
Abstract
Abstract
Background:
Inguinal hernia is a common disease treated with diverse methods. Nowadays, laparoscopic totally extraperitoneal approach is gaining its validity and shows favorable outcomes. However, single-incision laparoscopic surgery is also widening its applicable fields as a new technique. This study aimed to find whether single-incision laparoscopic total extraperitoneal inguinal hernia repair (SILTEP) is applicable compared to conventional laparoscopic total extraperitoneal hernia repair (CLTEP).
Methods:
We retrospectively reviewed 120 cases of SILTEP and 60 cases of CLTEP in Yonsei University Severance Hospital from January 2012 to December 2013. Each group was compared with patients' characteristics, operative details, and postoperative complications.
Results:
There were no statistical difference in patient age, sex, body mass index, American Society of Anesthesiologists score, hernia type, or location between SILTEP and CLTEP. In operative details, operation time (61.77 ± 16.48 minutes versus 77.83 ± 35.15 minutes, P = .001) was shorter in SILTEP. Postoperative complication rate has shown no statistical difference in SILTEP compared to CLTEP (n = 20, 16.7% versus n = 16, 26.7%, P = .114).
Conclusions:
SILTEP is feasible and provides comparable postoperative outcomes compared to CLTEP. Although SILTEP has its own challenges for mastering the procedure, with some experiences, it is possible to operate as well as CLTEP.
Introduction
I
Currently, there have been efforts to reduce the usage of trocar for improving cosmesis. Thus, this led to evolution of a surgical technique known as single-incision laparoscopic surgery (SILS). Studies showing safety and effectiveness of SILS made extension of its field to cholecystectomy, appendectomy, and even to the colon resection.5–7 Not an exception to inguinal hernioplasty, as is called single-incision laparoscopic total extraperitoneal inguinal hernia repair (SILTEP) is being reported in several studies.8–11 However, there are few studies comparing conventional laparoscopic total extraperitoneal hernia repair (CLTEP) and SILTEP.12–14 Therefore, the aim of this study is to evaluate the safety and efficacy of SILTEP with compared to CLTEP.
Materials and Methods
Patients
Between January 2012 and December 2013, 120 inguinal hernia patients had undergone SILTEP and 60 inguinal hernia patients had undergone CLTEP. All patients had undergone physical examination in outpatient clinic for diagnosis, and an ultrasonogram was taken, if appropriate. Patient data were prospectively collected from Severence hospital, Yonsei University College of Medicine. Age, sex, body mass index (BMI), side of hernia, type of hernia, American Society of Anesthesiologists score, and previous lower abdominal surgery history were recorded in preoperative patients' characteristics. Primary or recurrent cases of inguinal hernia were all included in this series. Operation time, conversion status, intraoperative peritoneal injury, pain score, postoperative intravenous analgesic usage, postoperative hospital stay, and mortality were recorded in operative and postoperative details. Postoperative complications were categorized into hematoma, wound infection, seroma, urinary retention, chronic pain, scrotal swelling, recurrence, and others.
Single-incision laparoscopic TEP
All patients were given prophylactic antibiotics, and surgery was taken under general anesthesia, with supine position. A single 2.0 cm vertical incision was made through the umbilical skin with linea alba exposure after subcutaneous dissection. The linea alba was then incised vertically and the peritoneum was preserved. After careful finger dissection in extraperitoneal space, a disposable SILS Multiple Instrument Access Port (Covidien, Mansfield, MA) was placed through the umbilical incision, and three 5 mm channels were inserted into each hole of the SILS port. After 8 mmHg pressure of CO2 insufflation through the insufflation channel of the SILS port, an endoscopic camera 5 mm in diameter and 45 cm in length was accessed through the upper 5 mm channel. Graspers and monopolar diathermy were used to expose preperitoneal space through the two 5 mm channels. Lateral space was dissected toward the anterior superior iliac spine and continued medially until the inferior epigastric vessels, symphysis pubis, and cord structures were identified. If a direct hernia was present, the hernia sac was reduced using gentle traction on the sac and the defect of transversalis fascia was ligated with endoloop. In cases of indirect hernias, the hernia sac was carefully isolated, freed from the spermatic cord, and reduced from the internal ring by gentle traction and dissection.
Indirect hernia sacs were routinely ligated just beyond the internal ring with a Vicryl Endoloop (Ethicon, Somerville, NJ) and divided using endoshears. One 5 mm access channel was then removed and a 12 mm access channel was subsequently inserted. Polyester mesh (Parietex, Covidien, Dublin, Ireland) 10 cm × 12 cm in size was introduced through the 12 mm access channel, unfolded, and placed around the spermatic cord from the pubic symphysis to the anterior iliac spine laterally without fixation suturing. The space was deflated under direct visualization without drainage after completion of the operation. The incision wound was repaired with absorbable 3-0 sutures by subcuticular methods.
Conventional laparoscopic TEP
All patients were given prophylactic antibiotics, and surgery was taken under general anesthesia, with supine position. About 1 cm semicircular incision was made through the infraumbilical skin and the preperitoneal space approached after opening fascia. With a midline incision, a small space is made, and then a camera itself was used to widen preperitoneal space, bluntly. After 8 mmHg pressure of CO2 insufflation through the insufflation channel of infraumbilical port, by direct vision of endoscopic camera, the first 5 mm trocar is placed in the suprapubic level and the second 5 mm trocar is placed between umbilicus trocar and suprapubic trocar. When hernia is on both sides, the second 5 mm trocar is inserted strictly on midline, but when hernia is on only one side, the second 5 mm trocar is inserted slightly opposite side of hernia from midline to approach easily by securing space. Then graspers and monopolar diathermy were used to expose the preperitoneal space. The lateral space was dissected toward the anterior superior iliac spine and continued medially until the inferior epigastric vessels, symphysis pubis, and cord structures were identified. If a direct hernia was present, the hernia sac was reduced using gentle traction on the sac. In cases of indirect hernias, the hernia sac was carefully isolated, freed from the spermatic cord, and reduced from the internal ring by gentle traction and dissection. Indirect hernia sacs were routinely ligated just beyond the internal ring with a Vicryl Endoloop (Ethicon, Somerville, NJ) and divided using endoshears. Polyester mesh (Parietex, Covidien, Dublin, Ireland) 10 cm × 12 cm in size was introduced through the 10 mm access channel, unfolded, and placed around the spermatic cord from the pubic symphysis to the anterior iliac spine laterally without fixation suturing. The space was deflated under direct visualization without drainage after completion of the operation.
Statistical analysis
All variables are described using mean ± standard deviation or percentages, properly. Only age was described with median and range. Chi-square test or t-test was used to compare variables between two surgical groups. All data were analyzed with Statistical Package for the Social Sciences Windows version 20.0 (SPSS 20.0 for Windows; SPSS, Inc., Chicago, IL), and statistical significance was accepted at P value <.05.
Results
Table 1 shows preoperative patients' characteristics of SILTEP and CLTEP. There was no statistical difference between two groups.
ASA, American Society of Anesthesiologists; BMI, body mass index; CLTEP, conventional laparoscopic totally extraperitoneal; SD, standard deviation; SILTEP, single-incision laparoscopic totally extraperitoneal.
Operative and postoperative details are shown in Table 2. Operation time was shorter in the SILTEP group than the CLTEP group (P = .001). However, when subdivided by unilateral and bilateral group, only unilateral operative time was shown shorter compared to CLTEP (P = .003). Pain score, postoperative IV analgesics use, surgery conversion, and peritoneal injury have shown no statistical difference. There were two cases of peritoneal injury during the operation in SILTEP and four cases in CLTEP. There was one conversion case each from SILTEP and CLTEP group to open surgery. One case in SILTEP was converted because of severe adhesion. The other case in CLTEP was converted because of peritoneal injury, incomplete reduction, and high BMI (34.6 kg/m2), which made surgery complicated.
Values shown in bold are <.005, and are significant.
CLTEP, conventional laparoscopic totally extraperitoneal; IV, intravenous; NPIS, numeric pain intensity scale; OP, operation; POD, postoperative day; SILTEP, single-incision laparoscopic totally extraperitoneal.
Table 3 shows postoperative complications in two groups. There were no significant statistical differences between the SILTEP and CLTEP group (P = .114).
CLTEP, conventional laparoscopic totally extraperitoneal; SILTEP, single-incision laparoscopic totally extraperitoneal.
There were two recur cases in the SILTEP group and one recur case in the CLTEP group. Two cases in the SILTEP group were recurred hernia cases when initially treated with SILTEP. All patients underwent reoperation with open hernioplasty. Every recurred patient who has undergone open hernioplasty is being followed up in outpatient clinic without any complication. Figure 1 shows single incision only 2 cm long, enough to be buried in to dented umbilicus. This picture was taken from outpatient clinic after 7 days of discharge from hospital after SILTEP.

Picture of SILTEP postoperative wound after seventh day of operation. SILTEP, single-incision laparoscopic totally extraperitoneal.
Figure 2 shows SILTEP operation, approaching working port parallel to hernia site. Figure 3 shows initial three of 5 mm trocar inserted in SILS port, and Figure 4 shows changing one 5 mm trocar to 12 mm trocar for insertion of Vicryl Endoloop (Ethicon, Somerville, NJ) and Polyester mesh (Parietex, Covidien, Dublin, Ireland). Figure 5 shows anatomy of operation field by direct vision under laparoscope, and Figure 6 shows fully covering hernia site with mesh after hernia sac ligation.

Picture of SILTEP operation, approaching parallel to hernia site. SILTEP, single-incision laparoscopic totally extraperitoneal.

Initial 5 mm trocar approach to inguinal area.

After changing 5 mm trocar to 12 mm trocar.
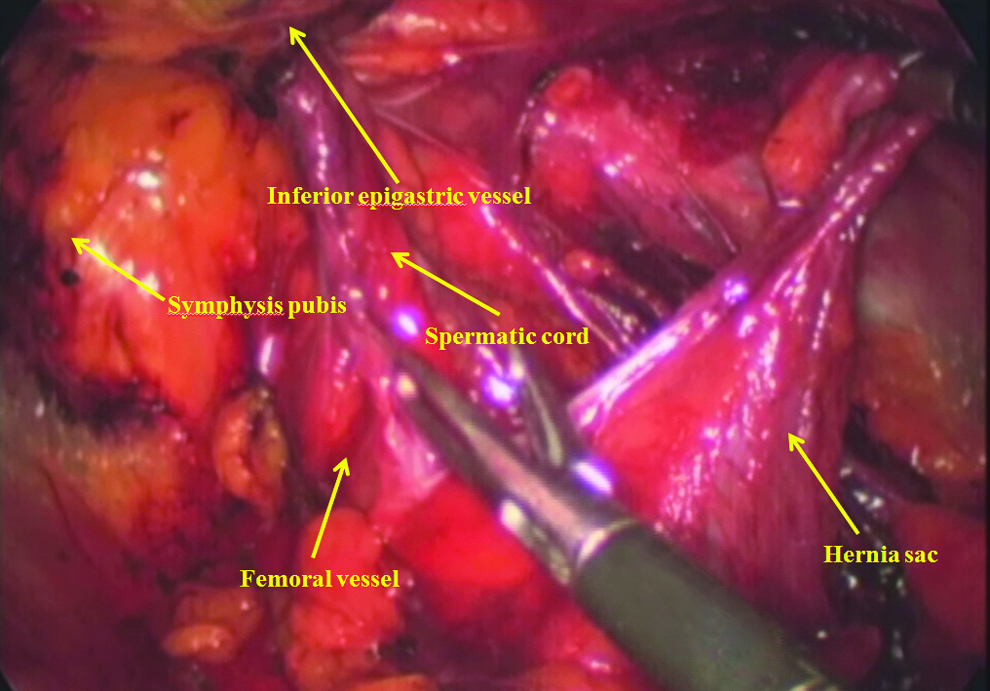
Operative field by SILTEP. SILTEP, single-incision laparoscopic totally extraperitoneal.
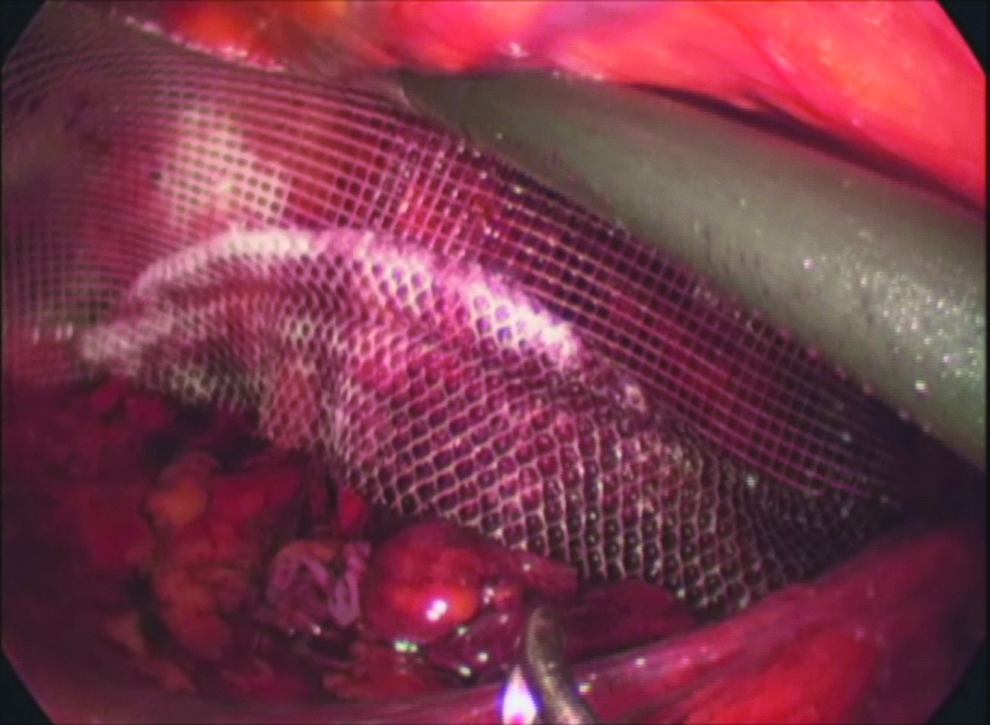
Mesh applied after hernia sac ligation.
Discussion
This study showed that SILTEP could be a feasible procedure compared to CLTEP in inguinal hernia repair. Commonly, SILS operation is considered to be difficult, but SILTEP seems applicable as TEP operation in inguinal hernia requires limited surgical field than other SILS operation and needs simple dissection.
As mentioned above, since the first report of SILTEP hernia repair by Filipovic-Cugura et al., 15 there have been few reports comparing SILTEP between CLTEP. SILTEP has its own challenges, including the relative loss of triangulation, inline vision, clashing of instruments, and a steep learning curve for mastering the procedure. Contrary to expectations, SILTEP showed shorter mean operative time compared to CLTEP in our study. First, when performing TEP operation, it is a critical issue to make secure preperitoneal space. CLTEP makes preperitoneal space bluntly, which might not form fully enough space, while SILTEP makes this space clearly under direct vision. Without proper formation of preperitoneal space, there are risks of peritoneal perforation, bleeding, exposing surgical field below the inferior epigastric vessel, which make surgery difficult. Second, when using working port, the SILTEP approach to hernia site from umbilicus is in a parallel way, while the CLTEP approach is vertical from skin. In CLTEP, the first suprapubic 5 mm trocar reaches hernia vertically and second midline 5 mm trocar reaches hernia diagonally, which may increase possibilities of peritoneal perforation, if surgeon fails to control handling power during dissecting tissues. However, in SILTEP, after approaching preperitoneal space, tissue dissection is processed up and down or lateral, which is not perpendicular to the direction of working port. This difference may result in less peritoneal perforation near the inguinal field in SILTEP. Elimination of extra 5 mm trocar placement and shorter closing time in SILTEP, as it has only single incision, also may account for competitive operative times in this study. Mainly, time differences occurred in unilateral hernia operation rather than bilateral hernia operation and this shows a similar result from Buckley et al. 13 Nevertheless, bilateral hernia operation is less time-consuming in SILTEP than CLTEP, although it was not statistically significant.
SILTEP had comparable postoperative pain on operation day and postoperative day 1 to CLTEP. Patients' request for intravenous analgesics after operation was checked for supportive evidence to find out the severity of postoperative pain, which turned out to have no statistical difference between SILTEP and CLTEP. Complications between the two groups also demonstrated to have no statistical difference between SILTEP and CLTEP.
In our study, we did not measure the satisfaction level of postoperative scar between two groups. Although the cosmetic satisfaction is a subjective issue, some reports reveal higher satisfaction in SILTEP.14,16 Nevertheless, it is for sure that as SILTEP uses less number of ports, it results in less number of scars.
As this is a retrospective study with single institution experience, prospective randomized trial with long-term follow-up is needed to provide more definitive statement of the efficacy of this procedure. SILTEP is safe and feasible, and provides comparable postoperative outcomes compared to CLTEP. Although SILTEP has its own challenges for mastering the procedure, with some experiences, it is possible to operate as well as CLTEP.
Footnotes
Disclosure Statement
No competing financial interests exist.