
Abstract
Abstract
Introduction:
Surgery for liver metastases in pancreatic neuroendocrine tumor (PNET) improves overall survival rate. We present the first case report for robotic multivisceral resection of distal pancreas, spleen, and left liver for metastatic PNET.
Materials and Methods:
We present a case of 52-year-old female diagnosed with PNET in the pancreatic neck metastatic to the liver, responding to somatostatin and bland embolization, who underwent surgical debulking using da Vinci robotic platform. Intraoperative Doppler ultrasound was used to define the vascular distribution and tumor extension. The parenchymal liver transection was performed with vessel sealer. The distal pancreas and the spleen were approached medial to lateral and resected in an en-bloc fashion. The left liver inflow, outflow, and splenic artery and vein were transected with vascular stapler device.
Results:
Da Vinci robot-assisted multivisceral resection has been performed with good postoperative outcome. Operative time was 369 minutes and the estimated blood loss was 100 mL. The patient had a short hospital stay with quick recovery and good outcome at 5 months follow-up after the surgery.
Discussion:
Liver metastases in PNETs are considered an adverse factor. Aggressive surgical management is a mainstay. The laparoscopic approach to pancreatic or hepatic surgery is difficult in inexperienced hands with steep learning curve. The recent robotic system seems to overcome many limitations. This is the first case of robotic multivisceral resection for synchronous liver metastasis from PNET. Concurrent primary tumor resection with hepatectomy offers potential curative intention.
Introduction
P
Because of the nonspecific and intermittent nature of their symptoms, diagnosis of the neuroendocrine tumors is often delayed for months to years, even in functional tumors. 6 Approximately 75% of patients with neuroendocrine tumors have metastatic disease at presentation. After the lymph nodes, the liver is the predominant site for neuroendocrine tumor metastases. Synchronous liver metastasis, present in 75%–80% of patients, is a key adverse prognostic factor. 7 Primary hepatic neuroendocrine tumors are extremely rare, and are diagnosed by exclusion of other primary tumors.
Whereas, the 5-year survival rate of pancreatic adenocarcinoma is 5%–10% after curative resection, long-term survival is not uncommon for patients with PNETs, particularly nonfunctioning tumors.8,9 Patients who have undergone resection have been reported to have a decreased likelihood of future metastasis and disease-specific death compared with patients who did not undergo resection.10,11 When it is feasible, aggressive surgical management of both the primary tumor and liver metastases improve survival rate extensively.10,12,13,14
The minimal invasive surgical approach to pancreatic neoplasm leads to many benefits, including recovery cosmetic results, lower perioperative complication, early access to adjuvant therapies, and psychological implication. 15 After the first robotic distal pancreatectomy reported by Melvin et al. 16 in 2003, robotic surgical systems exhibit several advantages over conventional laparoscopic instrumentations. 17 Recently, articles also have proven that the robotic liver resections could be an advantageous technique that may facilitate accurate tissue resection of lesions adjacent to major vessels, close to the liver hilum, or in difficult anatomic positions. 18 However, the poor oncologic prognosis of patients affected by malignant tumor represents an important incentive to adopt some minimally invasive operation that is able to minimize the perioperative comorbidity. 19
In the early stage of learning curve, the only robotic extended resection procedure done so far is for pelvic exenteration. To the best of our knowledge, this is the first totally robotic multivisceral resection for liver metastasis in PNET ever reported in the medical literature, describing the surgical technique, short-term oncologic outcomes with literature reviews.
Materials and Methods
We are presenting a case of a 52-year-old female who was diagnosed with a nonsecretory neuroendocrine tumor of the pancreatic neck metastatic to the liver of intermediate grade.
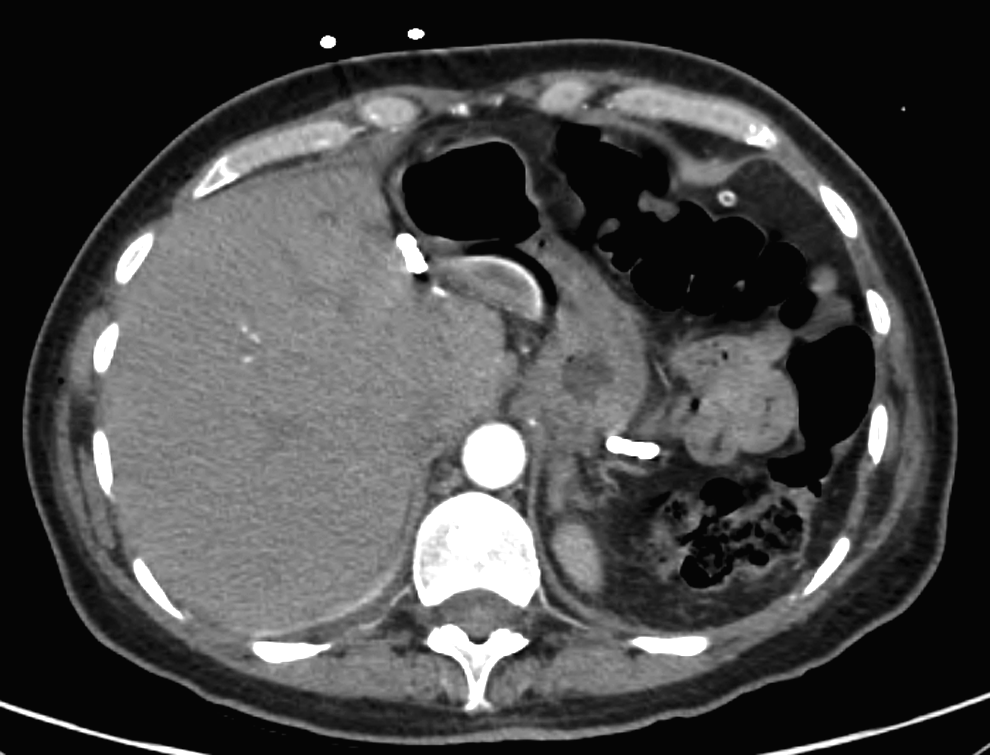
A 5 cm mass in the left liver lobe and a pancreatic neck mass with secondary pancreatic duct dilatation of the body and tail were incidental findings on a CT scan of the abdomen and pelvis that was performed as a workup for recurrent urinary tract infections (Fig. 1A). The patient then underwent a CT-guided liver biopsy that was consistent with well-differentiated neuroendocrine tumor of intermediate grade with one mitoses per high-power field. Immunohistochemical stains were performed and were positive for synaptophysin, chromogranin, and SATB2 and negative for CK7, CK20, CDX2, and CAD17. The quantitative MIB1 was consistent with 6% proliferative activity. This immunohistochemical profile is consistent with a metastatic well-differentiated neuroendocrine tumor of intermediate grade. The PET scan confirms the hypermetabolic activity of the lesions from the pancreas and the liver (Fig. 1D–F).
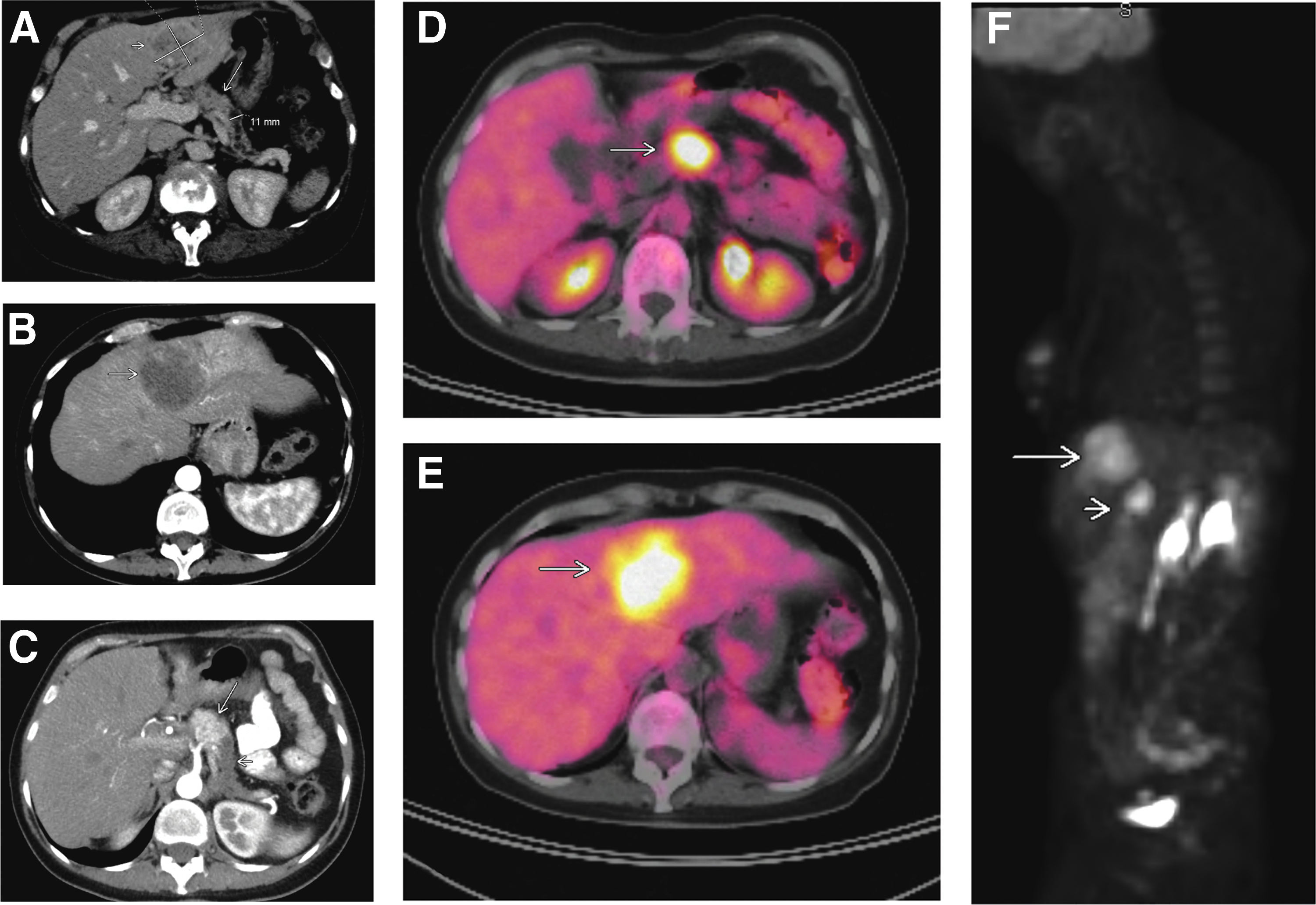
Preoperative imaging.
The patient was started on sandostatin and received one successful session of bland embolization of the hypervascular liver mass with 100 μm particles (Embozene) through selective catheterization of the left hepatic artery, which she tolerated well. The follow-up CT after 1 month had shown stable-size lesion of the left hepatic lobe, however, the vast majority of this lesion has become centrally necrotic. There were no new lesions identified within the liver (Fig. 1B, C). As there was no evidence of progression of the disease and the patient responded well to embolization, we offered the patient the option for surgical debulking by robotic distal pancreatectomy and left hemihepatectomy.
Her medical history is relevant for newly diagnosed diabetes mellitus type 2 without known end-organ sequelae, with hemoglobin A1c of 6.5%, remote duodenal ulcer bleed with history of blood transfusion, recurrent urinary tract infections on chronic nitrofurantoin therapy. The past medical history is notable for open umbilical hernia repair, and bilateral tubal ligation, bilateral breast fibrocystic disease BIRADS 2 with biopsy negative for cancer. She is a former smoker.
The vitals on the day of preoperative evaluation were as follows: Temperature 98.5°C, pulse 83 beats/minute, respirations 18/minute, blood pressure 131/81 mmHg, height 171 cm, 71.8 kg, O2 saturation 100% on room air, body mass index of 21.1. She is a youthful-appearing 52-year-old in no acute distress. The general physical exam was normal and there were no signs of obstructive jaundice or cirrhosis. All the preoperative laboratories, including CBC, CMP, and coagulation panel were within normal ranges. Sandostatin intramuscularly was administered once a month since the time of diagnosis. She also received prophylactic immunization against meningococcus, Haemophilus, and Pneumococcus as splenectomy was a part of the surgical plan.
Patient position and port placement
The patient was placed on the operative table in supine position, sequential compression devices were applied on both legs and general anesthesia with orotracheal intubation was achieved without difficulties. She received prophylactic antibiotics. For purposes of hemodynamic monitoring she had a radial arterial line placed. A Foley catheter and a nasogastric tube were also placed in after anesthesia. Both arms were then tucked to sides and all the pressure points were padded. The patient was secured to the operating table using the Pink Pad—Pigazzi Patient Positioning System with strips across the chest and mid-thigh. The abdominal area was prepped with chlorhexidine from mid thigh to the nipples and from table to table and draped sterile to expose an operative field between pubis and xiphoid and between the two axillary lines.
Pneumoperitoneum was achieved through a Veress needle in the superior umbilical crease and the abdomen was insufflated to 15 mmHg. We have used two plastic 12-mm trocars and four metallic 8-mm trocars. One of the two 12-mm single-use trocars was placed one in the superior umbilical crease and the other one on the right side at the level of the umbilicus slightly medial from the midclavicular line. These two trocars were used for camera and assistant port instrument as it follows further in description.
Four additional metallic 8-mm trocars were placed for the robotic arms and assistant instruments. Two of these were placed at the level of the umbilicus, on the lateral extreme, about 1 cm above from the peritoneal reflection from the ascending and descending colon on the right side and left side, respectively. They were placed under vision with care to avoid colon injury. On the outside, they would correspond approximately to the midaxillary lines. The other two were placed on the midclavicular line at the level of the umbilicus on the left side and on the anterior axillary line about 2 cm below the horizontal line through the umbilicus on the right side (Fig. 2A–C).
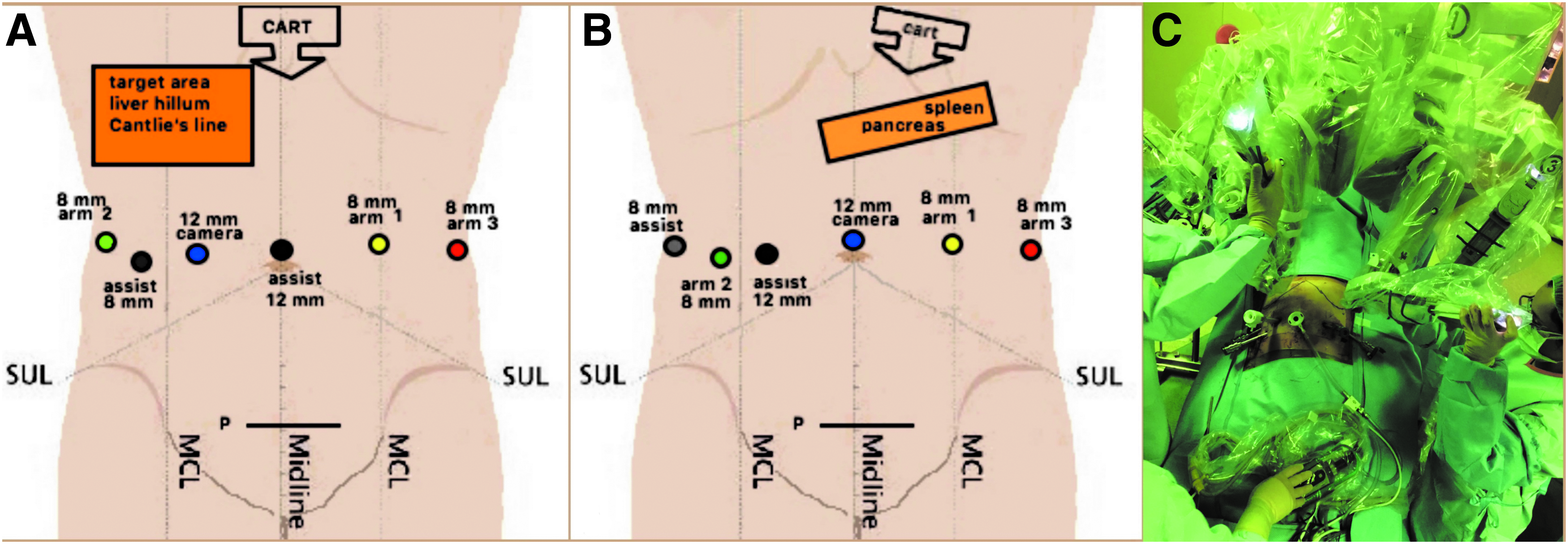
Robotic docking.
Robotic hepatectomy
The robot was docked from head initially for hepatectomy. We have docked the camera in the midclavicular line at the level of the umbilicus, then arms 1, 2, 3 on the left midclavicular line, right midaxillary line, and left mid-axillary line, respectively, all being at the level of the umbilicus (Fig. 2A). Using fenestrated bipolar forceps and permanent cautery hook, we divided the round ligament and transected the falciform ligament toward the coronary ligament. We then transected the right side of the coronary ligament corresponding to segment 4b, and the left side of coronary ligament following the left triangular ligament, so that the whole left liver was mobilized and inferior vena cava was exposed above the liver. Cadiere forceps in arm 3 was used for additional exposure and retraction.
The intraoperative Doppler ultrasound was used to identify the inflow and outflow for the left liver. The liver hilum was dissected and the left hepatic artery was followed along the left portal vein. The hilar dissection was continued within the liver plate at the point of entrance of the vessels in the liver (Fig. 3A). The middle and left hepatic veins were identified with intraoperative Doppler ultrasound and the superior surface of the liver was scored with the hook from the inferior vena cava to the anterior liver margin following Cantlie's line to delineate the future transection line between segment 4 and 5. The dissection line was kept in the line of the middle hepatic vein. The vessel sealer and the fenestrated bipolar forceps were used to transect the liver parenchyma along the previously scored line down toward the liver hilum (Fig. 3B).
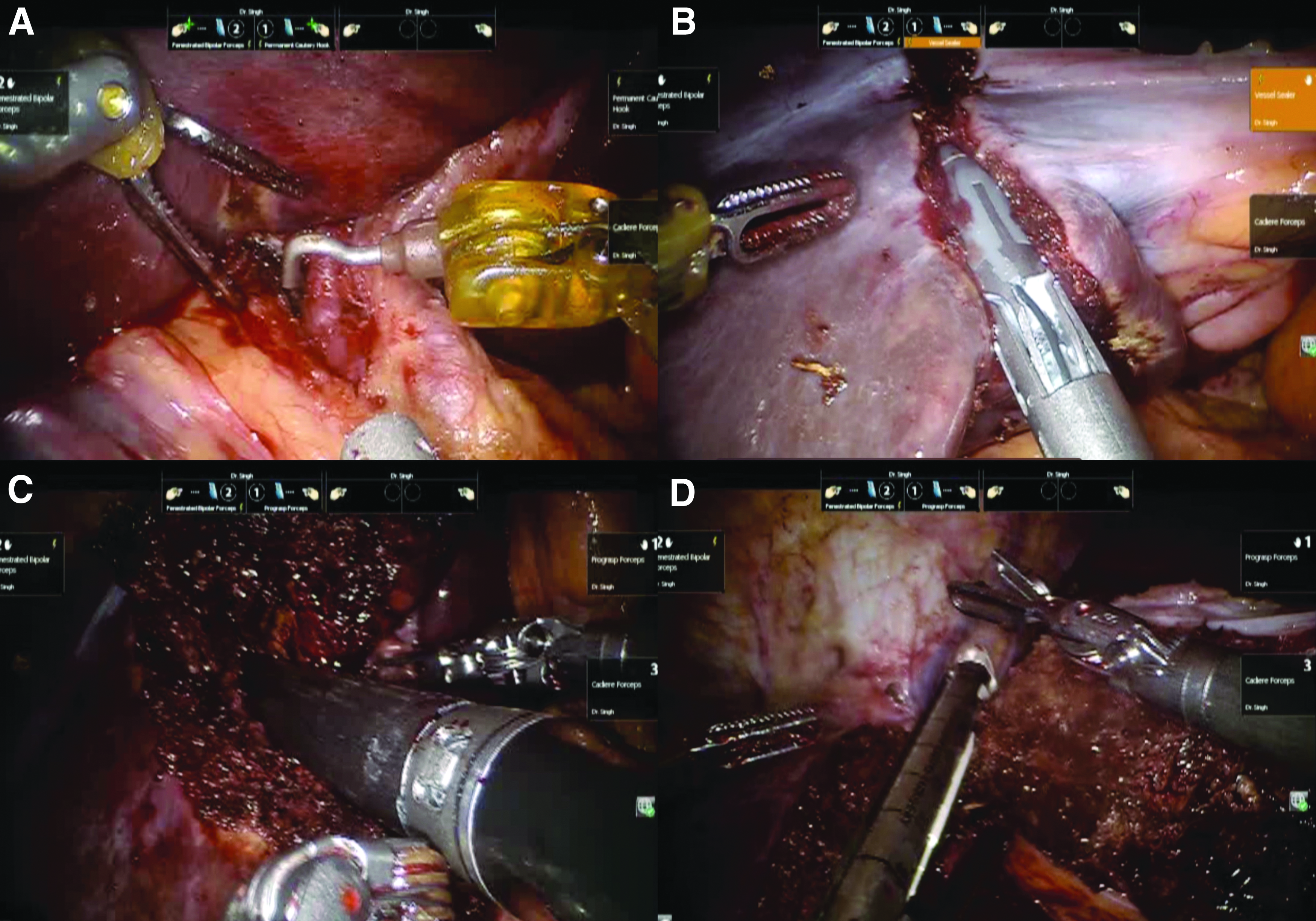
After confirming the left portal branch, left hepatic arteries and left biliary duct, a white vascular load cartridge of a 60 mm Ethicon stapler was fired across these structures (Fig. 3C). Another white vascular load cartridge of a 60 mm Ethicon stapler was then used to transect the middle hepatic vein and the left hepatic veins (Fig. 3D). Estimated blood loss was about 50–70 mL. The remnant liver appeared to be healthy. Over the transection line, there was no bleeding or bile leak.
Robotic distal pancreatectomy
We then repositioned the patient in steep reverse Trendelenburg with 30° left side up. The camera port was docked at the umbilical trocar, and the three arms were placed as follows: arm 1 on the left midclavicular line, arm 2 right anterior axillary line, and arm 3 on the left midaxillary line, all being at the level of the umbilicus (Fig. 2B, C). The ProGrasp forceps was used in arm 3 for the entire surgical step to serve mainly for retraction of the stomach. The other instruments used were Cadiere forceps, fenestrated bipolar, hook, scissors, large suture cut needle driver that were alternating between arm 1 and arm 2.
The lesser sac was entered by dividing the gastrocolic and gastrosplenic ligament with fenestrated bipolar forceps and vessel sealer with care to keep the gastroepiploic vessels on the stomach side and to avoid colon injury. The anterior surface of the pancreas was exposed and the tumor immediately became apparent. Using the hook and the fenestrated bipolar forceps we dissected circumferentially the splenic artery on the upper border of the pancreas, then we detached the pancreas from the transverse mesocolon on its lower border and we identified the superior mesenteric vein. This was followed under the pancreas and a tunnel was finally created between the pancreatic neck and portal vein and a vessel loop was placed around the pancreatic neck for traction. The dissection was then carried out along the upper and lower margins of the pancreas toward the spleen.
After confirming the transection line by ultrasound, a 60 cm Ethicon 60 white vascular load cartridge stapler was used to transect the pancreas (Fig. 4A). There was minimal bleeding from the left coronary vein, which was avulsed from the left side of the portal vein. Hemostasis was achieved with the vessel sealer. Once the splenic vein and splenic artery were dissected from the retroperitoneal plane, an Ethicon 60 white vascular load cartridge stapler was used to transect these vessels (Fig. 4B).
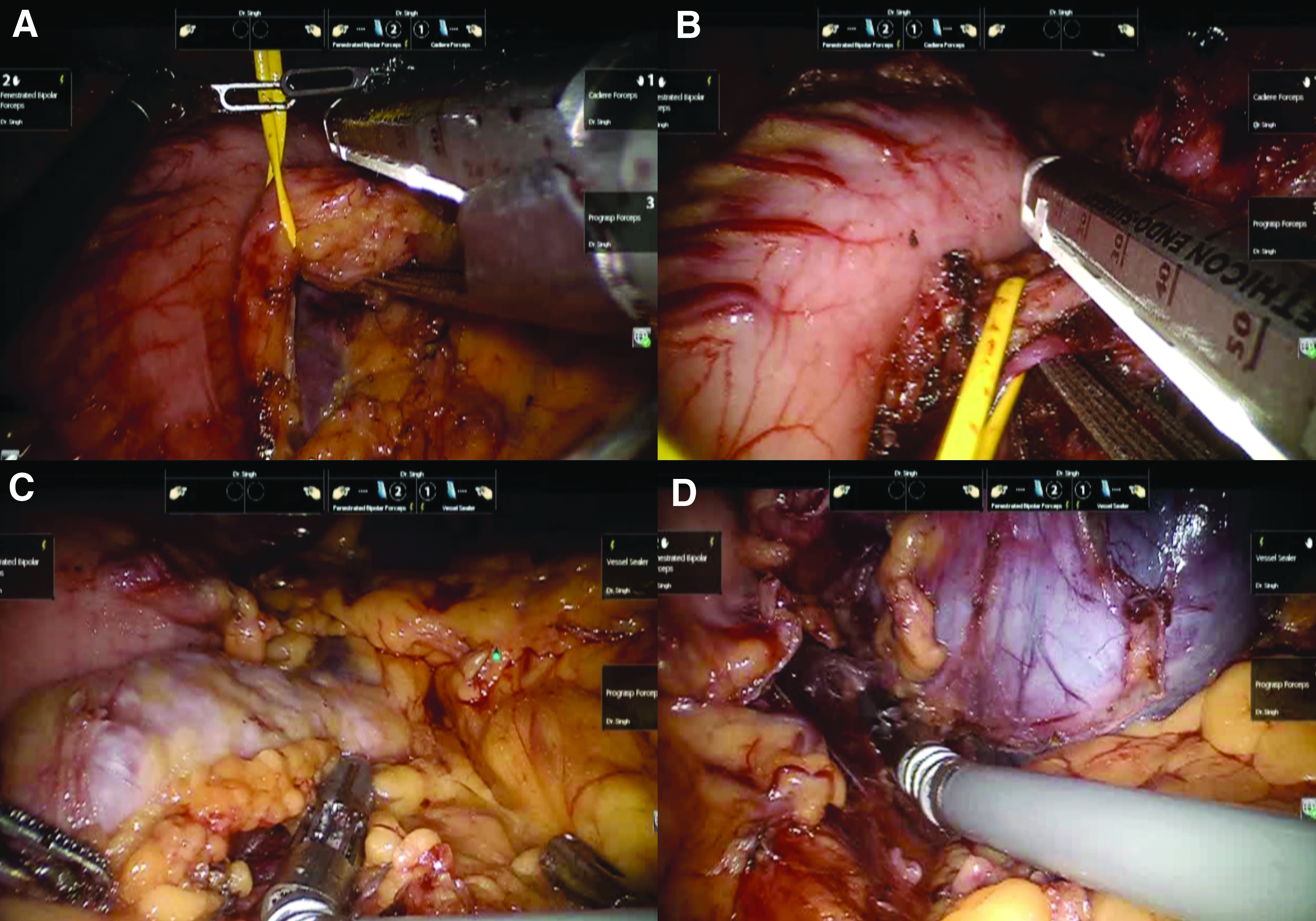
The tail of the pancreas was detached with the medial-to-lateral approach toward the spleen (Fig. 4C). The splenic flexure was mobilized appropriately and the spleen was dissected free from its ligaments with the vessel sealer (Fig. 4D). The specimen consisting of liver and distal pancreas was placed in an extractor bag and was extracted through a 3 cm Pfannenstiel incision. A drain was sutured proximal to the pancreatic stump with 4-0 catgut chromic and was exteriorized through the left midaxillary trocar. Another drain was placed in the transection surface of the liver and was exteriorized through the right midaxillary line trocar.
The total operative time was 369 minutes and the estimated blood loss was 100 mL without necessity of blood transfusion. She tolerated the procedure well. Postoperative course was uneventful with the exception of an episode of supraventricular tachycardia that responded to medication. A CT angiogram of the chest was done and pulmonary embolism was ruled out. On the same CT scan, the liver transection line appeared intact and there were no intraabdominal collections (Fig. 5). She received prophylactic anticoagulation with low molecular weight heparin started in the morning of postoperative day 1. She had minimal pain at the incision sites and she was fully mobilized on postoperative day 1. The epidural, opioid-based patient-controlled analgesia was discontinued on postoperative day 2 and was replaced with oral narcotic-based analgesics that were sufficient in minimal doses.
CT scan done immediately postop reveals no intraabdominal collections or other postoperative complications.
The outcome of the minimally invasive approach with extraction of the liver, distal pancreas and spleen through a small Pfannenstiel incision and the excellent cosmetic advantage was very well appreciated by the patient (Fig. 6). Clear liquid diet was started on postoperative day 1 and by discharge she was tolerating regular low fat diet. She was discharged home on postoperative day 4. The liver drain was removed 2 weeks postop and there was no biliary leak and the pancreatic drain was removed at 7.5 weeks postop, as there was a mild pancreatic leak that subsided without intervention other than low-fat diet. Pathological findings confirmed the diagnosis (Fig. 7).

The incisions used for the minimally invasive approach. Postoperative day 2.
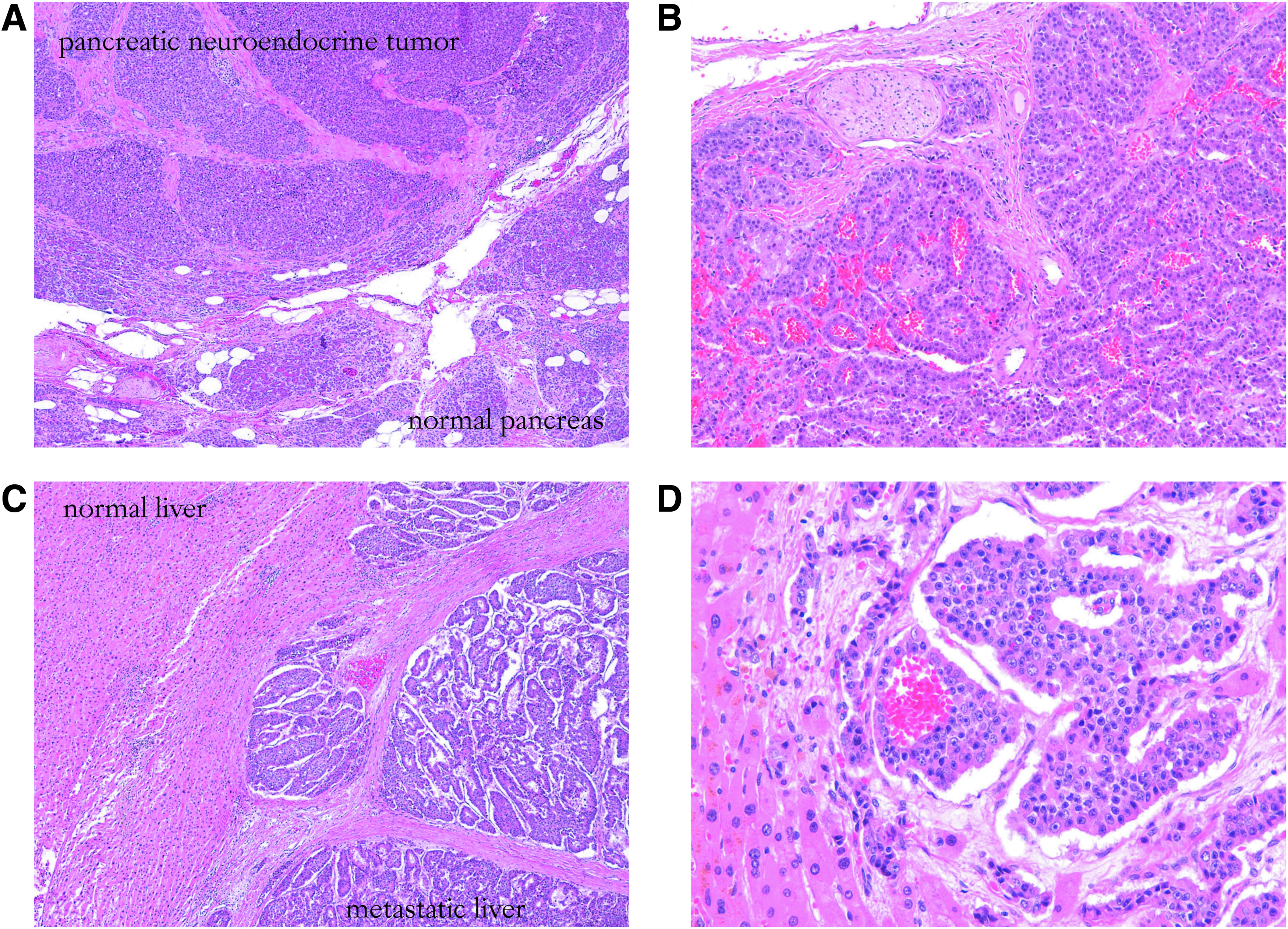
Pathological findings.
Discussion
PNETs are a rare subset of pancreatic tumors, accounting for 1%–2% of all pancreatic tumors. 2 The overall incidence of neuroendocrine tumors is estimated to be 1–1.5 per 100,000 in the general population, leading to an overall 2500 cases per year in the United States. 1 Autopsy series have reported an incidence of 0.5%–1.5%.2,20 The tumors have a peak incidence at age 30–60 with no gender preference. 2 The incidence of neuroendocrine tumors has markedly increased over the course of 15 years. Metastases were found in 20.8% at presentation and in other 38% after the initial diagnosis. 21 After lymph node, liver is the predominant site for metastasis. Seventy percent to 80% of patients with liver metastasis are considered to be nonsurgical and are treated with palliative intent. 22 Patients who have undergone resection have been reported to have decreased likelihood of future metastasis and disease-specific death compared with patients who did not undergo resection.13,23 However, the role of cytoreductive surgery in this situation is controversial.10,26
Currently, there are many therapeutic options for metastatic NETs. This includes surgery (open resection, laparoscopic resection, robotic resection, and liver transplant), medical intervention (e.g., chemotherapy, biotherapy with somatostatin analogues and interferon, thermal ablative techniques [radiofrequency ablation, microwave ablation, and cryotherapy]), and embolization. Although there is no evidence-based data directly comparing surgical versus alternative liver-directed treatment options, the mainstay treatment for PNETs is surgical resection.7,27–30 Even though numerous uncontrolled studies provide evidence that surgical resection may improve symptom control and longer survival time, no result is proven at present.25,27,31 Nevertheless, because of the low efficacies of other tumor treatments, most conclude that surgical resection should be attempted in any patient with malignant PNETs if at least 90% of visible tumor could be removed.25–28,31
The 5-year recurrent rate is more than 80% and up to 80%–90% occurs as hepatic metastases, followed by bone, lung, and lymph node.10,13,24,32 Sakurai et al. reported a case of a 34-year-old male with long-term survival for open multiple visceral resection. The patient was diagnosed with PNET and multiple liver metastases. After chemotherapy reduction with etoposide and cisplatin, the patient underwent open approach for pylorus preserving pancreatoduodenectomy with partial colectomy and partial hepatectomy. Three months after the surgery, multiple liver metastases were recurrent in segments 3, 5, 6, which were resolved with TACE. The patient has been well for 14 months since the operation. 33
Sarmiento et al. retrospectively analyzed 23 cases undergoing open approach distal pancreatectomy, splenectomy, and concurrent hepatectomy. There were six major and 17 minor resections with complete gross resection (R0/R1) in nine patients and debulking resection (R2) in 14 patients. Overall, progression-free and symptom-free survival was 71% (median: 76 months), 5% (median: 21 months), and 24% (median: 26 months), respectively, at 5 years. These data advocate aggressive concurrent resection when it is feasible. 34 NANETS, European and Japan guidelines recommend liver resection for stable and localized PNETs as extensive liver metastasis progression is frequent and is the major cause of death.28–30 However, concurrent hepatic resection with primary resection is still controversial due to limited patient volume. 34
Minimally invasive surgery has tremendously changed the approach to patients affected by pancreatic neoplasm. 35 Similarly laparoscopic hepatectomy has become a viable alternative to open approach. 36 These laparoscopic procedures have been well described and a vast majority of authors agree that it is a technically challenging procedure with steep learning curve and requiring high laparoscopic skills.35–37 Compared with the conventional laparoscopic surgeries, the robotic surgery is supposed to overcome these limitations: due to the elimination of trembling effect, the clear 3D images, and the EndoWrist™ wrist-stimulating devices with seven degrees of freedom. These provide better solutions for the division of pancreas uncinate process, fine separation between pancreatic mass and surrounding tissues, retroperitoneal lymph node dissection, skeletonization of the structures inside the hepatoduodenal ligament and reconstruction of major vessels.38–40
As a novel technique accompanied by questionable cost productiveness, robotic surgery has not widely popularized, and the only robotic multivisceral resection done so far is pelvic exenteration for pelvic cancer or rectal cancer. Its use has been relatively unexplored, accounting for few reports with limited patient volume.41–43 A recently published case of robotic pelvic exenteration for prostate cancer involving rectum and bladder reported a good short time outcome. 43 Shin et al. analyzed 36 rectal cancers undergoing multivisceral en bloc resection and extramesorectal lymph node dissection robotically. All the resections were R0 and there were no incomplete total mesorectal excisions. The vagina and prostate or periprostatic structures were the most commonly resected. The 5-year cumulative local recurrence rate was 3.6%. 42 Robotic multivisceral resection has been gradually noted with relative good oncologic and perioperative outcomes.42,44,45
The intraoperative Doppler ultrasound was very useful in identification of the arterial and venous vascularization of the liver that facilitated the dissection and guided the proper placement of the vascular staplers. The incidental finding of two left hepatic arteries was in concordance with the interventional radiology report that had mentioned some difficulties in cannulating one of the left hepatic arteries. Also intraoperative Doppler ultrasound was used to identify the boundaries of pancreatic mass and to determine the transection line of the pancreas, as well as to identify the splenic vessels.46,47
We herein present the first case of totally robotic distal pancreatectomy, left hemihepatectomy and splenectomy for PNET with no severe perioperative comorbidity and optimal oncologic outcomes. As the tumor was stable and localized in just pancreas and liver, she was offered surgery with both curative and cytoreductive intent. Even though concurrent resection is still a controversy, our patient was young with good performance status; hence one-stage surgery was a logical option to avoid adhesion, halting disease progression, decreasing physical debilitation and possible aesthetic complications due to multiple operations.
Combined liver and multivisceral resections are rare, complex procedures that demand extensive surgical skills, with not very well defined indications yet, but in carefully selected patients and in experienced hands the postoperative morbidity and mortality rates are acceptable. 48 In a hand of skillful and experienced robotic team, robotic multivisceral resection for PNET is feasible with optimal outcomes in well selected patients.
Conclusion
We believe that robotic multivisceral resection for synchronous liver metastasis in PNET is feasible and the best treatment ever, combining good oncological results and, overall outcomes, together with the advantages of minimal access surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.