
Abstract
Abstract
Objective:
To determine the association between pain related to laparoscopic port sites and different incision sizes after gynecological laparoscopy.
Design:
Prospective, cohort trial Canadian Task Force classification 2-II.
Setting:
Zhejiang Provincial People's Hospital, China.
Patients:
Two hundred patients who underwent three-port laparoscopic gynecological procedures for benign indications.
Interventions:
In total, 200 patients underwent laparoscopic gynecological procedures. Each patient had three incisions, one in the left lower abdomen, measuring 5, 10, or 15 mm based on the type of surgery, another measuring 10 mm in the umbilical port, and the third one measuring 5 mm, in the right lower abdomen. Port-related pain was registered and measured by visual analogue score (VAS).
Measurements and Main Results:
The VAS score showed statistically significant differences between 5-, 10-, and 15-mm port sites at each time point (24 and 72 hours) (P < .05); the score elevated as the size of the incision increased. Pain was significantly lower at the umbilical port sites at 24 hours than in the left lower abdominal port sites with incisions of the same (10 mm) size (P = .013) and also significantly lower in the right lower abdominal port sites than in the left lower abdominal port sites with incisions of the same (5 mm) size (P = .041). Specimen extraction port significantly affected the 24-hour pain intensity, while specimen extraction port, surgical time, and previous abdominal surgery affected the 72-hour pain intensity.
Conclusions:
The size of port sites is the most important factor related to port-specific pain.
Introduction
P
Bisgaard et al.2,3 reported that about 60% of patients complained of moderate to severe pain during the first 24 hours after laparoscopy, but a surprising finding was that the pain remained high in many patients throughout the first postoperative week. Despite the advantages of the minimally invasive nature of this procedure, the postoperative pain meant a slower return to routine activities, increased use of analgesics, prolonged length of hospital stay, and, consequently, increased total healthcare costs.2,3 It has been reported that incisional pain is more intense than visceral pain after laparoscopy procedures and is the principal patient complaint during the first 48 hours after surgery.1–3
Recently, surgeons have attempted to reduce postoperative pain by reducing the number and size of incisions. There has been a recent drive to reduce port number and sizes, first with the introduction of a 5-mm laparoscope and then with an equipment designed for 3- and 2-mm port sizes4,5 or single-port laparoscopy (SPL).6–10 The rationale is that using smaller and/or fewer surgical ports constitutes a less invasive technique that would cause less trauma and, consequently, lead to better surgical outcomes.11,12
There exist multiple studies about interventions to relieve port-specific pain after laparoscopic procedures, but most of them reported that smaller or fewer ports did not necessarily cause less pain.13–20 In addition, the safety of miniport laparoscopy has been questioned. 21 Some studies reported lack of evidence about this technique in terms of patient mortality, morbidity, length of hospital stay, return to work, or requirement of cosmetic improvements compared with standard port laparoscopy.13,14 Present studies do not allow surgeons to recommend miniport laparoscopy routinely yet, and, in fact, there exists a modest increase in the operating time using this method. 21 As previously mentioned, identifying the fundamental factor that affects port-specific pain is critical to alleviate the pain.
However, a quantitative pain analysis related to laparoscopic port size and location is not available in the literature. There are some data on port site pain,4,22–23 but the reported results fail to correlate with the pain measure at different times, sizes, or locations.
Therefore, the present study was designed to prospectively assess the pain related to each port site with different sizes, distribution, and times. Surgical facts (e.g., abdominal wall closure suture, extraction technique, use of surgical tapes, emergency or elective type, surgical time) and baseline characteristics (e.g., patient age, education background, body mass index [BMI], previous abdominal surgery) were also assessed, to determine the factors that could influence the pain score and to provide a theoretical basis to understand the pathophysiology of port-specific pain.
Materials and Methods
This was a prospective cohort trial that included patients who underwent gynecological laparoscopic procedures with three laparoscopic ports, with one in the left lower abdomen, another in the umbilical port, and the third in the right lower abdomen. The Ethics Committee of Zhejiang Provincial People's Hospital approved the study protocol (2014KY060). The sample size was calculated in 200 patients, expecting to reach 600 laparoscopic ports. All patients classified under American Society of Anesthesiologists (ASA) grade I–II, who were scheduled for gynecological laparoscopic surgery, were enrolled in this trial after providing written informed consent.
Patients aged younger than 18 years or those older than 80 years, those with language limitations, those who converted to open surgery, those requiring drainage tube placement, those suspected of having a malignant disease, those who opted for analgesia pump after operation or local anesthesia during the operation period, and those with a pre-existing pain-related or pain-affecting morbidity such as a medical history of chronic pain, those who reported pain medication, alcohol or drug abuse, patients undergoing psychiatric treatment, and those with diabetes were excluded from the study. Patients who underwent pure SPL and patients in whom laparoscopy involved another port number and distribution or an incision size other than 5, 10, or 15 mm were also excluded from the study.
Postoperative pain at each port insertion site was evaluated using a visual analogue score (VAS), owing to its high validity and reproducibility, as well as its ratio scale properties. 24 Before surgery, all patients were explained how to score pain on the VAS (0 mm, no pain; 100 mm, maximal pain), 24 and they were clearly told that they would not be given analgesics during the postoperative period unless they requested for them. The scores were measured as the main objective. Secondary objectives included some surgical facts (e.g., type of abdominal closure suture, extraction technique, use of surgical tapes, emergency or elective surgery, surgical time) and baseline characteristics (e.g., patient age, education background, BMI, previous abdominal surgery).
All patients underwent a standardized general anesthetic induction and maintenance without epidural anesthesia. A single intravenous dose of antibiotics was administered before surgery. The operative field and port sites were dressed with identical dressings regardless of the procedure. All operations were performed by the same experienced laparoscopic surgical team (all right-handed surgeons). All surgeries were performed using three trocars, with the patient in the Trendelenburg and modified lithotomy position, with arms secured at the sides and the surgeon positioned to the left of the patient.
First, a vertical 10-mm incision was made in the center of the umbilicus and a 10-mm trocar was introduced; CO2 gas was insufflated at 3 L/min to establish pneumoperitoneum with an intraperitoneal pressure of 12–15 mmHg with continuous CO2 insufflation. A 30-degree, 10-mm telescope (Karl Storz, Tuttlingen, Germany) was inserted through the umbilical port. Another trocar placed in the left lower abdomen at reverse McBurney point was the closest to the surgeon among the three trocars and had three different incision sizes (5, 10, and 15 mm) according to the type of surgery.
For example, myomectomy and subtotal hysterectomy, which need electric power morcellation, required a 15-mm incision at the left lower abdominal port. In total hysterectomy, in which the specimen (uterus) was taken out through the vaginal stump, the size of the left lower abdominal port was either 10 mm or 5 mm, depending on the preference of the operating surgeon. Oophorocystectomy, adnexectomy, salpingectomy, salpingotomy, and other types of operations required either 10- or 5-mm ports depending on the port used for specimen extraction, with 10 mm reserved for this purpose. The third trocar measuring 5 mm was placed in the right lower abdomen in the midclavicular line under direct vision (Fig. 1). All trocars were blunt-tip type and were placed under direct vision. The same surgical team performed every intervention.
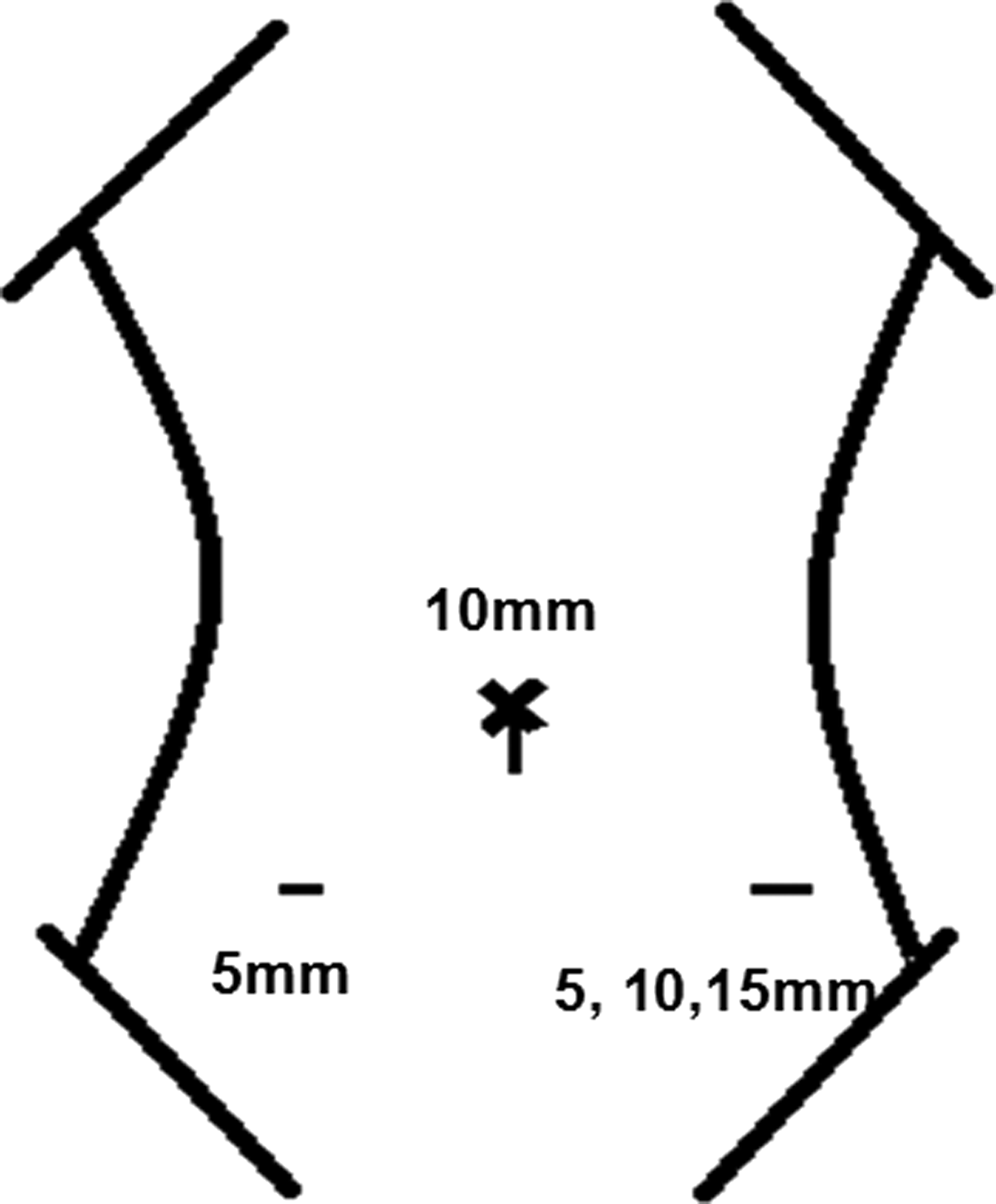
Schematic diagram of the laparoscopic ports used. Only the left port has different sizes.
The assistant only controlled the 30-degree laparoscope. The surgeon tailored the incision size according to the size of the trocar to be used. The freed surgical specimen was removed from the abdominal cavity through the umbilicus or the left abdominal trocar either with or without the use of a specimen bag. When used, a retrieval bag was inserted blindly through the umbilical trocar or through the left abdominal trocar under direct vision. The specimen was placed in the retrieval bag and removed by pulling the edge of the bag through the trocar. If the incision is further extended for extraction, a larger trocar would be required. The abdominal cavity was cleaned with 1000 mL of saline at the end of the procedure. No local or regional anesthesia was applied to the wound before or after operation and no drainage tubes were placed.
After the completion of laparoscopic surgery, 1-0 polyglactin 910 suture (Ethicon, Somerville, NJ) was used to close the fascial defect if the port site was 10 mm or greater. The skin was closed using either 4-0 polyglactin 910 sutures (Ethicon) or 1-0 polyglactin 910 sutures using the same technique, and the same surgical tapes were applied.
Patients were encouraged to resume activity as soon as possible after surgery. If patients asked for painkillers within 12 hours after operation (propyphenazone tablet or Dolantin with a half-time of about 3 hours), the effect of analgesia was eliminated at the time of assessment (24 hours after surgery), taking care not to affect the evaluation. Pain was assessed at rest. A resident who did not participate in the surgery (blinded observer) asked the patients to report the pain at each port through the VAS score based on the standardized questionnaire. A nontransparent sterile dressing was applied postoperatively over the skin wounds to prevent the patients from looking at their incision size. Because patient self-reporting is the most reliable indicator of pain, to avoid the introduction of induced pain, pain was measured without dressing changes within 24 hours after surgery.
After the assessment, some patients had surgical tapes applied, while some preferred keeping the wound open and denied dressing. Then, the investigators, together with the operating surgeon, filled out a detailed standardized data sheet. The size, type, and the precise port distribution were recorded, together with the patients' baseline characteristics, surgery type and surgical time, and method of wound closure. At 72 hours after the operation, the VAS scores were obtained by the observer and recorded in the data sheet. All patients underwent pain evaluation at 24 and 72 hours after the operation.
Statistical analysis
Statistical analysis was accomplished using χ2 analysis for proportional data. For continuous variables, the treatments were compared using t tests. Pain intensity scores (VAS scores) from 0 to 100 mm were considered as continuous variables. Data are expressed as mean ± standard deviation. P < .05 was considered statistically significant. Data were analyzed using SPSS version 19.0 for Windows.
As every patient had a 10-mm umbilical incision and 5-mm right lower abdominal incision, to assess the relationship between the incision size and the pain intensity, the left lower abdominal incision was the key point to evaluate and compare. Besides port incision and distribution, the relationships between other factors, including port-specific/baseline characteristics and pain intensity, were also assessed using analysis of variance. Any factors with P < .1 in univariate analysis will be included in a multivariate analysis to assess the relationship between port size and pain intensity using analysis of covariance.
Results
From October 2014 to June 2015, data from 259 continuous patients were collected, among which 57 patients were excluded according to the exclusion criteria; another 2 patients who asked for painkillers within 12 hours close to the assessment time were also excluded from the study. Finally, 200 patients completed this study and were considered eligible for analysis; 159 (79.5%) of these were electively operated and 41 (20.5%) underwent an emergency procedure. Each patient had 3 incisions; one in the left lower abdomen (5, 10, or 15 mm based on the type of surgery), another in the umbilical port (10 mm), and the third in the right lower abdomen (5 mm). Altogether, there were 600 port sites in the 200 patients.
As the present trial was an observational study of all kinds of benign laparoscopic gynecological procedures, we could not select the type of operations; hence, the numbers of patients with 3 different left port sizes were not consistent. With regard to the left lower abdominal port, 41 patients (20.5%) had 5-mm port sites, 82 patients (41%) had 10-mm port sites, and 77 (38.5%) patients had 15-mm port sites. In total, 35 myomectomies, 33 subtotal hysterectomies, 18 total hysterectomies, 44 oophorocystectomies, 19 adnexectomies, 29 salpingectomies, 12 salpingotomies, and 10 other types of procedures were performed. Despite the slight difference in the duration of surgery, all procedures were benign laparoscopic procedures and were similar in complexity. Table 1 shows the surgical characteristics of the performed procedures.
BMI, body mass index.
Relationship between incision size and pain intensity
Owing to the different surgeries and different indications, the port sizes were not equivalent. The majority of patients reported minimal laparoscopic port-related pain. The mean VAS score (95% confidence interval [CI]) at 24 hours postoperation with 5-mm port sites was 17.63 ± 13.8 (range, 13.27–21.99), with 10-mm port sites was 26.95 ± 16.66 (range, 23.29–30.61), and with 15-mm port sites was 34.81 ± 18.81 (range, 30.53–39.07). The VAS score (95% CI) markedly declined at 72 hours and was 2.98 ± 6.76 (range, 0.84–5.11), 6.90 ± 9.50 (range, 4.81–8.99), and 10.21 ± 7.05 (range, 8.61–11.81) for 5-, 10-, and 15-mm port sites, respectively.
The group of patients with larger port sizes showed a significantly higher score on the VAS than that shown by the group of patients with smaller port sizes (at 24 hours, the differences in the VAS scores were 17.17 [P = .000] between 15- and 5-mm port sizes, 9.32 [P = .018] between 10- and 5-mm port sizes, and 7.85 [P = .016] between 15- and 10-mm port sizes. At 72 hours, the values were 7.23 [P = .000], 3.93 [P = .042], and 3.31 [P = .039], respectively). The score elevated as the size of the incision increased, and the difference was statistically significant (Table 2 and Figs. 2 and 3).

Difference between the incision size, incision distribution, and pain intensity 24 hours after operation. VAS, visual analogue score.
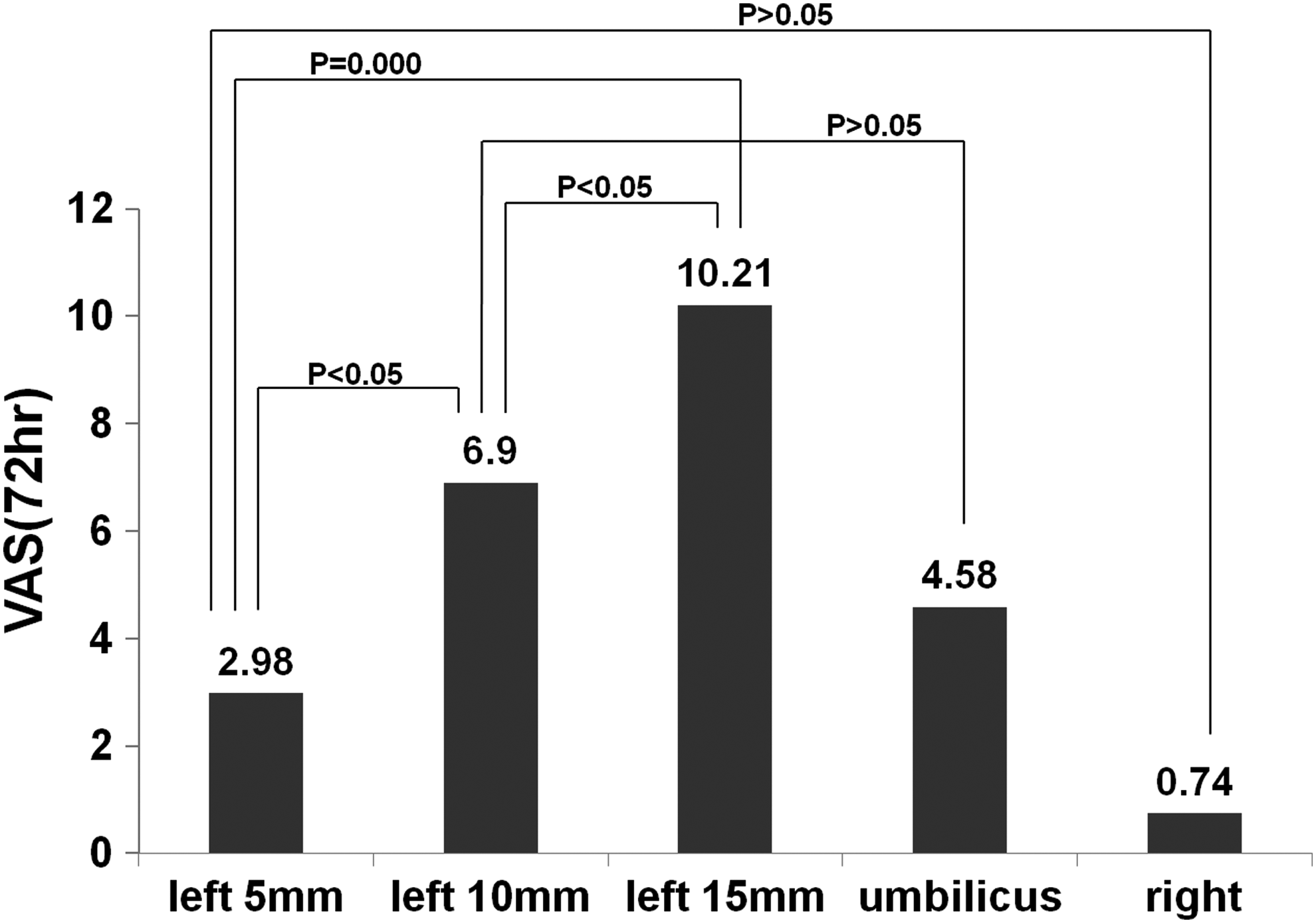
Difference between the incision size, incision distribution, and pain intensity 72 hours after operation. VAS, visual analogue score.
15–5 mm.
10–5 mm.
15–10 mm.
Left 10 mm–umbilicus 10 mm, only according to 82 paired ports of the same (10 mm) size.
Left 5 mm–right 5 mm, only according to 41 paired ports of the same (5 mm) size.
CI, confidence interval; VAS, visual analogue score.
Relationship between incision distribution and pain intensity
At 24 hours postoperation, the trocars placed in the left lower abdomen caused significantly more pain than the pain caused by umbilical trocars with the same (10 mm) incision size (P = .013); moreover, the VAS scores were also higher in patients with left lower abdominal incisions than in patients with right lower abdominal incisions of the same (5 mm) size (P = .041). At 72 hours, the pain in the left lower abdomen with the 10-mm port size was still more severe than that in the umbilicus, but the difference was not statistically significant (P = .162). The difference between the left and right lower abdominal incisions was also statistically insignificant (P = .081) (Table 2 and Figs. 2 and 3).
Other port-specific characteristics associated with pain intensity (focusing only on the 200 ports located in the left lower abdomen)
The extraction port site showed a significantly higher VAS score at both 24 and 72 hours postoperation (P < .05). There were no statistical differences between the type of suture used for abdominal fascial closure and the surgical tapes (P > .05) (Table 3).
CI, confidence interval; VAS, visual analogue score.
Baseline characteristics associated with pain intensity (focusing only on the 200 ports located in the left lower abdomen)
Surgical time and the existence of previous abdominal surgery were significantly associated with the 72-hour pain intensity. However, other factors such as BMI, emergency or elective nature of the surgery, and patient age and educational background showed no significant differences (P > .05) (Table 4).
BMI, body mass index; CI, confidence interval; VAS, visual analogue score.
The factors with P < .1 at 24 and 72 hours (24 hours: incision size, specimen extraction, 72 hours: incision size, specimen extraction, operative time, previous abdominal surgery) were included in a multivariate analysis. It showed that only incision size was a significant predictor of pain intensity 24 hours after the operation (P = .045), and the pain increased with increase in the incision size. Specimen extraction with P = .063 did not reach statistical significance at 24 hours after the operation. At 72 hours after the operation, factors such as incision size (P = .073), specimen extraction (P = .653), operative time (P = .497), and previous abdominal surgery (P = .101) showed no significant differences using adjusted analysis techniques.
Discussion
The American Pain Society defines pain as “an unpleasant sensory and emotional experience with actual or potential tissue damage or described in terms of such damage.”2,3 The persistence of wound pain related to gynecological laparoscopy remains a significant health concern.
The ranges of interpretations of pain have led to the development of various measurement tools that address the different components of pain. Based on established criteria, the VAS was found to be methodologically sound, conceptually simple, easy to administer, and unobtrusive to the respondent. 24 Thus, the VAS seems to be the most suitable for measuring the intensity of pain after surgery. 25 Because pain is a subjective finding, patient self-reporting is the best indicator of pain. Thus, this study deliberately used the pain assessment of individual patients to act as their own control. The clinician only recorded the VAS score, which reduced observer bias.
To our knowledge, this study is the first to numerically assess the pain related to each port site by using different port sizes (5 mm/10 mm/15 mm) and distributions in gynecological laparoscopy. In this study, the pain at 600 port sites in 200 patients at 24 and 72 hours after multiport laparoscopic procedure was prospectively assessed. The present analysis provides detailed and specific quantitative assessment of the impact of individual laparoscopic ports on pain, using validated scores. Using this score, port-specific pain was found to increase proportionally to the incision size.
It was also observed that the umbilical incision was less painful compared to the left lower abdominal incision of the same size, and 5-mm trocars placed in the left lower abdomen caused more pain than those placed in the right lower abdomen. This difference could be attributed to the lack of nerves and the vertical nature of incision in the umbilicus, and the asymmetric location of the left and right incisions (one at the reverse McBurney point and one at the midclavicular line) because of different nerve distributions. Specimen extraction could be another adverse factor, which may cause more tissue damage. A very low incidence of adverse outcomes was observed using 5-mm trocars.
Anesthetic agents have been widely used to diminish pain after surgery in the ports. 1 However, in our study, we excluded patients who preoperatively opted for analgesia pump after operation or requested local anesthesia during the operation period, to exclude the potential bias of anesthesia, and then discussed the internal factors that affect port-specific pain after laparoscopy. Owing to the short half-time of the painkillers, their use within 12 hours after operation would not have affected the evaluation. However, 2 patients who asked for painkillers close to the assessment time were excluded from the study to avoid any bias.
In addition, the duration of surgery and a history of abdominal surgery significantly affected the 72-hour pain intensity. The increase of port use and instrument manipulation was identified as a pain-modifying factor, and the experience and memory of pain from an incision made in a previous operation may have led to excessive attention to the impending incision pain.
It is well known that incision length is the most important determinant of pain.4,5,12 Several investigators have reported attempts to reduce port size and number in nongynecological surgical subspecialties, addressing the supposed advantages and potential risks versus the conventional laparoscopic approach.6–10,23,26,27 After downsizing either all ports or only accessory instruments, many authors reported better results than those obtained using standard procedures, demonstrating less postoperative pain, faster recovery, and more desirable cosmetic outcomes.4,5,12 The rationale is that smaller instruments, which need smaller incision, cause less abdominal wall trauma and, consequently, reduce the stress response to surgery and postoperative pain. 3
Some studies also reported that there are other interacting factors besides incision length that contribute to continuing pain, such as patient age and fascial closure.28,29 Specimen extraction site and emergency surgery can also be other predictors of adverse outcome, as reported in some articles.12,30,31 However, these studies were focused not only on port-specific pain but also on introducing new technologies. Moreover, studies in gynecological surgical subspecialties are rare.
Some previous studies1,32 have reported several other options to reduce port-specific pain after laparoscopy, including the use of nonsteroidal anti-inflammatory drugs, pre-emptive infiltration of local anesthetics, CO2 drainage, low-pressure CO2 pneumoperitoneum during the procedure, heated gas, and nitrous oxide pneumoperitoneum or intraperitoneal saline irrigation. The effectiveness of some of these methods has been reported, but none of these has been recommended as the standard of care.
This study is a prospective cohort using validated pain scores and blinded assessments, including some covariables such as surgical facts (e.g., abdominal wall closure suture, extraction technique, use of surgical tapes, emergency or elective type, surgical time) and baseline characteristics (e.g., patient age, education background, BMI, previous abdominal surgery), but may not include all covariables (such as marital status, contraceptive use). Besides, our study still had several limitations.
First, postlaparoscopy pain has a multifactorial etiology. Besides the pain of incisional trauma at trocar sites, factors such as phrenic nerve irritation, residual pneumoperitoneum, direct tissue trauma from electrocoagulation, or mechanical injury have been advocated as possible additional determinants.2,3
Second, after a 24-hour assessment, the dressing was removed and patients realized the difference between the sizes of each port, which might have influenced the result at the 72-hour time point.
Third, as this trial was an observational study of all kinds of benign laparoscopic gynecological procedures, we could not select the type of operations, so the number of the three different left ports was not equivalent and randomized.
Fourth, in this study, all surgeons belonged to the same surgical team, were right handed, and were positioned to the patient's left. Moreover, the trocar placed in the left lower abdomen was the closest to the surgeon among the 3 trocars; since it undertook the main manipulation task (needle introduction, instruments exchanging, etc.), it may have caused more tissue damage and abdominal wall trauma (although the workload of each trocar was difficult to quantify). Furthermore, the asymmetric nerve distribution may have accounted for the differences in the VAS scores. We did not consider other situations (e.g., with the surgeons standing on the opposite side of the patient or those operating with the left hand); further studies are required to assess the effects of these factors.
Finally, although we mainly focused on the incision size, the presence of heterogenic diseases and operation procedures may also cause potential bias, and owing to the small sample size in our study, the single-center experience might have decreased the reliability of the results.
Conclusions
According to our evidence, port-specific pain mostly depends on incision size and distribution, and therefore, based on our findings in the present study, we think that choosing umbilicus for specimen retrieval and using smaller ports, especially 5-mm trocars for major operation ports in patients undergoing benign gynecologic surgery with three ports (varying at the left port from 5 mm to 10 mm to 15 mm), would lead to better outcomes by causing less postoperative port-specific pain and would increase patient comfort after surgery.
Footnotes
Acknowledgment
This study was supported by grants from the Natural Scientific Foundation of Zhejiang Province (No. LQ16H160018).
Disclosure Statement
No competing financial interests exist.