
Abstract
Abstract
Hirschsprung disease is a congenital disease characterized by intestinal aganglionosis of various extents. Most patients are younger than 1 year of age. Though, a minority of cases can be older or even adult. Older the patient the more difficult and prolonged is the endorectal dissection required for the pull-through procedure. Longer surgery leads to longer anal dilatation and trauma with subsequent higher likelihood of continence impairment. The article aims at describing the first case series of robot-assisted Soave procedure, which was adopted as an alternative minimally invasive approach to older patients with Hirschsprung disease. The technical principles are represented by intraoperative seromuscolar leveling biopsies, intracorporeal endorectal cranial dissection, and endorectal pull-through with colo-anal anastomosis. The authors report three procedures that were carried on without complication with a limited requirement for anal dilatation and trauma, given the reduced need for endorectal caudal dissection. The results demonstrate the feasibility of the proposed approach. The robotic approach should be considered as an alternative minimally invasive approach for older children or adults with Hirschsprung disease.
Introduction
H
The introduction of minimally invasive surgery in children has progressively gained popularity also for the treatment of HSCR. Georgeson et al. in 1995 first described the laparoscopic ERPT. 6 Many other laparoscopic procedures and modifications of Soave technique were reported later on. A sole transanal ERPT (TERPT) without laparoscopic or laparotomic assistance was also introduced by De la Torre in 1998. 7 At present, there is no evidence on the superiority of one of these techniques over the others as reported in a recent meta-analysis by Thomson et al. 8
Recently, robotic surgery (RS) was introduced in the pediatric clinical practice. 9 RS is largely used in adult surgery and thanks to the relatively easier management of deep endopelvic structures, found its ideal indications in prostatic and colorectal surgery.
All minimally invasive procedures (either laparoscopic or not) include an extended transanal endorectal dissection that can turn traumatic for the sphincteric structure, given the need for prolonged and tough anal dilatation. Obviously, older the patient the more extended, difficult, and prolonged is transanal endorectal dissection required to get to the peritoneal reflection to complete the ERPT. Subsequently, older the patient higher the likelihood of damaging sphincteric structures.
Some adult surgeons dealing with HSCR proposed the use of a laparotomic or modified laparoscopic Duhamel procedure (posterior dissection of aganglionic rectum) to deal with adult aganglionosis.10,11 To reduce the duration and extent of sphincters stretching and trauma during transanal dissection in older children or adults with HSCR, we decided to apply a robot-assisted endorectal dissection resorting to the very first principles of dissection reported by Franco Soave in 1964. To the best of our knowledge this is the first description of a robotic Soave ERPT in literature.
Robotic Technique According to Soave's Principles
The patient is prepped from the nipple to the knees with complete sterilization of buttocks and perineum to have complete access of all surgical fields. Pneumoperitoneum is created with Veress needle and CO2 is inflated with a pressure up to 12 mmHg. A 12-mm trocar is inserted in the umbilicus. Two 8-mm trocars are inserted in the right iliac fossa and in the left flank. Robotic arms are inserted in these three trocars and a further 5-mm trocar is inserted in the left or right hypochondria to assist traction and manipulation with conventional laparoscopic instruments. The DaVinci® Surgical System Robotic IS3000 HD single console with four arms (Intuitive Surgical, Inc., Sunnyvale, CA) was used in this case series. Figure 1 shows team layout and docking in case of a robotic Soave procedure.
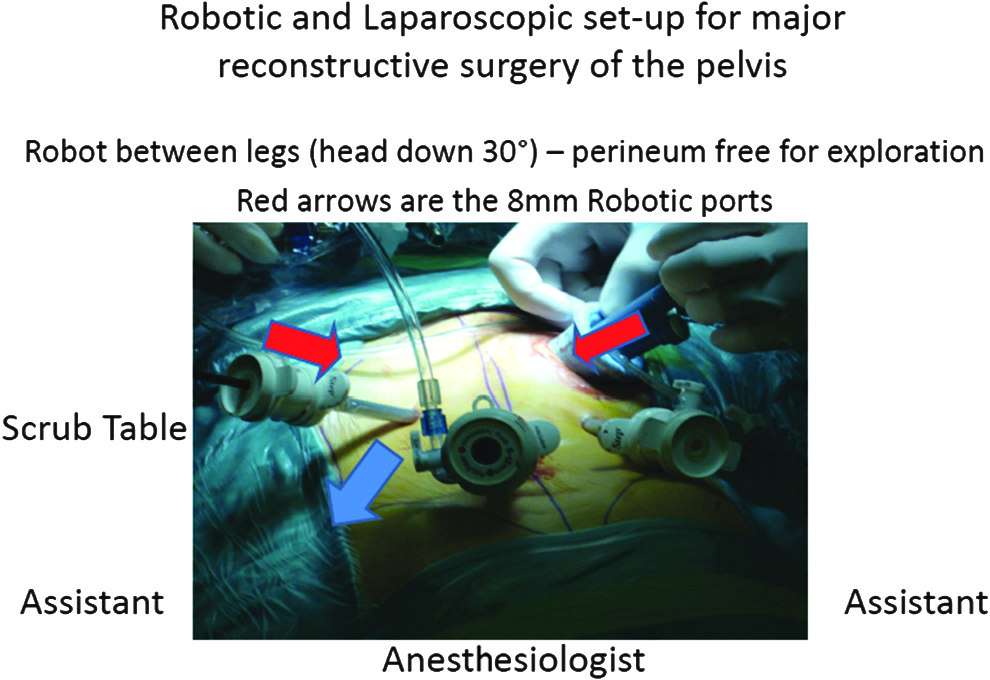
Team layout and docking for major pelvic reconstructive surgery. This picture shows a typical setting in pelvic laparoscopic surgery. The red arrows indicate the sites for 8 mm robotic ports positioning. The anesthesiologist is placed at the head of the patient. The two assistant pediatric surgeons stand on both sides and the scrub nurse is on the left hand side of the operating table. If the patient has a stoma, a SILS® port (Covidien plc, Cherrywood Business Park, Dublin, Ireland) can be used to avoid multiple trocars and facilitate manipulation and mobilization.
A complete visualization of the distal colon is required to identify the transition zone and the dilated colon predicted site of normoganglionosis. A seromuscular biopsy is performed just proximal to the dilated colon in the area of suspected normoganglionosis to confirm the normal innervation of the bowel that will be pulled-through and anastomized to the pectinate line. Mesorectal and mesosigmoid dissection is performed with robotic bipolar scissors down to the peritoneal reflection after visualization of ureters, vas, and seminal vesicles (in males).
A seromuscolar dissection is started 0.5 mm above the peritoneal reflection according to Soave original report. 5 The dissection is carried down as far as possible until 2–3 cm of remaining dissection is required (Fig. 2). The extend of dissection is determined by inserting a probe in the rectum and checking the downward progression of the seromuscular dissection (see Supplementary Video 1; Supplementary Data are available online at www.liebertpub.com/lap). The patient is then moved to a gynecological position with slight Trendelemburg tilting of the operative table. A limited transanal endorectal dissection is then started 1–2 mm above the pectinate line and extended upward to join the distal part the robotic dissection. The previously isolated distal colon is then pulled-through until the seromuscular biopsy is identified and a colo-anal anastomosis is accomplished at the pectinate line. All patients undergo examination under anesthesia (EUA) 6 week postoperatively to check anastomosis and possibly dilate strictures.
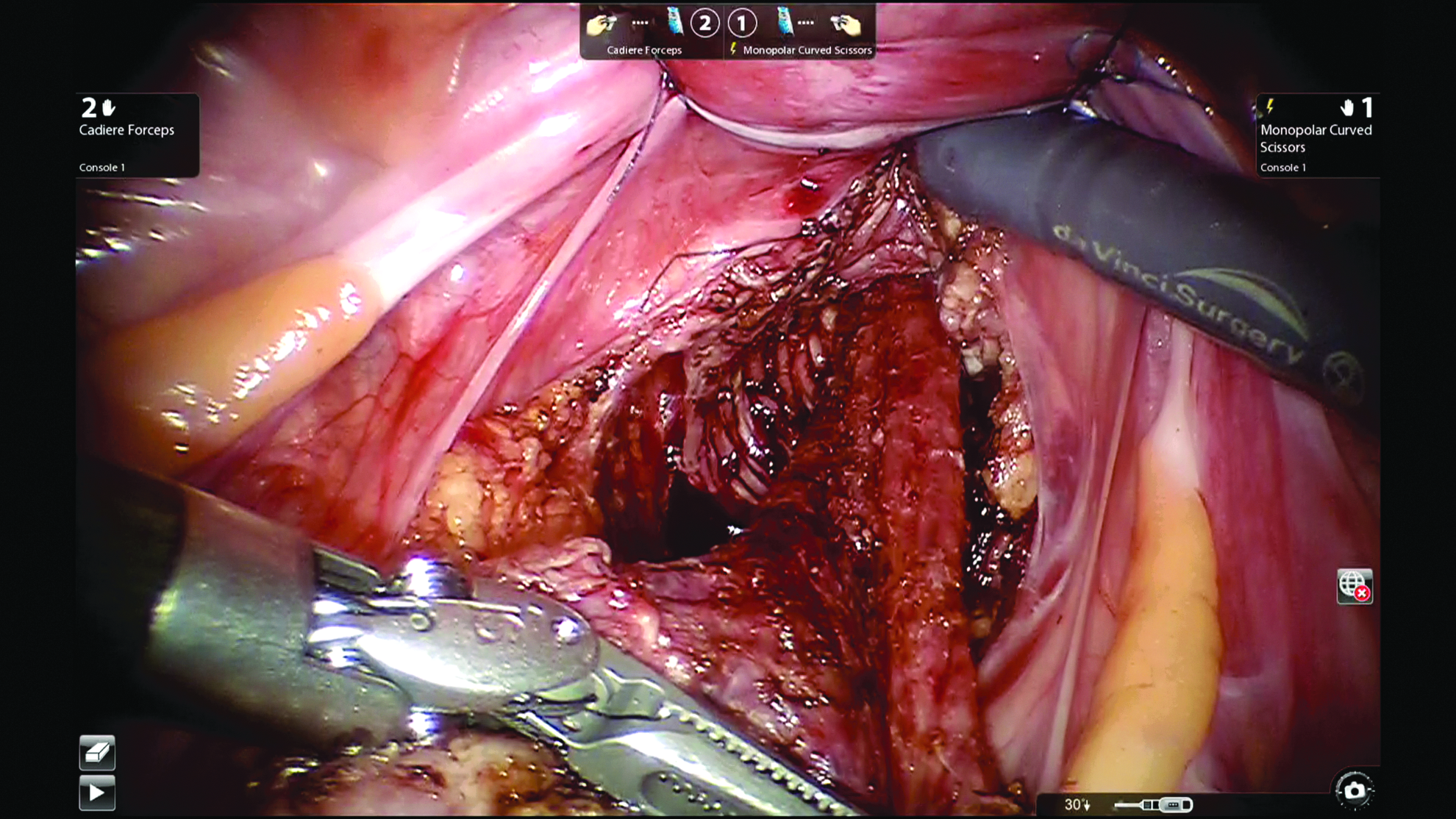
Seromuscolar dissection in the submucosal plane carried down to 2–3 cm from the pectinate line.
Case Series
1. A 5-year-old boy, pluri-operated for a rectosigmoid form of HSCR presented to our department with a diverting ileostomy. Patient's weight was 40 kgs. The procedure consisted of stoma closure, intraoperative leveling biopsies, and robotic Soave procedure as described above. A multichannel-access flexible SILS® Port (Covidien plc, Cherrywood Business Park, Dublin, Ireland) was inserted in the site of stoma closure site and used for two 5 mm servicing instruments (needle insertion and suction/irrigation). No intraoperative complications occurred. Robotic console time was 120 minutes. Overall surgery lasted 445 minutes. The patient was discharged in postoperative day 7. EUA was uneventful without strictures or anastomotic issues. Continence was normal at 6 months follow-up without episodes of soiling, excellent sensation, and possibility to hold up bowel movements without leakage. No constipation was experienced. No episodes of enterocolitis occurred postoperatively.
2. A 16-year-old boy had a delayed diagnosis of rectal HSCR and underwent radical treatment of his longstanding symptoms. Patient's weight was 65 kgs. The procedure consisted of intraoperative leveling biopsies and robotic Soave procedure as described above. No intraoperative complications occurred. Robotic console time was 230 minutes. Overall surgery lasted 525 minutes. The patient was discharged in postoperative day 6. EUA demonstrated anastomotic stricture that underwent two cycles of dilatation under anesthesia. Continence was normal at 3 months follow-up without episodes of soiling, excellent sensation, and possibility to hold up bowel movements without leakage. No constipation was experienced. No episodes of enterocolitis occurred postoperatively.
3. A 20-month-old female infant had a delayed diagnosis of rectal HSCR and underwent radical treatment of her longstanding symptoms. Patient's weight was 13 kgs. The procedure consisted of intraoperative leveling biopsies and robotic Soave procedure as described above. No intraoperative complications occurred. Robotic console time was 115 minutes. Overall surgery lasted 230 minutes. The patient was discharged on postoperative day 5. EUA was uneventful without strictures or anastomotic issues. Continence could not be assessed at 3 months follow-up due to age lower than 4. No constipation was experienced. No episodes of enterocolitis occurred postoperatively.
Postoperative course was uneventful with routine administration of an elastomeric pump (chirocaine plus clonidine) but no requirements for opioids administration in any of the patient. Faces, legs, activity, cry, and consolability score were well within the limits of optimal pain control for the entire length of hospital stay. Postoperative histochemestry, immunohistochemistry, and histology of the proximal resection margin confirmed normal innervation pattern in the whole circumference of the resected bowel thus confirming the adequate level of anastomosis.
Discussion
Surgery represents the only radical treatment for HSCR. Although available surgical procedures proved to be relatively safe and effective, several complications have been described intraoperatively, postoperatively, and in the long term. Possible intraoperative or short-term surgical complications include infections, bleeding, adhesions, anastomotic strictures, cuff abscess and fistula, and cuff strictures. Long-term sequelae are mostly related to residual disease (residual aganglionosis or hypoganglionosis), enterocolitis occurrences, and continence issues (either constipation, soiling, or complete incontinence). Given the sphincteric trauma related to the dissection required to radically treat intestinal aganglionosis a number of patients can experience troublesome issues in the long term. Recently, Neuvonen et al. reported that continence issues are complained by up to 25% of patients in the very long term and in adulthood after a TERPT performed in early childhood. 12 Of note, the same author reported in another article up to 58% of soiling (either frequent or occasional) after a TERPT. 13 The authors concluded that continence issues are the most important complaints in the long term that will ultimately interfere with the quality of life of our patients. Among the causes of impaired continence and bowel function in patients who underwent a TERPT we must include prolonged sphincter stretching and deep surgical dissection. In case of infections, the likelihood of functional issues will raise.
RS was mostly introduced to overcome some limitations represented by limited operative space and poor visualization of the deep pelvis and the limited degree of freedom of conventional laparoscopy. With specific regard to HSCR, the major strength of RS is the possibility to perform an extended seromuscular dissection thanks to a better 3D visualization of robotic camera and to the degrees of freedom of robotic instruments that allows an ideal identification and dissection of submucosa. These advantages are well evident if we compare RS either with laparoscopic surgery or with conventional open laparotomic surgery in a limited working space such as that of the deep pelvis. An extensive intra-abdominal seromuscular dissection affects the need for a far less extensive transanal dissection and may potentially reduce the risk for complications related to the perineal surgical step. Reduced sphincters stretching and endorectal dissection are required compared to conventional laparoscopic surgery. Easier seromuscular dissection is performed down to 2–3 cm above the pectinate line compared to conventional laparotomic surgery.
This aspect becomes crucial in adults or older children as this subset of patients with HSCR requires the longest and most difficult endorectal transanal dissection. Those patients have a higher likelihood of developing continence issues in the long term unless a short rectal aganglionosis is left in place with subsequent symptoms recurrence or persistence. In case of radical treatment, older patients will experience the highest risk of continence issues after a TERPT either laparoscopic assisted or not. This issue is confirmed by a number of authors proposing posterior dissection (i.e., Duhamel approach) for the treatment of HSCR in adults. Nonetheless, Rintala and Pakarinen 14 in a wide literature review reported a measure of continence impairment ranging between 35% and 55% in adults who underwent a Duhamel procedure in infancy thus suggesting that this procedure cannot be considered safer or more effective than ERPT either in children or adults.
Even though recently Rickey et al. reported a robot-assisted Soave procedure in a young adult, 15 the authors did not describe a true Soave procedure but a robot-assisted Georgeson procedure without seromuscular intracorporeal dissection, as originally reported by Franco Soave in 1964. Our proposed robotic Soave has never been reported so far. It proved to be feasible and safe in older patients with Hirschsprung disease. Although based on a small case series and a relatively short follow-up, our encouraging results suggest that RS may play a role in the treatment of older patients with HSCR. Nonetheless, we believe that robotic Soave procedure is feasible only in highly specialized referring centers dealing with HSCR with advanced laparoscopic skills.
Further studies on long-term functional outcome are required to confirm effectiveness, safety, and reproducibility of this robotic approach and possibly determine its superiority over conventional laparoscopic procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.