreatitis could affect the postoperative clinical course. As a result, 54 cases were enrolled in the trial and randomized. The current study was approved by the Institutional Review Board (IRB No. KC15EISI0037) and informed consent was obtained from all patients preoperatively.
Surgical procedures
LC was done using the standard technique with three trocars. 7 In special cases, we additionally inserted a fourth trocar at the subcostal anterior axillary incision. All operations were performed by 2 surgeons, each of whom had experience with >1000 cases of LC. After the specimen was bagged, saline irrigation was performed until all the fragments of the gallbladder or infected debris were clearly removed in the laparoscopic view. The specimen was retrieved through the umbilical trocar and a drain was not routinely used, except in unusual cases involving a high level of concern over bile leakage or delayed bleeding. If a drain was inserted, the case was excluded from this study.
Randomization and the clinical maneuvers used in the intervention group
The table of random sampling numbers was generated by a computer. After informed consent was obtained, a random sampling number was given to each individual case, and each was allocated to intraoperatively undergo the various maneuvers (group A) or not (group B). Immediately before the surgery, the scrub nurse opened the envelope holding the sampling number and informed the operator whether or not to perform the maneuvers. The patients in group A underwent the maneuvers during surgery, which consisted of the following: (1) local anesthesia injection at the incisional site. At the start of the operation, 4 mL of 0.5% bupivacaine was subcutaneously injected around each 5 mm trocar site, then 6 mL of 0.5% bupivacaine was also injected around the 11 mm umbilicus trocar site. (2) Low-pressure pneumoperitoneum. In group A, the intraabdominal pressure was kept at about 8 mmHg by carbon dioxide (CO2) insufflation, whereas the pressure was maintained at 12 mmHg in group B. (3) AGS. In group A, AGS was performed according to the method described in our previous report. 5 For patients in group B, the gas valves of all trocars were left open until the abdomen was completely deflated. (4) Pulmonary recruitment, as described in the report by Khanna et al. 6 At the end of the operation, the patient was placed in the Trendelenburg position and the pneumoperitoneum was eliminated by a pulmonary recruitment maneuver consisting of two manual infiltrations to the maximal pressure level of 60 cm H2O for 5 seconds.
Postoperative management and outcome assessment
All patients were given prophylactic antibiotics using intravenous (i.v.) cephalosporin (ceftminox, 1.0 g) once before surgery, and it was discontinued postoperatively. Pain after LC was assessed using the visual analog scale (VAS) from 0 (no pain) to 10 (worst pain imaginable) at 6, 12, and 24 hours after the operation. The analgesic requirement was estimated by measuring the total usage of parenteral analgesic (tramadol HCl, 50 mg) or oral opioid tablets (oxycodone HCl, 5 mg) during the postoperative hospitalization period. Analgesics were administered when the patient requested pain killers, and oral tablets were used after postoperative 24 hours if oral consumption was possible. To evaluate the residual volume of intraperitoneal gas, a plain chest X-ray was taken for all patients on the first postoperative day, and it was assessed using the formula described by Jackson et al. 8
Postoperative pyrexia was defined as a body temperature over 37.5°C sustained for >48 hours. Wound infection was defined as any complication of the trocar sites with tenderness or erythema requiring drainage, opening, or antibiotic therapy, whereas simple hematoma or seroma was not considered as wound infection. All parameters were evaluated by an independent investigator who was not related to the current study. The conditions for discharge were as follows: fine physical condition, ability to tolerate normal activities, and resumption of oral diet. All patients returned to the outpatient department on the seventh day after discharge, and wound status and general condition were checked.
Statistical analysis
Categorical variables were evaluated using the chi-square test or Fisher's exact test and continuous data were calculated using Student's t-test. Descriptive statistics were given as mean ± standard deviation. All tests are two-tailed and the level of statistical significance was set at .05. SPSS statistical package software (version 20.0 for Windows; SPSS, Inc., Chicago, IL) was used for data analysis. The primary outcome measure of this study was the extent of postcholecystectomy pain relief. The secondary outcome measures were the operation time, incidence of postoperative morbidity, and length of postoperative hospital stay. The calculation of the sample size was done such that it would be possible to distinguish a mean difference in pain score using the VAS of more than one point between the two groups. With a power of 80% and considering a dropout rate of 10%, a total of 48 patients (24 patients per group) were required to show the difference at a significance level of .05.
Results
Demographic findings and perioperative outcomes
A total of 54 patients were enrolled in this study, and they were randomly assigned to either the intervention group (group A) or the no-intervention group (group B). Among them, 3 patients who were found to have gallbladder malignancy in the permanent pathology report were excluded from the analysis. Finally, a total of 51 patients [26 patients (51.0%) in group A and 25 patients (49.0%) in group B] were analyzed; a diagram of patient enrollment is shown in Figure 1. The participants consisted of 19 males (37.3%) and 32 females (62.7%) with a mean age of 47.3 ± 13.5 years (24–76 years). Demographic characteristics are presented in Table 1. Both groups were comparable in terms of age, sex, and body mass index, and the most common diagnosis was chronic cholecystitis with cholelithiasis [20 cases (76.9%) in group A and 21 cases (84%) in group B] followed by gallbladder polyp [6 cases (23.1%) in group A and 4 cases (16%) in group B]. There was no statistical difference regarding disease diagnosis (P = .726) or type of operative procedure [three-port versus four-port, 25 (96.2%) versus 1 (3.8%) case in group A and 24 (96%) versus 1 (4%) case in group B, P = 1.000]. Perioperative outcomes and the details of postoperative morbidities are shown in Table 2. There was no statistical difference between the two groups in terms of mean operation time (25.6 ± 7.4 minutes in group A and 23.5 ± 7.1 minutes in group B, P = .296), mean estimated blood loss (17.5 ± 19.9 mL in group A and 17.9 ± 28.7 mL in group B, P = .137), or mean length of postoperative hospital stay (2.0 ± 0.2 days in group A and 2.5 ± 0.2 days in group B, P = .085). There was a significant difference in residual gas volume between the two groups (10.3 ± 30.5 mL in group A and 60.0 ± 42.2 minutes in group B, P = .000). In our study, a total of 5 morbidity cases (9.8%) were observed [2 cases (7.7%) in group A and 3 cases (12%) in group B, P = .668]. One patient in group A presented with wound infection at the umbilicus trocar site, which was treated with oral antibiotics and dressing. The other 4 cases were significant side effects associated with analgesic administration, such as nausea, vomiting, or urinary retention, as described in detail below.
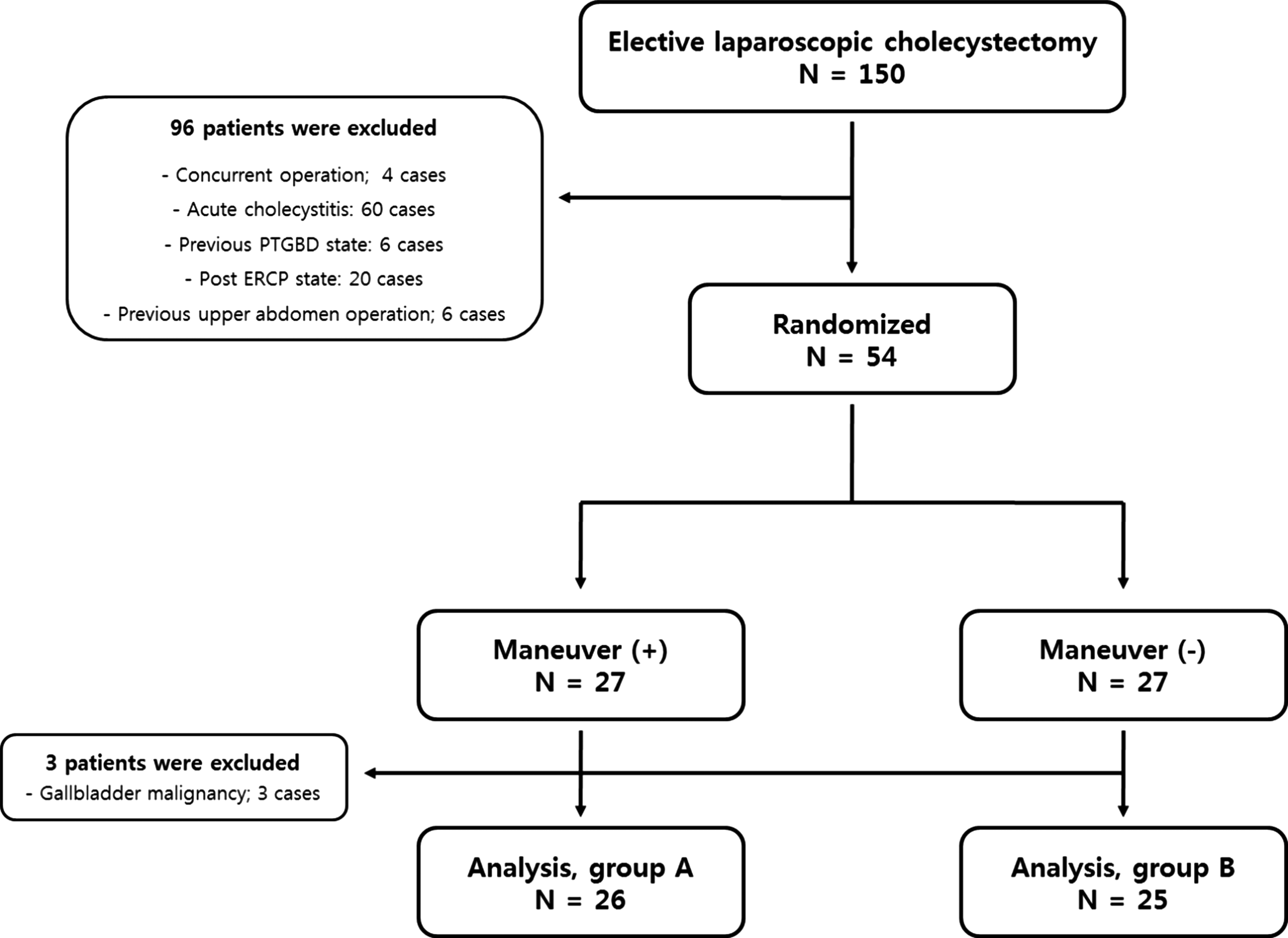
Flowchart for patient enrollment.
ASA, American Society of Anesthesiologist class; BMI, body mass index; GB, gallbladder.
P-value <.05.
LC, laparoscopic cholecystectomy.
Assessment of pain after LC
Pain assessment and total analgesic consumption are presented in Table 3. Total analgesic usage was compared between the two groups, and it is represented as total consumption of i.v. tramadol HCl and oxycodone tablets, the latter of which was converted to the equivalent dose of i.v. tramadol HCl using the equation described in a previous report (Kampe et al. 9 ; the equipotent dose ratio of i.v. tramadol HCl compared to oral oxycodone is 10:1). Analgesic consumption in group A was significantly lower in the form of both parenteral and oral agents. In group A, the total usage of i.v. tramadol HCl and oxycodone HCl tablets were 17.3 ± 31.4 and 3.1 ± 1.9 mg, respectively, whereas they were 48 ± 58.6 and 5.9 ± 3.7 mg in group B, respectively (P = .026, P = .002). VAS pain score was also significantly lower in group A at postoperative 6, 12, and 24 hours (3.7 ± 1.2 in group A and 4.8 ± 1.7 in group B at 6 hours postoperation, P = .016, 1.5 ± 0.6 in group A and 3.3 ± 1.3 in group B at 12 hours postoperation, P = .000, and 1.0 ± 0.6 in group A and 3.0 ± 1.7 in group B at 24 hours postoperation, P = .000). Among the postoperative morbidities, a total of 4 cases (7.8%) were reported that were associated with analgesic medications, 1 case in group A (3.9%, urinary retention) and 3 cases in group B (12%, 2 cases of nausea or vomiting and 1 case of urinary retention), and the difference between groups was not significant (P = .350).
P-value <.05.
i.v., intravenous.
Discussion
Postoperative pain is a subjective symptom; different individuals have a wide spectrum of responses to the same stimuli. Moreover, the pathogenesis of postoperative pain is multifactorial, which makes treatment more difficult and requires multifaceted methods for effective management. In elective LC, postoperative pain is the most common complaint that usually occurs within 48 hours after cholecystectomy. Several maneuvers have been reported to be effective in reducing pain after LC, which act through different mechanisms. First, insufflated CO2 gas during laparoscopic surgery converts to carbonic acid, which causes chemical irritation of the peritoneum leading to the referred pain in the shoulder.10,11 AGS 5 or pulmonary recruitment immediately after operation 6 effectively eliminates the remnant CO2 gas and reduces the pain after LC. Second, the insufflation of gas causes an overstretching and extension of the peritoneum and diaphragm. This may be associated with stretching of diaphragmatic muscle fibers and result in traumatic traction of the phrenic nerve, tearing of blood vessels, and the release of inflammatory cytokines that provoke the referred shoulder pain.2,10,11 Consequently, low-pressure pneumoperitoneum and slow insufflation of gas seem to be helpful in reducing pain after laparoscopic surgery. Lastly, the injection of a local anesthetic agent at the incisional wound site3,4 is also expected to paralyze the subcutaneous nerve and desensitize the patient to the parietal pain caused by trocar insertion or the distortion of incisional skin according to the manipulation of laparoscopic instruments.
Having gained an understanding of the multifactorial pathogenesis of pain after LC, we supposed that the performance of these procedures concurrently could be more effective in reducing pain from diverse routes such as visceral, referred, or somatic pathways. Indeed, the pain score using the VAS was significantly lower in the combined maneuver group at postoperative 6, 12, and 24 hours. However, it should be noted that there is a limitation to our study in that we compared performance of all procedures to none at all, not to each individual one, and, therefore, cannot confirm any synergistic effects. However, the results of this study using combined maneuvers revealed superior outcomes on pain control than did those of our previous report investigating the effects of AGS only (VAS pain scores were 3.7 ± 1.2 versus 4.1 ± 1.2 and 1.0 ± 0.6 versus 2.3 ± 1.4 at 6 and 24 hours postoperation, respectively). 5 Our results, therefore, support the notion that a synergistic effect on pain control can be expected through the intraoperative performance of various maneuvers concomitantly.
Herein, the dosage of opioid consumption between the two groups was also compared. Opioids usually act on the medullary center involved with vomiting and facilitate several complications, such as nausea, vomiting, urinary retention, or respiratory depression, and these adverse effects could be significant obstacles to fast recovery.12–14 In the current study, the consumption of opioid agents was significantly lower in the combined maneuver group. Additionally, all cases of complications, such as nausea, vomiting, or urinary retention, were observed in patients who had used opioid analgesics, although there was no significant difference between the two groups in terms of the incidence rate of those complications. We propose that the reduction in postoperative pain allows patients to avoid the unnecessary complications of opioid use, which hinder the quality of life or patient satisfaction. This might be of special importance in surgery for benign diseases. Additionally, we expect that the effective alleviation of pain through the combined maneuvers can also facilitate early ambulation, which helps patients recover faster. It could ultimately increase the validity of day care treatment for postoperative care after cholecystectomy. This can prevent the unnecessary expenditure of medical resources or insurance money.
In this study, the results concerning operation time and other parameters such as blood loss and the incidence of morbidities revealed no difference between the groups. We suppose this may be because the maneuvers we performed are very simple and noninvasive. Our findings show that the combined maneuvers can effectively reduce pain without causing an additional burden to the operator or patient, because our maneuvers require no specific instruments or entail any significant additional financial burden on the patient.
In conclusion, we first described the combined maneuvers composed of various methods, including local analgesic injection at the incision site, low-pressure pneumoperitoneum, AGS, and pulmonary recruitment during LC and their effectiveness in reducing postoperative pain. We propose that our combined maneuvers are effective and feasible methods for pain management after LC that also enables a reduction in opioid consumption and elevates quality of life after surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.